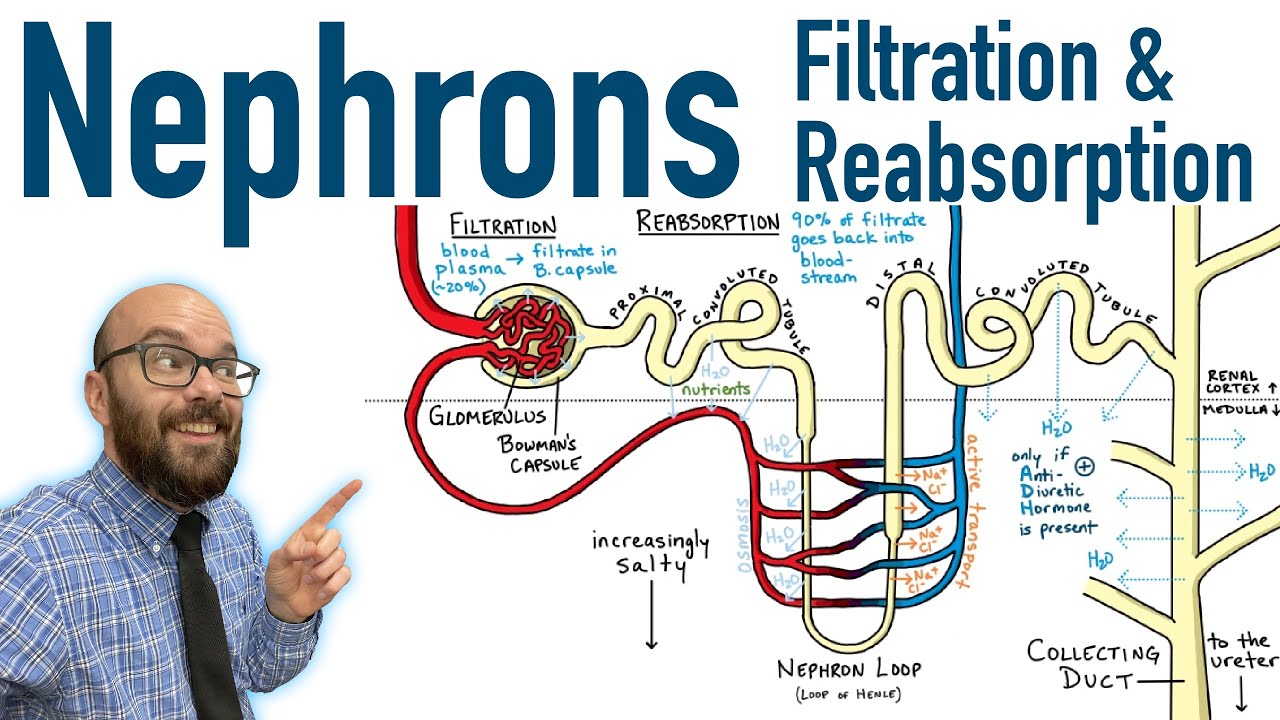
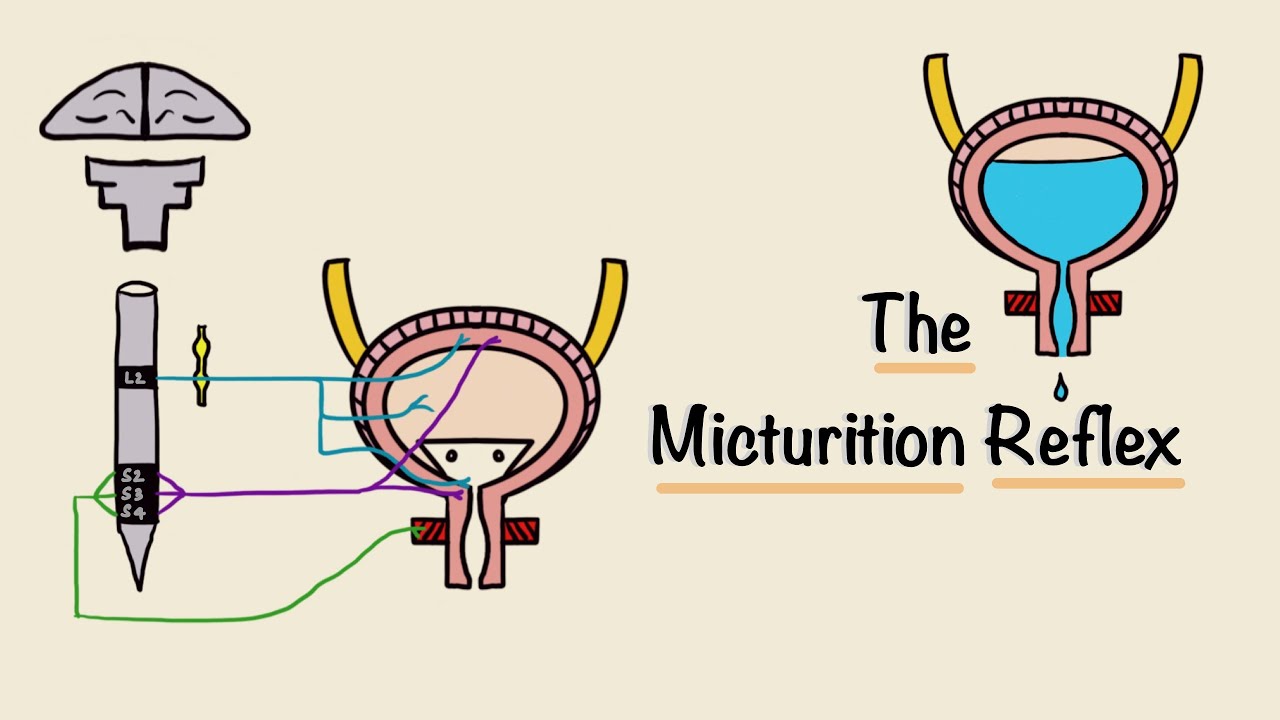
hi everyone welcome to bite size med where we talk about quick bite-size concepts in medicine for study and rapid review this video is on glomerular filtration each kidney has millions of nephrons each nephron has a glomerulus a proximal convoluted tubule the loop of henle the distal convoluted tubule and the collecting duct blood flows through the afferent arteriole into a tuft of capillaries and that's the glomerulus it exits via the efferent arteriole the plasma gets filtered through the glomerulus to form the glomerular filtrate which then passes through the rest of the nephron where processes like reabsorption
and secretion happen followed by excretion the filter when magnified has three layers because it's a capillary it has endothelial cells and a thin basement membrane the endothelial cells are fenestrated so they have spaces the visceral layer of bowman's capsule which surrounds the glomerulus has specialized cells called podocytes and these podocytes have foot processes the foot processes interdigitate creating slit clefts so solutes can pass through the spaces so obviously there's a size restriction only substances that can fit through these spaces can pass but also it's a charge barrier all three layers are negatively charged so even
