welcome back to the ninja nerd podcast today we're talking about lymphoma it's going to be an awesome episode we're doing two cases one on hotchkin lymphoma and the other one on non hodkin lymphoma but the first one's a surprise you got to try and figure it out I think so I think so I think so all right let's get right into it case one we have a 25-year-old male presents with Progressive fatigue and painless neck swelling for the past 3 months the patient noticed a painless Mass on his right side of his neck which has
slowly enlarged he also reports intermittent low- grade fevers drenching night sweats and unexplained weight loss some b symptoms right there yeah he denies recent infections cough hemoptisis or significant bruising bleeding real quick b symptoms what I thought it was called like constitutional symptoms or yeah systemic typ same thing what what's the be I I don't really know what the bee is actually for body I just wondered I mean it's truly a good question symptoms I never really thought about that yeah you can kind of call them constitutional symptoms but for some reason they kind of
just I don't know if it's because of the B lymphocytes I don't know it's it may be a possible thing like that but I have to look it up uh if you guys know please comment down below' be a good one actually cool to know he doesn't know everything he's not that good no no I'm not man I really am not but yeah I think that constitutional symptoms b symptoms I'm guessing the b symptoms may have something to do with the b lympocytes or something I don't know let's get into it all right heit me
past medical history no significant past medical history no prior history of malignancy no known immuno deficiency he's on no medications his exam vitals bp 125 over 80 hor rate is 85 temp is 37.8 Celsius is O2 sat 99% on rir for his lymph nodes they are firm non- tender right cervical and a supraclavicular lymphadenopathy abdomen no hepatus SPL omegal skin no PTI or emosis we get a whole bunch of labs and a little bit of Imaging as well let's start off with the labs first we have a hemoglobin of 12.5 platelets of 180,000 a white
a white blood cell count of 8500 peripheral smear and it shows no blast mild normal cic anemia his ESR is elevated LDH mildly elevated we get some Imaging now chest x-ray we have a media styal Mass H okay lymph node biopsy we note readed Sternberg cells and a positive cd15 and cd30 and then we also get a PET CT and we know multiple enlarged nodes in cervical and mediastinal regions real quick Zack for these findings would this be like more incidental or would these be like they would be he would be much more symptomatic so
um with this one I think like whoever started this off whoever started the workup up um with having this lymphadenopathy that would be the big thing would be lymphadenopathy and the b symptoms that's kind of the biggest symptomatology that I would see in this patient to suspect lymphoma the other things that they potentially found as a result from the labs and imaging I think some of them maybe there was the first thing I would have said is if I have a patient who has lymphadenopathy and b symptoms would be consider working up for like an
infection uh could there be something else that's going on and so a CBC was pretty helpful in that and hemoglobin there's some mild anemia plet are pretty much normal white cell counts normal so there's no evidence of kind of like any infection or inflammation at least in that scenario uh and the peripheral smear just really doesn't show any kind of blast that would suggest like maybe like a leukemia and if the white cell count was pretty high maybe it could have been a leukemia as well that have infiltrated into um a lymph node so that
was helpful as well but chest X they didn't have any symptoms so I didn't see any symptoms uh of cough or no dnia or any kind of like you know dysphasia anything like that would suggest from a medial Mass causing compression so that was probably just an incidental finding which actually happens pretty often um when patients have like hodkin Loma the most common subtype which we'll talk about is called nodulos sclerosis that te typically likes to hit the mediastinal lymph nodes and it'll cause the enlargement of those they can be completely asymptomatic 50% of the
time they're probably incidental findings you get a chest x-ray CT for something else and you happen to kind of meander upon them but this is a pretty good work up here on this patient definitely and if you note we also see that he has so cervical we see super clavicular and now with the chess x-ray we also have a media styal Mass so it is following a little bit of a pattern at this point that's the key thing with like hodkin lymphoma is that whenever you have like someone who has a a very let's say
