[Music] hello i'm dr christopher slatten i'm the clinical director of the pain rehabilitation program at the mayo clinic in jacksonville florida in 2015 we videotaped our first central sensitization video to describe the process that happens with chronic symptoms and also to explain how a program like ours can be very helpful for individuals with chronic and hard to treat symptoms we're redoing the video at this time for a number of reasons in the past several years there have been a number of clinical developments that have allowed us to expand the scope of patients that were able
to help and so pain rehabs have always been effective for individuals with migraine headaches fibromyalgia chronic back pain other musculoskeletal pain disorders chronic abdominal pain we've really been shown to be very effective and and have long-term benefit for individuals that that have those issues today i want to introduce the concept that we are also able to help individuals with a wide variety of chronic symptoms including those patients that have eylar stand lows pots functional neurologic disorders even post covid patients are benefiting from this program and the core reason for this is that we are expanding
our understanding of the concept of central sensitization which has allowed us to broaden the reach of our clinical scope so today i'm going to go over the model of central sensitization again adding some pieces and hopefully amplifying on some of the things that were not covered in the first video first we're going to start with a brief discussion of acute and chronic medical conditions and this is a very important distinction to understand because most of medicine whether we're talking about conventional medicine we're talking about alternative medicine interventions or new innovations in treating symptoms most treatments
today focus on the problem as if it were acute and so i want to distinguish the two conditions an acute medical problem by definition is time limited the cause is generally known [Music] onset is known treatments work and tissue damage and symptoms match up an example a broken ankle someone steps awkwardly off the curb they twist their ankle they hear a crack they go to the emergency room it shows a fracture it fractures where it hurts we put a cast on it we're good to go after six weeks sinus infection antibiotics hot appendix appendectomy those
kind of things and even some complex medical situations like cancer some cancers if treated in a timely fashion with proper treatment they can be expected to resolve so this is what we expect this is what we desire this is what we often get out of modern medical care however there are instances and this can happen for a variety of reasons where the the syndrome or the disease or the medical condition changes to chronic and the rules change frankly so when it becomes chronic it is now long lasting perhaps even permanent we're not always sure if
what causes it to be come chronic we aren't even sure when it becomes chronic treatments become very plus minus and tissue damage and symptoms don't match up so well anymore this might be the person with the broken ankle that three years after they break their ankle it still hurts and the problem with this scenario is historically persons with this problem often are doubted often they're told we don't see any problem on the mri we don't know why you have symptoms and in fact historically this has often been relegated to the realm of psychosomatic maybe you're
depressed maybe this is some issue that you haven't resolved in your life and nothing can be further from the truth those of you watching that have chronic symptoms you know it's real you know you're not imagining this and i want to emphasize this several times today that this is not a primarily psychological problem however when this happens and we still apply an acute methodology it just leads to more problems and so i'm going to over the next several minutes elucidate the pattern of this and and also some solution so i'm going to go over to
the rough sketch very rough sketch admittedly rough sketch of the nervous system it's a spinal cord in the brain or it's supposed to be the human nervous system can be divided generally into two parts central and peripheral central nervous system is brain and spinal cord peripheral is generally sensory motor and the autonomic nervous system we're going to focus initially on the sensory pathways the sensory pathways begin in the body we have sensors in every square inch of our body except for our hair and fingernails this is an also an important concept to realize because symptoms
