hi is tom from running physio I wanted to come and speak to you live today to talk about medial tibial stress syndrome now this is a challenging condition a lot of runners struggle with this and can find it quite difficult to manage so I wanted to talk you through some of the things that we find really effective in clinic and a little bit of the research around their pathology and pain in this region now you'll notice also we put a link to our running resources page in the title of this we tend to put in
our Instagram bio as well there you'll find free videos on Achilles tendinopathy lateral hip pain and low back pain in athletes including a nice step-by-step approach to that so do you visit that page for more video content so let's talk about medial tibial stress syndrome or shin splints as athletes often call it we do think it's a bone stress reaction so the bone is being irritated often because of overloading and possibly because we've increased our training volume or intensity and we start to get pain now there's been some nice research which confirms this so winters
a tool how to look at bone biopsies in athletes with medial tibial stress syndrome and they found unrepaired micro damage accumulation which would fit with this sort of bone stress injury presentation they've also done some in excellent work in Mt SS diagnosis and they do think that we can reliably diagnose me to a tubular stress syndrome based on history and physical examination alone and actually in many cases an MRI isn't going to change management if we do think its medial tibial stress syndrome it perhaps would come in if we suspect a different diagnosis like say
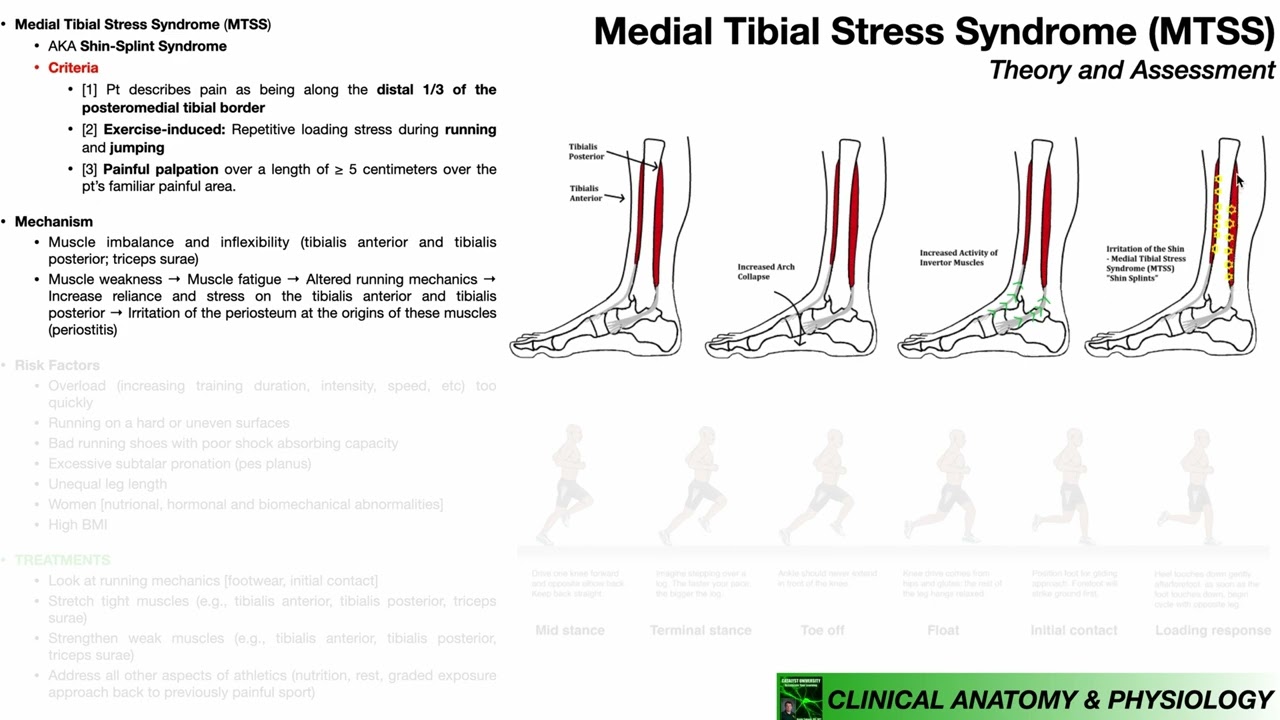
an anterior tibial stress fracture the typical presentation is exercise induced pain in the distal two-thirds of the medial tibial border so runners will often say when they're running they get this medial tibial pain that gets worse if they keep running there isn't the warmup effect that we can see in tendinopathy where sometimes a tender could be sore and get going it feels better if you keep running with the medial tibial stress syndrome and bone stress injuries in general the symptoms do tend to get worse but they will settle then usually when we stop now another
diagnostic criteria here is you would expect to have pain on palpation of the posterior medial tibial border of five centimeters or more that would be suggestive of medial tibial stress syndrome if there are other symptoms such as severe swelling pain that covers an area smaller than 5 centimeters pins-and-needles numbness cramping or symptoms that are more in a calf and posterior compartment that might suggest an alternative diagnosis or it may be that there's a coexisting issue there to consider now winters at all have done some great work in this field they've also done this great MDS
s score now this is a valid reliable and responsive outcome measure for medial tibial stress syndrome and what this does is it asks questions around symptoms during walking during sport and also at rest so you can use that clinically as an outcome measure so a lots of great work from meredith winters and colleagues now although we do think it's a a bone stress injury there does seem to be a bit of a gap sometimes between say MRI findings and pain you can have people with some periosteal inflammation bone marrow edema perhaps on on an MRI
but no symptoms so like in many regions across the body we can see pathology existing without pain so there's always going to be a question mark there of the exact connection between the two now one of the things I do think is quite important in athletes with medial tibial stress syndrome and in fact bone stress injuries in general is they don't do very well exercising with pain it tends to be a high pain no gain situation and in fact one study in runners with medial tibial stress syndrome said they could continue running as long as
they pain stayed at four or less out of ten but they did that and it actually took them around about hundred days to increase their running to just 20 minutes so it does seem clinically and in the research if you just keep working with pain takes things and you don't seem to get pretty far so I would aim with this for pain free loading particularly during running and impact based sport and this is a little bit different from other pathologies you know tendinopathy perhaps joint pain other issues we're quite happy to keep going as long
as the pain is mild and manageable and settles quickly in bone stress injuries and medial tibial stress syndrome this isn't really the case it's a little bit different so drew no rehab process we need to try and establish what is actually a pain-free level of impact loading and that's where our impact tolerance tests can come in really handy now these are really simple what we do is we start with light impact cuts something like - for impact jumping in place and see what symptoms people have if they're managing that pain free we might make you