contiguous spread so having lymphadenopathy that targets the cervical that's the most common 70% of the time when patients have lymphadenopathy and it's do lymphoma it's probably you know cervical that's most involved so it starts there but then it spreads and so you'll go from your cervical and you can kind you can kind of bifurcate you can go down into the medium and you can go to the Super clavicular and then from Super clavicular you go to axillary and then from medum you go to abdominal abdominal down to theal ones so this one kind of has
a a nice contiguous spread to it and then lymphadenopathy that is not painful where it's more painless it's firm you know that really suggests more of a malignancy than it does kind of what's called a shoddy or reactive lymph node due to like an infection or inflammation so that that this like right here really screams hodkin lymphoma especially ly in general uh just because lymphadenopathy b symptoms and lymphadenopathy is contiguous it seems it's gone from cervical and then bifurcated into that super clavicular and into the medial um and then the b symptoms also support that
and then you got this patient he got all this stuff like he got a really really great workup but I think suggesting basically the process of his presentation and some of the things we've seen here really it suggests more hodkin than it does non hodkin Loma with that being said we also have it Li lymph Noe biopsy so what do the Reed Sternberg cells and the the positive cd15 and cd30 tell you yeah so when I have a lymph nodee excisional lymo biopsy which is the only way that you can truly diagnose lymphoma is I'll
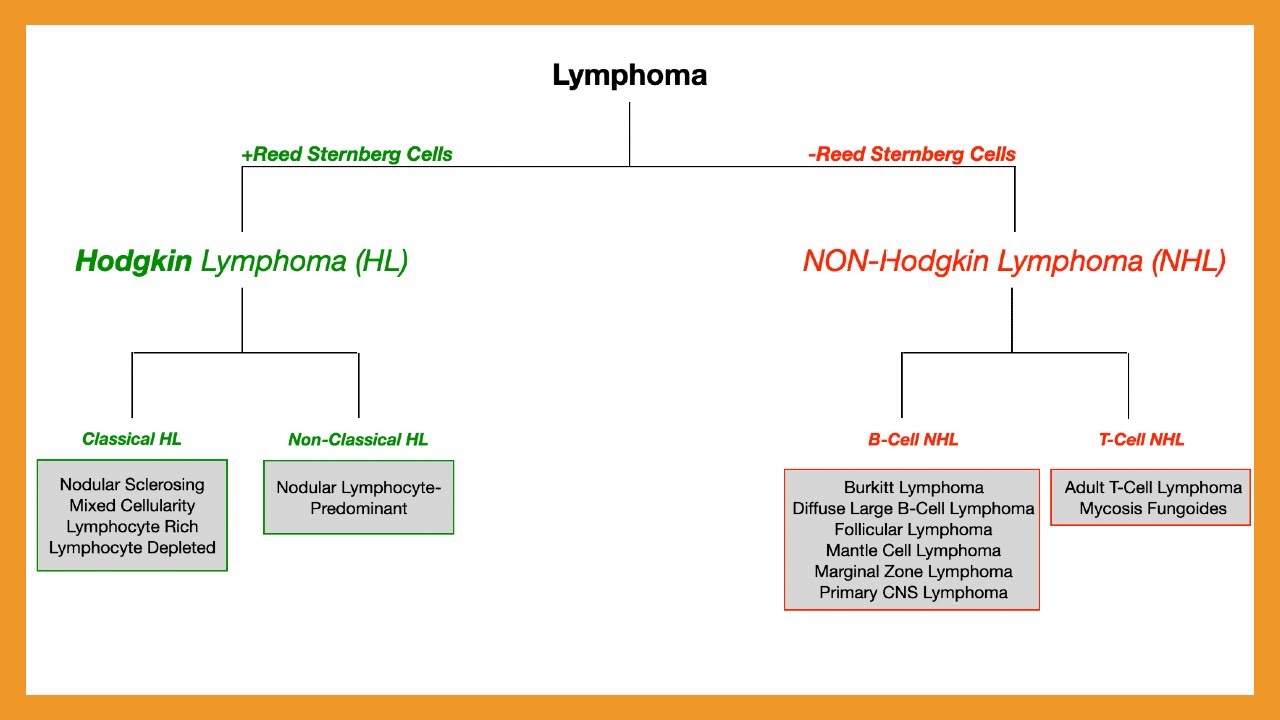
take those cells and what you want to know is is Reed Sternberg cells is basically pretty much pathom monic for hodkin lymphoma so whenever you see breed Sternberg cells it's hodkin whenever it's like not readed sturg cells it could be non hodkin you just have to figure out which type it is so once you then just said okay I got Reed Sternberg cells it's definitely hodkin it's not non hodkin then from here I got to determine if it's classical or non-classical so classical is about 95% of cases and then nonclassical or nodal lymy predominant is
about 5% so it's really low but you do what's called imunohistochemistry basically all you do is you take the tissue from the lymph node you run it through this like imunohistochemistry which is you take like antibodies and see if it tags specific proteins and if you have cd5 and 30 positive those are abnormal B cell markers not usually present on normal B cells so it indicates kind of a a reed Sternberg cell so cd15 30 positive cd20 45 which are normal B cell markers those are going to be negative and that really tells me it's
a classical hodkin lymphoma right there and then as far as confirmation goes it really is a lymph noopsy that's the main way of doing it yeah you can't really diagnose lymphoma unless you do a you know in this case an exision lympo biopsy in short his clinical presentation the symptoms really are all kind of leaning you toward hodkin but then you need to have that lymph node biopsy to say okay H lymphoma yeah yeah exactly so that's the only way that you can truly just like for example for most of leukemias you can't really diagnose
it truly unless you get a a bone marab biopsy sure uh the only one that you can potentially not do is CLL but all the other ones you have to get a bone marab biopsy to truly confirm same thing for this one you need the lymph noopsy to find these malignant you know lymphocytes that are present there all right so then we're we're at this point we have confirmed hodkin lymphoma what other complications could you see with this disease cuz I'm he doesn't look like he has too many at this point but what are some
scary things that could happen that's good so I think prefacing this prior to that mentioning of which kind of complications is it's important about hodkin lymphoma is if you could get one it's the best one to get okay so uh lymphoma is you know hodkin Wise It's probably counts for maybe 40% of the cases U most of the other ones 60% is going to be non- hotchkin um hodkin has a pretty good prognosis so overall it's pretty Curative um but there is different subtypes so nodulous sclerosis is the most common um and that one tends