if a substance is small enough to pass through like albumin if it's negatively charged it will get repulsed and hence can't pass through thus the glomerular filtrate is normally free of plasma proteins the rate at which substances get filtered through the glomerulus is the glomerular filtration rate or the gfr the gfr is dependent on the renal plasma flow more the plasma that flows through the glomerulus more the gfr the fraction of plasma that gets filtered is called the filtration fraction this is given by the ratio of the gfr to the rpf it's usually 0.2 or
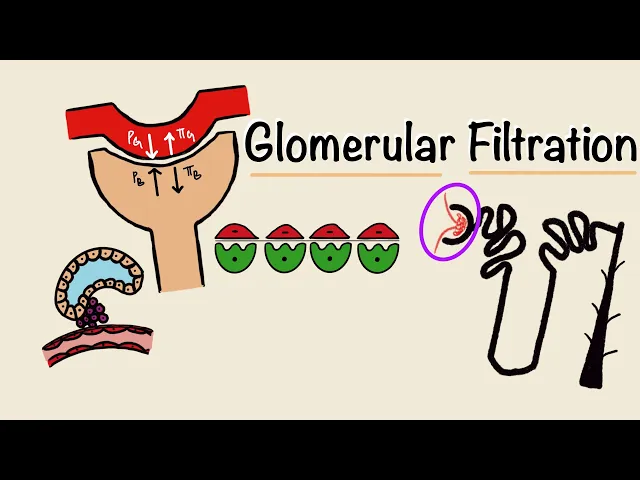
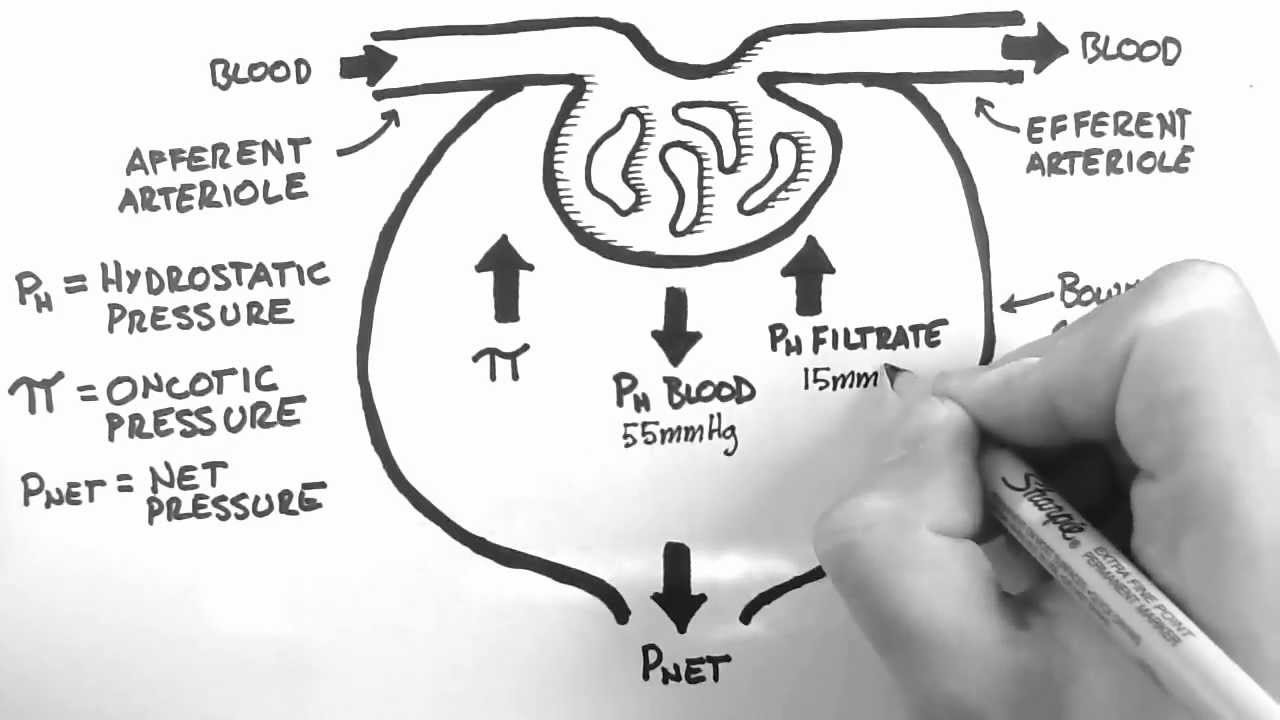
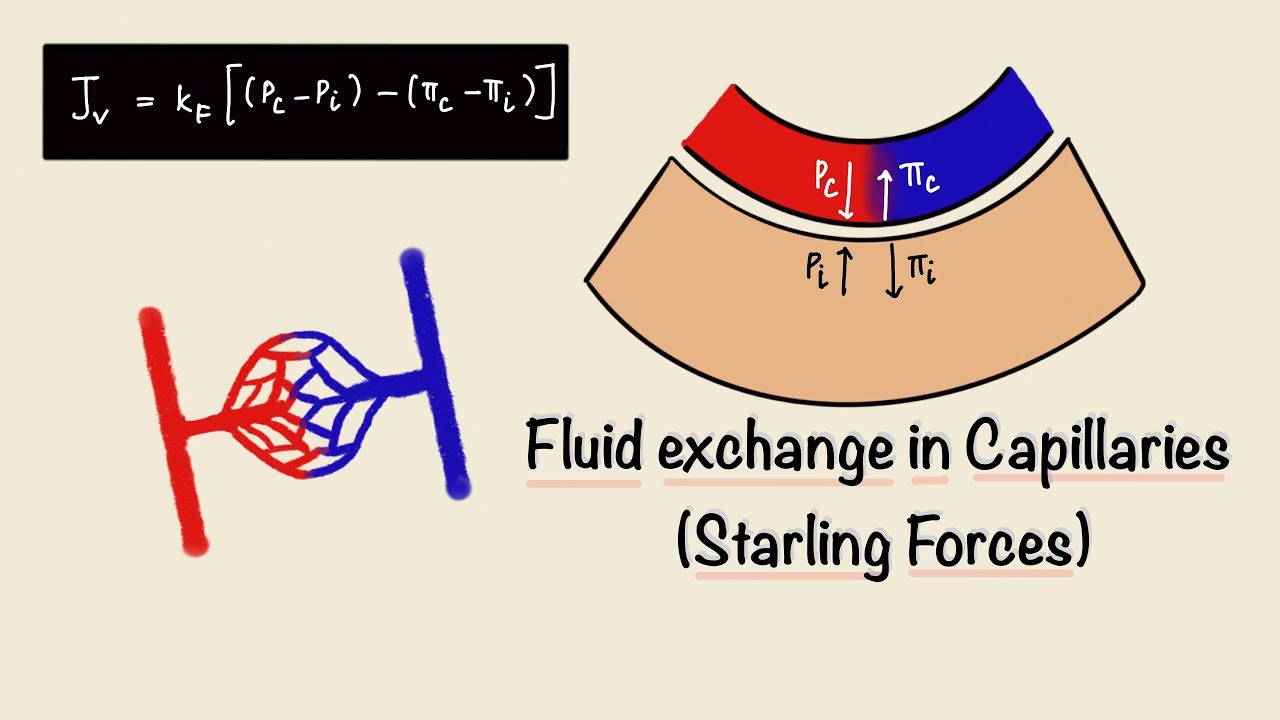
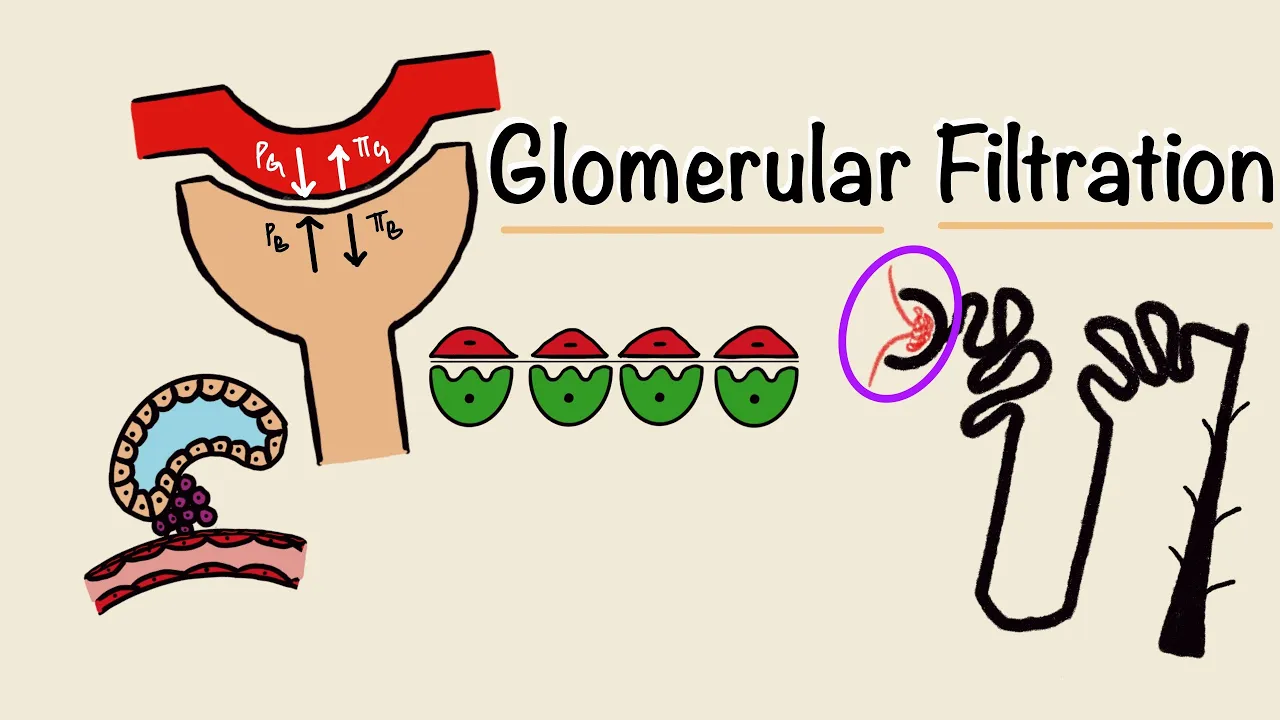
20 percent this means that 20 percent of the renal plasma gets filtered through the glomerulus the glomerulus is a set of capillaries so the forces that determine the fluid movement are startling forces for better understanding of starling forces you can check out my video linked in the description box below there are four starling forces the hydrostatic pressure on either side so in the glomerulus is pg and the bowman space is pb the colloid osmotic or oncotic pressure in the glomerulus is pi g and the bowman space is pi b pg is hydrostatic and it comes