chronic symptoms can arise from almost every system in our body so you can see this happens in any part of the body so sensory processing let's start with just a very basic elementary explanation sensory processing is basically supposed to work like a light switch stimulus present sensation stimulus absent sensation gone and that's how most of us experience our sensory world if i take a sip of coffee i taste the coffee when it's on my tongue i swallow it the taste goes away but for a variety of reasons these sensory pathways can become augmented or upregulated
over time and for purposes of your understanding i want you to think as broadly as possible this can start with an injury this can start with a progressive disease this can start sometimes seemingly out of nowhere but there always starts in the body with the change in the way that the sensors perceive and react to stimuli very quick explanation if i tap on my hand with the back of this pen i can report that every time the pen makes contact with my skin i'm perceiving a tap when i stop it stops i could however develop
a situation called neuromodulation where i tap long enough that when i stop i might still feel tapping for a little bit we've all had that happen to us if you've ever been on a boat and you get back on dry land and you still feel like you're going up and down or you've you've been on roller skates or ice skates you take them off you still feel like they're on your feet or if you're into such things you get off the roller coaster and you're back on the ground and shakra still has your soul up
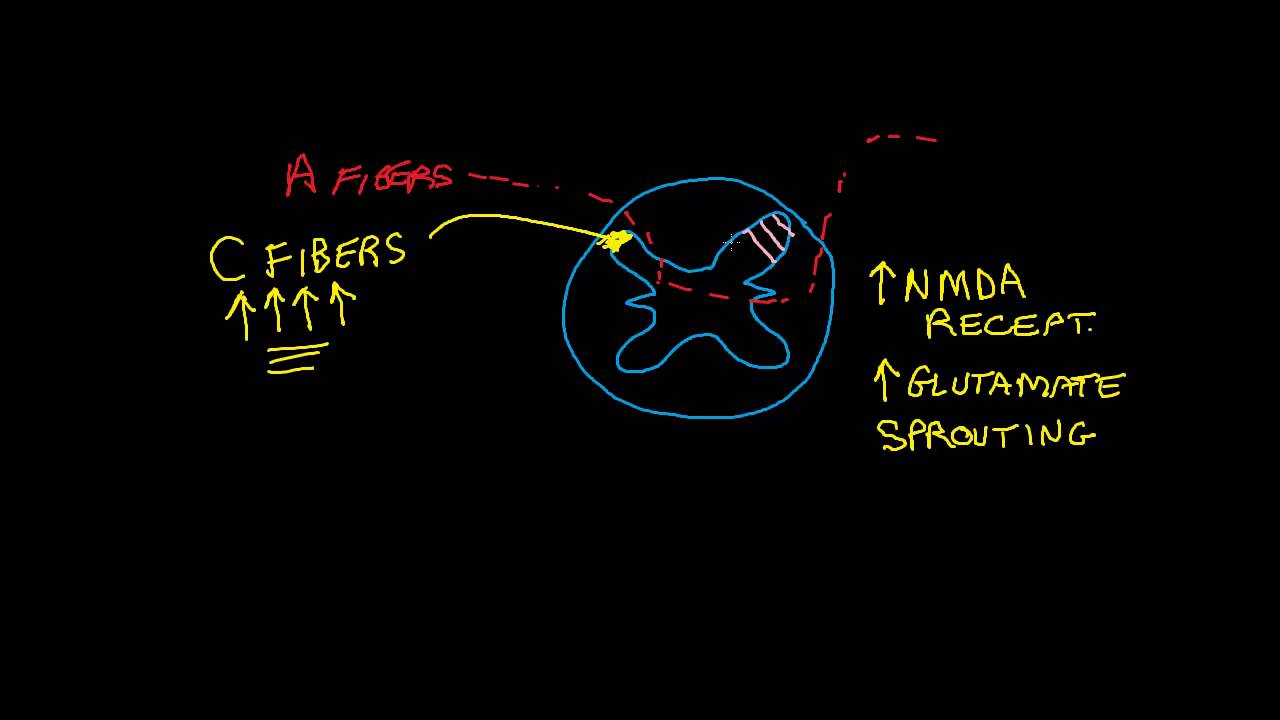
in space somewhere that's normal but the third iteration is where the sensors can be stimulated to such a degree that they never shut up or they shut up and and turn on at random times that's called neuroplasticity that's the beginning of the change and it gets more complex from there because with signals that have now changed in the body talk about them being up regulated now the body is sending a stronger signal to the brain and the primary target of all that sensory information is what we call the sensory cortex the sensory cortex sits in
both hemispheres of the brain it's a strip of neurons that's organized by body part so everything that happens in our body registers up in the brain it's a body map so if i stub my left big toe it registers left big toe in the brain that's an important concept because for a very long time it was poorly understood how symptoms can move around how they can pop corn how they can appear here one day and they're the next i've had patients that broke this arm and over time this arm hurt it's because they're neighbors up
here and when they get riled up they can affect other sensory parts of the body secondly as that gets sensitized it starts to react more vigorously to less input it's sort of like if if we look at this area like a smoke detector and a normal smoke detector in the kitchen would only go off when you burn something on the stove but now it's been swapped out for a super duper sensitive smoke detector that goes off at 100 decibels when you light a candle in the bedroom is the candle still a flame yes is it
dangerous no but the brain becomes so reactive that now there are sensory experiences that don't necessarily translate to what's going on in the body that's confusing that's frustrating but that's part of the amplification in the neuroplastic response so with this we talk about the fact that symptoms can grow and so we see pain fatigue sense of dizziness nausea numbness burning itching tingling all sorts of sensations can emerge from this process as can triggers light sound smell taste touch temperature now all of a sudden we're in a situation where symptoms seem to get worse more things
trigger the symptoms and that's where the problem becomes more and more worrisome and more and more confusing but before i move on i want to highlight a second part of the brain that could get impacted it's a neighboring map a parallel map that's called the motor cortex it too is organized by body part so what is supposed to happen is we are supposed to have the smooth sensory motor flow sensations come in direct our motor or movement activity so that we can navigate our environment so with the changes in the motor cortex we see individuals