to pred Dominate and involve the medal lymph nodes and that would be under the classical umbrella yeah exactly the other classical ones could be like mixed secularity that maybe makes up 30% um and then that one you see a lot in epine bar virus infections and U maybe even HIV uh the other one is lymy Rich that has the best prognosis and then the lymy depleted that one has the worst prognosis so whenever you think about hodkin lymphoma in general it has a good prognosis but the worst of that good prognosis is lymphocyte so that's
the one where even though it is kind of a bad diagnosis in the sense it's still something that can be Curative and then you said nodular sclerosis 60 mixed cellularity 30 and then the other two are five and five yeah they make up the remaining 5% and then naul lymph predominant for the non-classical path non-classical hot lymphoma it makes up a small percentage of the overall because classical is 95% non-classical is about 5% of the cases and ndro lymy predominant is the only one that's really a part of that subtype we don't really see it
too often and I think an important thing to remember for that one is you can do the CD 15 30 20 45 testing um and for these cells they don't have Reed Sternberg cells they're variants they're called popcorn cells and they actually do have cd 20 45 positive so they have their normal B cell markers and they didn't transform their other ones and so they actually are cd5 and 30 negative unlike Reed Sternberg cells which is the exact opposite I was going to say it's just flipped exactly all right yeah but I think complications it
really just kind of depends um usually lymphadenopathy is a big one b symptoms is a big one U Medi styl masses is where you got to be care careful if they get pretty bulky like big enough greater than 10 cenm they can cause Mass Effect it's not as common in hodkin as it is in non hodkin non Hotchkins it can get pretty big and they can compress structures but if it did get big enough and compress the trachea you can get dnia Strider if it compresses the esophagus you can get some dysphasia and if it
compresses the supera that's where you can get some supera syndrome so they get really enlarged you know facial neck swelling maybe some distended veins that you can see there um they can get like some arm and some chest kind of swelling and they can even have some distended veins in that area and it can look a little bit rough when you see it but it's not really an emergency unless you start seeing impeding uh Venus drainage from the from the cerebral system so high ICP could be a potential complication if they already have like a
cerebral structure that's actually kind of a space occupying lesion um they can get hypotension potentially from massive Venus return that's being impeded or compression of the heart and sometimes even lenal EMA is a scary one but those are the big things to watch out for I'd say is medial masses again b symptoms are pretty common lymphadenopathy is pretty common it's usually contiguous it's a consistent pattern the only thing I will say and this is what they like to ask in the textbooks is that when patients have hodkin Loma they get chemo theapy and they get
radiation therapy it's the radiation therapy that you got to be careful for we give radiation therapy uh for localized lymphadenopathy it's really good at hitting that area with radiation therapy to kill those leukemic Loma cells um but it can cause secondary malignancies because you're hitting things that are nearby so you got to watch out for other kinds of secondary malignancies that can potentially arise especially like breast cancer um and even like acute leukemia actually can form as well so those are the big things I think to watch out for is secondary malignancies due to like
radiation therapy can actually and and chemotherapy so the chemotherapy could actually cause the acute leukemias potentially and then the radiation therapy could potentially cause like breast cancer so that's something to watch out for now with hodkin lymphoma as a whole it has a favorable prognosis when compared to non- hodkin lymphoma so how is it treated all so it depends on the stage so you got to do what's called the like this guy got a was it a guy or a girl sorry it was a guy it was a guy they got a PET CT so
they had lymphadenopathy and then multiple and large noes in the cervical and mediastinal regions okay so when you have these lymph noes that are being involved you have to then do the Lano classification and so you basically take the PET CT scan and you look and say okay is there one lymph node region being involved if that is that stage one is there greater than or equal to two lymph node regions in the same like side of the diaphragm so meaning it's like in this case let's say it's above the diaphragm and then stage three