from fluid pressure so it encourages filtration and we're going to put a positive sign next to that pb from the other side opposes filtration so we'll put a negative sign there the colloid osmotic pressures are from proteins proteins pull fluid towards them so pi g opposes filtration and is negative while pi b encourages it so it's positive but since proteins can't cross the barrier pi b would be negligible because there's no proteins in the filtrate this whole thing together is called a net filtration pressure the most important force driving filtration is pg the hydrostatic pressure
in the glomerulus is altered by changes in the pressure and resistance of the afferent and deferring arterioles so if the pg reduces the gfr reduces another factor that determines gfr is the kf or the filtration coefficient this is the hydraulic conductivity of the barrier it includes things like surface area and thickness of the basement membrane for permeability so the gfr is the product of kf and the net filtration pressure higher the kf higher the gfr the renal blood flow and the gfr are auto-regulated over a wide range of pressure changes from 75 to 180 millimeters
of mercury so pressure changes in this range alter the gfr in very minute amounts the rbf is regulated by two mechanisms the myogenic mechanism where the blood vessel resists stretching in increased pressure so it maintains a constant renal blood flow and the tubular glomerular feedback this feedback is by the juxtaglomerular apparatus which includes three things the macula densa of the early distal tubule the extra glomerular mesangial cells and the juxtaglomerular cells of the afferent arteriole the macular densa senses flow rate and the changes in the sodium chloride concentration in the early distal tubule if it
senses a low sodium chloride concentration it stimulates the jg cells to produce renin renin converts angiotensinogen to angiotensin 1 and by the angiotensin converting enzyme angiotensin 2 is formed which constricts the efferent arteriole and reduces the renal plasma flow but increases the gfr by increasing the hydrostatic pressure in the glomerulus if it senses a high sodium chloride concentration it directly acts on the afferent arteriole and constricts it so it reduces the renal plasma flow and hence the gfr the gfr can be measured by measuring clearance and you can check out my video on clearance that
i've linked in the description box below clearance is the rate at which a substance is cleared from the plasma per unit time it's given by the urine concentration of a substance into the urine fluoride over the plasma concentration of that substance for gfr we need a substance that gets freely filtered but neither reabsorbed nor secreted and that substance is inulin so gfr is the clearance of inulin but inulin isn't produced in our body so it has to be administered creatinine therefore is an effective substitute even though a small amount does get secreted into the tubules
creatinine clearance can be used to measure gfr as the gfr reduces the creatinine clearance reduces and hence the plasma creatinine rises the gfr can be measured from the serum creatinine by the cockroft gold formula that's 140 minus the age into weight in kilograms over the serum creatinine into 72. that's for males and this whole thing multiplied by 0.85 is for females and that's the glomerular filtration i hope you found this video useful and if you did give it a thumbs up and subscribe to my channel thanks for watching and i'll see you in the next
one