that start to have issues with movement it might be simple as a tremor or spasm or stiffness it might be a whole body episode whether it looks like they're having a seizure and our neurologic colleagues will tell us we don't see evidence of epileptic activity in the brain we don't see evidence of a progressive neurologic disease but these individuals are still smitten with these chronic symptoms so from a motor perspective we see spasm [Music] tremor and these also can be triggered more easily so let me take a pause for a second and put this in
context if all these symptoms are emerging and as you're struggling with them you and your providers and your family are still viewing this through an acute lens this is a very worrisome development because if you have an acute problem and it's getting worse over time something has gone terribly wrong if i break my ankle and three weeks into casting it hurts worse than the day i broke it something's gone wrong or for patients going through chemotherapy and six weeks into chemo they have more tumors than than when they started chemo there's a problem but this
model predicts worsening of symptoms over time unless we do something different this model also explains why traditional treatments whether they're conventional medicine alternative medicine whatever stop working because you can't unsensitize sensitized sensors you can't cut it off with the spinal cord you can't turn off in the brain and so persons with central sensitization syndrome problems begin to get frustrated the shots don't work the acupuncture stops being effective the massage the the tinctures the diets the supplements the pain pills it all is doomed to fail ultimately this is where i want you to be very cautious
with what's out there and being promised right now the internet is full of false promises it is full of pseudoscience it is full of people out there saying oh if you just take this supplement if you just do this diet if you just rub this lotion you're going to be fine it's it's impossible this can't be stopped with any somatic physical treatment lastly before i move on there's also no psychology here this is not primarily a psychological disorder can psychology make it worse of course it makes all of our physical things worse but this did
not start from a psychological cause this is not a somatization disorder this is not a conversion disorder this is none of those things so i want you to take courage and understand that this is not psychological either so with all of that i appreciate the dilemma you find yourself in worsening symptoms fewer answers treatments stop working we can't medically treat this we can't psychotherapize you out of this what do you do well here's the answer we need to approach things differently because if this pathway is generally unchangeable then we have to find a different direction
and so from a pain rehab perspective from a symptom rehab perspective we've arrived at four targets of treatment physical emotional behavioral and chemical i call these the reactive and maintaining factors reactive because these are issues that when you first start having your problems it made sense to do certain things if it hurts don't do it put ice on it rest get a shot take a pill it's scary so all those things make sense but in the long term these are the things that now make this worse and so in our program and in our pain
rehab approach we look at physical deconditioning no one has ever come to pain rehab in the best shape of their life it's hard to maintain physical fitness in the face of chronic symptoms now for sure this is on a continuum some individuals come to us and they're just slightly deconditioned others are profoundly deconditioned the level of conditioning doesn't matter we're just going to reset the mechanism work on whole body reconditioning strengthening cardio and flexibility instead of focusing on different body parts we're going to look at the whole body as a unit to get it stronger
we talk about our physical therapy intervention as fit for life trying to get you back on track emotional it's distressing when you can't do what you want to do when you want to do it it's distressing when you have out of control symptoms it's distressing when there's no answers and some of our patients come with previous mental health issues but a lot of our patients come with anger and depression and anxiety and stress because of the problem but in either case we address it through a cognitive behavior therapy model we give a lot of tools