is you have lymph node regions that could be above and below the diaphragm and then four is it has extr noal involvement so it involves other areas besides your lymph nodes like your bone marrow your spleen your liver your brain um uh your skin anywhere really your git if it involves those other areas and infiltrated other tissues then you're stage four so this one tells me that they don't have any extra noal involvement but they do have multiple and large nodes in the cervical medical regions so it's greater than or equal to two l no
regions on the same side of the diaphragm it's above the diaphragm it's media stal so this would be stage two now I have heard of the an Arbor staging so is this just a different type of classification it's a modified an arbor staging yeah so it's basically imagine an arbor it's been modified and improved and so we use the Lugano classification now and some dude named Lugano came up with it probably yeah cool but yeah we so that's how we kind of determine it first is what stage they are uh and so I classify this
stage two and then you can actually subclassify so you can use um so stage two and you can do ABX for example so a is there's no b symptoms B is there is b symptoms and then X is there's bulky disease so you look to look at the lymph nodes and measure them and if any of them are greater than 10 cm you can add X to it so it didn't tell me how big the lymph nodes were so I'm just going to assume it's not greater than 10 cenm but they do have b symptoms
and so I could say this is stage 2B you know what I mean so from there we can determine that but stage one and two you do uh chemotherapy and radiation therapy okay all right so that's what is it the abvd regimen so adriam bomy uh you use what's called ven uh ven blasting and then decarbos uh and so those in combination with radiation therapy hitting the radiation therapy to the localized regions that should be able to achieve like a Curative uh response put them in remission but if they get a little bit more in
the aggressive stages um so they get to stages three and four then we we only do abvd regimen preferred um in certain scenarios you can escalate it to What's called the the be a cop regimen I always got these things chemo is intense he when you look at these and I used to like consult other like hemon teams and stuff for patients who had underlying malignancies and that I was seeing them for like neural or logical or you know intensive care for purposes you would read their notes and You' be like oh my gosh these
chemotherapy meds they're insane the amount of acronyms are insane yeah yeah it's it's intense everything's abbreviated and funny enough we'll have like a chemotherapy like podcast but I think the yeah but the big thing for the be aop one is is that this is really only if they're like pretty aggressive so I'd say if they really have some extensive like Extron noal involvement it's disseminated you can use that one and it's um so it's bomy aoide adriamycin cyclophosphamide Vin Christine and then um procarbazine and prednizone so it's a lot of those that you're adding on
to really help with that process but sometimes they just do the abvd and they'll do multiple cycles of it as instead um the other thing to do is that you just really want to keep an eye on these patients and then continue to potentially do serial PET CT scans to see if you're eliminating some of those hot spots um or the lesions that kind of turn up hot on the CT scan and see if you're improving that or getting rid of some of those extra noal sites that's the ultim ultimate goal is to get this
to where you're not really having these lesions light up on PET CT anymore so that would be the ultimate goal is complete Curative um you know therapy well let's move into non- hodkin lymphoma which is much more common and of course the the prognosis isn't as good as hodkin lymphoma yep so let's start off with our patient here we have a 68-year-old male presents with rapidly growing abdominal mass and intermittent fevers for the past 2 months the patient reports a painless mass in his left lower abdomen which has rapidly enlarged over the last two months
he has also experienced intermittent fevers night sweats and a 15b weight loss he has no significant bruising recurrent infections or prior malignancy for his past medical history we have hypertension no known autoimmune disease and there's been no prior malignancy medic ations he's on linpro and for his exam his vitals are BP 130 over 75 heart rate is 78 temp is 37.6 Celsius and his O2 sat is 98% on room a his lymph node exam they are it's a palpable firm non-tender axillary and inguinal lymphadenopathy his abdomen large firm mass in the left lower quadrant in