a bit more challenging go to a minute of jogging on the spot then onto bounding and repeated hopping because we're looking to see what symptoms if any they get from these now this helps with the diagnostic process because most people with bone stress injuries will tend to to have pain with impact but it also know helps us to know where to start in terms of their loading if they can't jog on the spot for a minute then our pain is unlikely they're gonna tolerate running and generally we want runners to be able to hop repeatedly
maybe even as much as 30 seconds without pain before we're going to get them to build their running so we test that impact tolerance in clinic and we can use that then to form a bone loading program we look for that impact level that is pretty comfortable that doesn't trigger any symptoms and we can utilize that then as a way of building up their bone load tolerance by using that regularly and often in clinic I use something really simple this is a simple measure it measures are often the best so I'll get a runner typically
maybe to do jogging on the spot for a minute or two in the morning if that's pain free and a minute or two in the evening because we do think that a little and often approach is better for bone adaptation that it the bone responds better to short periods of impact loading separated by rest than it would do with doing a lot in one go so that would be an approach I would tend to use and it's not been studied a lot in terms of the research but what I'm tending to see is runners often
come in we do the impact tolerance testing maybe they're they're managing jogging on the spot but bounding and hopping a painfull we send them off doing a couple of weeks of simple impact loading for twice a day and they come back in these impact tolerance tests have improved improved often to a level where we can actually restart some running paps getting on the treadmill and start that return to running process now it may be there in more complex cases that you would want to go for a slightly more detailed bone loading program perhaps something like
this now this is a design so that we've got a straight-line impact that runners need to get used to we've got balance and weight-bearing work and we've got directional impacts it was stressing the bone in a number of different ways it starts with very easy levels of loading so useful for irritable cases so mat may be marching in place single leg balance and sidestepping and then once people are managing a minute or two of these without pain we go up to the next level so we perhaps go up to some to four impacts and jumps
and some skipping and a long time student single leg squat work and side to side jumps again with both feet if they're managing that we can go up to jogging on the spot and side to side jumps from one leg to the other and then on to bounding to drills like a skips maybe slalom jobs and cutting drills and eventually onto hopping and even multi-directional hopping where that hope being that once they're tolerating repeated hopping they're certainly going to be ready to build that running so that would be a sample bone loading program not necessary
for everyone to go to that level we've got someone who's had a history of multiple bone stress injuries or recurrent medial tibial stress syndrome you really might want to use that to stimulate the bone to build tolerance for loading in multiple different ways so obviously said little and often is going to be best for that approach now I would recommend as well including strength work in your management of media type of stress syndrome we think one of the things that is provocative for the media tibia this sort of bending force on the tibia during impact
and we think the calf complex helps to reduce that bending force so I will nearly always include some kind of calf strengthening program in a patient with medial tibial stress syndrome well I may well strengthen up other muscles that we know manage a lot of load in running as well such as the quads and the glutes and there is some evidence of glutes your weakness in media tibial stress syndrome particularly in women so that might be another area that we could aim to strengthen up now if we can make the muscle stronger the theory is
that helps to reduce the stress on the bone but also by doing strength work that in its own right will stimulate the bone and hopefully improve its load tolerance so it's a real win-win including strength work within our program now once we have these things in place and we've established that this person has enough load tolerance the next step might be to consider a gradual return to running you know perhaps they're managing these impact Orient's tests they're bounding jogging the spot hopping etc they're doing fine with those now we start this gradual return to running