a lot of practical advice a lot of application to help individuals reduce the emotional distress behaviorally there's two issues pain behaviors which are anything a person says does or thinks it reminds themselves or others that they're having symptoms so we work on reducing those because those feed this we also work on moderation because pushing and crashing stirs us up many of you watching this video have been busy and active folk you're type a you want to be in the game and every time you felt better you thought i got stuff to do and you got
up and did stuff and you overdid it you pushed stirred everything up and you crashed pushing and crashing feeds the problem every push stirs up symptoms every crash leads to deconditioning and then finally chemical and we're all fully aware of the dangers of addictive drugs and and certainly that's part of our scope we we do help people come off of opioids and benzodiazepines and sleeping pills and things like that but we're also very concerned about any number of symptom treating chemicals that can add to the problem because whether the drug is psychoactive or not anything
you put in your body for your symptoms reminds yourself and others that you're having symptoms and it can stir up the pathways and as i mentioned a few minutes ago there's nothing that's going to turn this off there's no chemical there's no natural substance there's no vitamin there's nothing that's going to turn this off so all of that stuff turns out to be more fuel on the fire so as we wrap this up i want to make one last analogy i often think of an acute medical problem like a house fire when there's a house
fire it's a big deal for a localized area fire department comes in puts out the fire the family rebuilds etc but chronic is more like a forest fire forest fires have impact well beyond the boundaries of the burning stuff if you've ever been near a forest fire you know the skies get smokey for sometimes hundreds of miles away it can change weather patterns and and it doesn't just go out with enough water unfortunately we've all seen far too many news reels of of forest fires consuming hundreds if not thousands of acres of land and the
only way to get rid of a forest fire is you contain it you cut off the burning stuff from the non-burning stuff so those brave men and women are out digging dirt berms and lighting backfires and doing whatever they can to contain the fire well very much the same way with pain rehab we're working to cut the fuel off the fire that's why we work on these four areas so by introducing physical conditioning and fit for life by reducing emotional distress by normalizing behaviors by getting people off of chemicals we're cutting the fuel off the
fire and when we see that we see the symptoms begin to become contained the impact dies down and the person's functioning improves and so over time the three weeks of the program but also well beyond the program we see this new pattern emerge where the focus is on functioning not trying to eliminate symptoms and as we work with our patients we teach them how to work through these problems not try to stop them because at the end of the day this isn't directly stoppable it's not necessarily curable it's a permanent change in the system but
the permanence doesn't have to mean permanent impact it just means that the system has been revved up but we can teach techniques to help it calm down to reduce the impact to improve the quality of life so if you have chronic symptoms and you've struggled with getting them treated effectively if the quality of your life has declined you're struggling with sleep and mood issues and in decline in occupational and daily functioning relationship changes that's the stuff we can help with and i just want to again urge caution about pursuing the quick fixes there is no
quick fix this is hard work it takes time i just want you to understand this and i want you to see the breadth of what we can help with so again to repeat my opening statement not only fibromyalgia migraine headaches back pain musculoskeletal disorders abdominal pain but also individuals with either stand lows pots functional neurologic disorders post-covert syndrome and other things can benefit from this approach thank you [Music] you










![[PART 1] Understanding CRPS: The Truth About it’s Neurobiology and Effective Treatments](https://img.youtube.com/vi/XBB_7MrJkQA/maxresdefault.jpg)