his skin there is no peti or eimos present we do a pretty comprehensive lab and imaging panel we get the following back hemoglobin of 10.2 platelets of 140,000 a white blood cell count of 18,000 peripheral smear showing aty atypical lymphocytes his LDH is elevated we do a PET CT and we see widespread lymphadenopathy axillary retrop peraonal ininal regions we do a lymph no biopsy for our confirmatory test and we note large atypical B cells cd19 positive cd20 positive for his bone marrow biops we also do a bone marob biopsy it we have involvement of the
marrow with large B cells and for his cytogenetics we have a translocation of 34 and 1418 this involves mutation of the bcl6 and bcl2 overexpression respectively some questions Zach out of all of this information what do these findings suggest we know we're talking talking about non- hodkin lymphoma but what are some things that jump out at you so first thing is lymphadenopathy um and it's abdominal Mass that's a little bit more suggestive of non hodkin uh but more more importantly I would say like when you look at their physical exam they got palpable firm non-
tender axillary and inguinal and then they also have this abdominal Mass so that's very like non-contiguous right so usually it should start like somewhere like the cervical spread to the super clavicular or then that one goes to the the axillary it can go mediastinal they can go abdominal they can go you know inguinal this is all over the place so we got one in the axillary and then we got one over in the inguinal and we got in the ab abdomen so it's very diffuse it's a non-contiguous non you can't predict the spread so that's
super classic of non- hotchkin lymphoma that's right away what screams at me um b symptoms um he does have some b symptoms and so there is some intermittent fevers and night sweats and some 15lb weight loss so again I have lymp an opathy that's diffuse non-contiguous and it's associated with b symptoms I'm thinking lymphoma so obviously whenever you have that you would go and you would Target a lymph Noe biopsy and so with this patient they got a lymph Noe biopsy and it showed that there's large atypical cells they're B cells so it's a B
cell type of non- hodkin lymphoma and we can confirm that with cd1 1920 just so for you guys are listening you can confirm if it's a t- cell lymphoma so that's the rarer type it's about 15% of your lymphomas for non hodkin but it can be t or B so for the T it's about 15% and then there's these components there which we'll talk about uh it's cutaneous t- cell lymphoma and that's consist of mosis fungoides and then Cesar how do you say it Cesar Cesar syndrome Cesar Cesar syndrome so yeah those usually make up
your cutaneous t- cell lymphomas so you'll have a lot of skin manifestations and then adult t- cell leukemia sloma that's usually seen with the human lympo t- celly Tropic virus infection and so we can already throw the t- cell mediated lymphomas out the window because the only way that we tell that is they'd have to be CD3 and CD4 positive and they don't have that so that right there helps me to say it's not telmas and they don't even have any skin manifestations and so I wouldn't have any pric papules or rodera and usually for
adult T Cell leukemia sloma they cause liic lesions and hypercalcemia so that's not even present as well so it's not teloma it's a cell from there you have to determine which type of B cell lymphoma and they were pretty good they got like a bone marrow biopsy which you don't always have to do you can just do a PET CT scan the real indication for why you would do a bone marrow biopsy is it showed maybe your PET CT was negative and you suspect that the bone marrow was involved and how would you suspect that
the bone marrow is involved I would really prefer to see pancytopenia so I don't really think that this patient completely warranted a bone marob biopsy it used to be the older way of doing things where almost every patient would get a chest x-ray a CT of the chest abdomen and pelvis and then they get a bone marrow biopsy we don't really do that anymore now we just kind of go at pet C scans and then we only do the bone marrow biopsy if they have pancytopenia or if the PET CT was negative um and then
we do lumbar punctures only if they have symptoms that suggest like primary scenus lymphoma or menitis um or that pet C didn't really show me that so I really didn't need the bone marrow biopsy but it's interesting because it shows me that those large atypical B cells that were in the lymph node are now in the bone and it probably infiltrated there what really helps me is the cytogenetics because when we get a belloma I told you that there was te- cell and that was cutaneous so mosis fungoides or Cesar and then the adult t-