and again it's going to be ideally with minimal pain because if we keep running with pain it just tends to stir things up now we want to think about how we're going to do this quite often will use walk breaks initially but you can in irritable cases because it seemed to help symptoms but also we think the T is a factor in medial tibial stress syndrome and bone stress injuries in general so if we utilize a walk break perhaps every couple of minutes or so it helps to reduce the fatigue and facilitates that return to
running then we start to build a continuous comfortable easy running and we build that distance up a bit before increasing intensity with medium intensity work like tempo running and eventually high intensity work maybe track sessions so we're planning this really gradual return to running that exposes our bone to load but a level that's very manageable in terms of symptoms now as with many things there is a bigger picture here we if we think of me do tubular stress syndrome as a bone stress injury then we need to think about things that influence bone health so
that would definitely include things like diet very important past medical history medications that they may have taken bone stress injuries can present in amongst a whole host of other conditions things like relative energy deficiency syndrome so we really want to be able to see the bigger picture here and recognize what might be influencing bone health sleep and recovery are also very important for bone health as we think some of the remodeling of the bone is going to occur during our sleep so it routinely ask athletes about their sleep how much they're getting and the quality
of their sleep and hopefully we can optimize that to improve their recovery and then think about recovery more broadly when other persons rest days when of this athletes recovery weeks because if we think fatigue is going to increase bone stress then we need to manage fatigue by planning recovery appropriately so think about the bigger picture here in your athletes with medial tibial stress syndrome especially those recurrent cases that aren't getting better we certainly work with some athletes where we found that sleep is a real big problem or they're just simply not getting enough recovery so
final thing we might add in perhaps would be some gait retraining now our strategies here broadly divided into ones that might help to reduce the stress on the bone such as strengthening up the muscles and bringing the training down to a manageable level and strategies that might help to improve the bones capacity to manage loads such as a bone loading program and improving sleep and recovery now gait retraining may work as another strategy to reduce the stress on the bone by altering the gait very slightly so the two probably most likely strategies you would use
here is if you have a runner's over-striding you could increase this step rate because that may reduce tibial load and if you have a runner with a very narrow stride width you can increase that stride with slightly using some simple cues and that may reduce medial tibial stress this is evidence and narrow stride width will increase medial tibial stress so we might bring that in once we've got those other strategies in place so I think important things really are more around getting the exercise at pain-free manageable level bringing in some progressive strength and conditioning and
a bone loading program and then planning a graded return and thinking about the bigger picture I think the gait retraining is more of kind of an icing on the cake thing that you're going to bring in a later on when you've got these other strategies and finally with this and we can team up with our podiatry colleagues and see if maybe some also sees may be of help now the theory here is not that we're trying to correct some faulty foot position or anything like that we've moved away from that idea it's more thinking that
perhaps some ortho sees may help to reduce the stress on the medial tibia at least in the short term and therefore reduce the irritation a strategy that maybe parallels with things like our gait retraining in reducing stress on sensitive tissue so that's a whistle-stop tour of medial tibial stress syndrome as you say we think it's a bone stress reaction so really key to get the stress on the bone down to a manageable level and improve its capacity through bone loading programs through strength and conditioning and through a progressive return to running but don't forget that
bigger picture as well okay thanks for listening bye for now