cell leukemia sloma for B cells there's mantle cell follicular diffuse large B cell lymphoma buret and marginal Zone lymphoma and so you're you have to figure out which one would it be you can look at the histology and that always helps so looking at the biopsy can tell me it's large atypical B cells but on the exams you don't often get tested on that you get tested on the C of genetics so you told me it was the 314 1418 translocations and their bcl6 and bcl2 overexpression was the primary ones that we see that's almost
always associated with diffused large Bell lymphoma especially the bl6 overexpression if I saw let's say for example 814 translocation with an increase in the CMC I think Burk it if I saw that there was um 1114 then I would think mantle cell inoma and that one's associated with increase cycl D if I saw 1418 translocation I'd be associating that with follicular cell lymphoma and that's an increase in bcl2 if I heard autoimmune diseases like shaan syndrome Hashimoto thyroiditis or if I heard um they had gastric uh tumor like a malt lymphoma from H pylori it's
always marginal lymphoma so things in the history or things in that cytogenetic study would tell me which type of B cell nonod lyoma it is and this is really suggesting uh that it's likely the diffus large B cell and the benefit of that is that diffus large B cell lymphoma is the most common type of non- hodkin or Bell mediat related non- hotchkin lyoma so right here I'd say I'm pretty much like convinced that this is going to be diffuse large B cell lymphoma so with having the diffuse large B cell lymphoma what are some
complications that you need to be looking out for and what are some things that are red flags for you to look out all right so first thing is going to be um I would like to look for extra noal involvement and so the PET CT scan would definitely help me with that right because we've confirmed at this point that we know it's diffused argb CA based on the biopsy we can determine the stage of it based upon the PET CT scem so that's what I would want to know so there's a couple different kind of
complications that can happen one is with extranodal disease you can involve the central nervous system so you can get primary CNS lymphoma that's a really scary one we see this a lot in patients who have HIV AIDS um it can actually be an AIDS defining illness and so sometimes they may come in with a headache they may come in with altered mental status they may come in with potential behavioral changes you'll get a CT scan of the head you'll see a big mask you're like oh my gosh they have brain cancer and then you'll go
ahead and you'll get an MRI the brain and you'll see these ring enhancing lesions and that's almost always consistent with primary CNS lymphoma um you can get spinal cord compression that's a scary one that can be an emergency if a patient comes in they have a history of non hodkin lymphoma and all of a sudden they're presenting with you know they don't have any history of like degenerative dis disease or SP spinal cenosis or then you want to be concerned if they come in with like weakness sensory losses bladder bowel dysfunction could that um spread
to their spinal cord that's compressing the spinal cord um another one is the git so you can actually get some of these like spread to the git and you can get bowel obstructions um you can have it spread to the Bone you can get liic lesions you can get hyper calcemia you can get pancytopenia if it infiltrates into the bone marrow it can go to the skin it can cause skin lesions and um it can even go in the liver and the spleen it can cause like hpat SP AAL too so there's a lot of
different organs that think can spread to and that's why we have to use the PET CT scan to see where it has spread to um so with the with the PET CT scan then how would you then is this it's the same classification as before right same lugana classification so yeah you would say if it just involves like the one lymph node region stage one if it involves greater than or equal to two on the same side of the diaphragm it's stage two if it involves lymph node regions on both sides of the diaphragm stage
three and if it has extra nodal involvement which is way more common with non- Hotchkins yeah that's going to be stage four that's why you see more often than not nonot lymphoma having a worse prognosis because it's more has a predilection for those extranodal tissues Prett aggressive then too yeah and so that's the big thing to remember for that one other complications is tumor liis syndrome so you can see this with acute leukemia particularly Al more than AML but you can see the non- Hotchkins so if they get chemotherapy and they have all these like
tons and tons and tons of like just chunked up tumor cells and lymph noes and other tissues and you hit that chemotherapy to it you can bust those cells open they release potassium uric acid and phosphate and so you can get acute kidney injures from the uric acid you can get hyperemia causing cardiac arrhythmias and you get hypocalcemia because the high phosphate will bind up the calcium so that's another one um the other thing I would watch out for and this is a big one for follicular lymphoma and CLL we talked about it in The
Chronic leukemia lecture is that sometimes in clll and then follicular lymphoma follicular is actually an indolent type of non- hotchkin so there's actually two types of non- hotchkin there's indolent which is meaning it's it's very slow gradual Progressive it's not a severe that's follicular marginal Zone lymphoma and then there's severe aggressive highgrade lymphomas these are very very hyperproliferative that's going to be your diffused archb cell your mantle cell lymphoma and burket Lymphoma funny enough follicular lymphomas can start off gradual Progressive indolent and if it undergoes that translocation of 314 it can then transform into diffuse
large Bol lymphoma so they can actually end up having that problem where they can have what's called a RoR transformation so you can start off with a very mild lymphoma an indolent one and all of a sudden rapidly enlarging diffused lymph no b symptoms are getting terrible and then you end up with LDH really high you end up with extranodal involvement and now you have diffused large B cell infa so that's that's another thing to watch out for so I'd say extranodal disease tumor Lys syndrome and then possible RoR Transformations well now that we're talking
about the diffuse large B cell lymphoma yeah how is it treated uh so you would treat any kind of aggressive type of non- hodan lymphoma you would check that at cd20 was our cd20 positive oh yeah yeah so in order for you to have a c you have to get the cd20 that's positive you would do what's called a rmab base chemotherapy so it's our chop and we would do rmab cycop phosphamide hydroxy Donar rubesin um we would do enoven and we would do prednizone and these are going to be the ways that we would
treat a patient who has this type of process and again diffus ARB cell lymphoma we could do um diffuse ARB cell lymphoma like this we could do mantle cell lymphoma like this you can consider burket lymphoma with this one sometimes they do the SE therapy that we talked about in the acute leukemia lecture uh but arop would be the primary gold standard for this patient um if they have an aggressive non- hodin lymphoma if it's indolent we can just do ruab as long as they're cd20 positive so you always have to make sure that their
cd20 positive because if not rmab won't work because rmab is a monocon antibody that literally targets the cd20 and then literally causes your immune system to kill those L those lymphoma cells and so we would really need them to be cd20 positive um for patients who have diffuse larb an aggressive non hodal lyoma diffuse burkets mantle they have HIV and they have other tissues that are extranodal tissues that are involved the testicles um the Parry uh partions of your spinal cord the epidural or the meninges those patients are super high risk for CNS infiltration and
so in those States we actually have to do CNS prophylaxis so we had to put in either an omay res Reservoir or we do a lumbar puncture and we squirt in chemotherapy you would think oh can you just give them the systemic chemotherapy the arch chop and it'll cross the blood brain barrier it doesn't and so you have to give them chemotherapy that you actually put into the cerebral spinal fluid that you prevent them from developing primary scus lymphoma menitis spinal core compression and all those things and so that's where I would add in the
intrathecal Methotrexate only if they have an aggressive highgrade lymphoma non hodkin HIV positive because that puts them at super high risk for primary cenus lymphoma um and then if they have multiple other extra noal sites that are involved particularly the testicles are a big one um and then again we say around the actual vertebrae around the epidural spaces these are really really sensitive areas and even for some weird reason the paranasal sinuses if they're near those areas these patients are super high risk for some type of like you know CNS involvement and we just want
to get them on intal methotraxate um the last thing I I would say is if a patient has really bad uh lymph nodes like they have supera syndrome because they have a meal like lymph an opathy that's compressing on that area we could do radiation therapy and if they have spinal cord compression from like a bulky kind of like tissue compressing on the spinal cord then we could do radiation therapy for those as well that would probably be more so with the te- cell one right you could you could do it the it could be
in the t- cell you can see with t- cell but you can also see it in B cell okay yeah so you can see it them both but yeah spinal cord compression scary one steroid are usually the upfront and then radiation therapy you'd have to reach out to your radiation oncology colleagues um and the same thing if you have super aava syndrome I do steroids maybe stenum if it's really really bad um but ideally it would just be getting them some radiation therapy to kind of decrease the size of it rapidly all right well we
talked a ton about hotchkin versus non hodkin lyoma I would say before we end this episode is there any quick and awesome key takeaways High Yi points that you can differentiate the two a couple different pearls that I would say to take away from this is that T lymphoma again you're going to want to look for that lymp anopia that's usually predictable it's usually cervical and then spreads in a contiguous Manner and it's almost always associated with b symptoms also remember it can cause mediastinal masses um and again that's usually the nodular sclerosis subtype biggest
thing with this one diagnostically is when you get a lymph node biopsy from that big swollen lymph node if you see Reed Sternberg cells it's hodkin lymphoma and then if you figure that out boom you just start off by saying okay what stage are they are they stage one two that's abvd chemotherapy plus radiation if if it's stage 3 4 it's just usually just abvd by itself for non hodkin lymphoma you want to look for lymph nodes that are really really enlarging pretty significantly but again they're not in a contiguous manner they're they're they're really
unpredictable they're diffus so you may have it in the cical then you also may have it in the axelay on the other side you may have it in the abdominal you may have it in the anginal so it doesn't really make sense the way that they're spreading and then again they can have b symptoms but extranodal disease is the classic difference look for s CNS involvement skin involvement GI involvement bone involvement bone marrow involvement liver and spleen involvement if you see that it's way more likely it's non hodkin again with these they can get pretty
bad but if you figure out from their lymo biopsy that they don't have Reed Sternberg and they're atypical malignant lymphocytes you just have to discern is it b or t look at the CD proteins and that should identify it but again the biggest thing from this is once you've identified that it is non hotk lymphoma you treat that appropriately if it's your aggressive subtypes you treat that with the r chop regimen if it's the non-aggressive or indolent subtypes like follicular or marginal Zone you treat that with Primary retab Therapy only thing I will add is
if it's marginal zonoma you can actually treat that without chemotherapy at all and that is really important to remember that we consider this in patients who have hpylori gastric malt lymphomas we actually just treat them as though they had peptic ulcer disease from H pylori yeah the quadruple therapy yeah because you're just kind of reducing the risk of recurrent immune activation and then causing them to have worsen than gastric M lymphoma so that's the biggest thing and I would say always monitor for the scary scary complications in these patients especially non- hodkin watch out for
CNS involvement watch out for tumor Lis syndrome watch out for any kind of like spinal cord compression and and and those are the big things I would say to take away from this that's awesome that was a really cool episode that was it was quicker than I thought yeah I think lymphoma a lot of the times when it comes down to it it just starts off with a big lymphonode and some b symptoms and you just kind of work down the process of is saying okay is it hodkin non hodkin and then if it is
how do I treat this yeah and that's really what it comes down to awesome well it was super informative thank you yeah thank you guys and I hope that you guys likeed this podcast I hope it made sense I hope that you guys enjoyed it and uh love you thank you and as always until next time [Music] oh [Music]