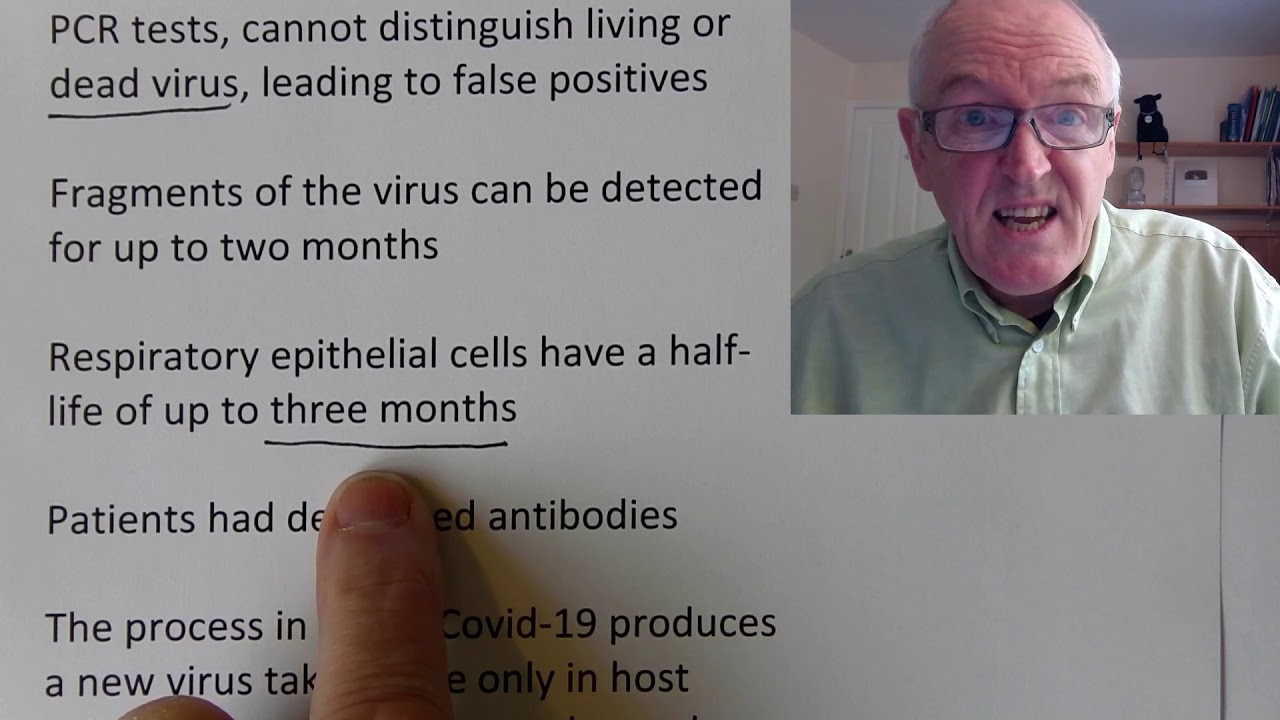
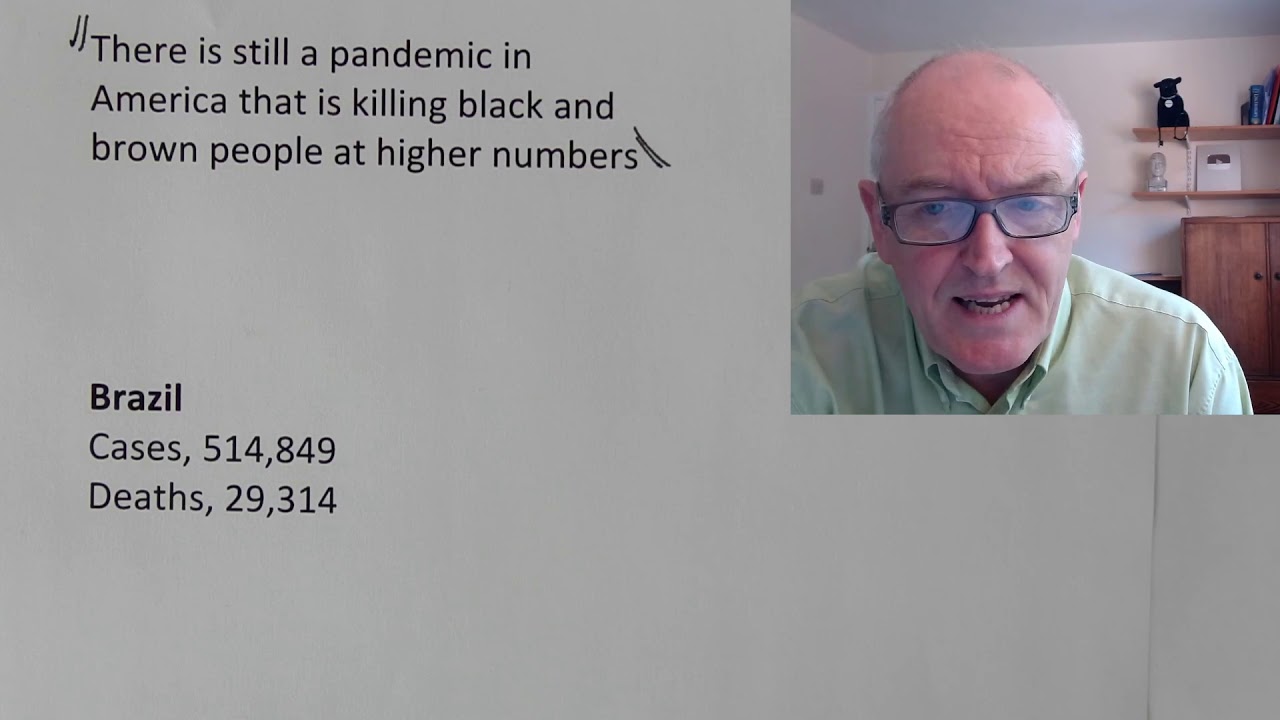
so these lovely children here are waiting for food distribution in Kenya that's made available in some areas for poorer families and they're waiting with great dignity they're all wearing masks there correctly socially distanced and they're behaving perfectly and of course queuing and waiting patiently is actually quite hard when you're when you're hungry but this is what they're doing now this is a protest in the Philippines against the new Nationality Act and we see the the great dignity with which the protesters are protesting and we see that they're socially distanced we see that they're disciplined but they're still exercising their democratic right to protest in a dignified safe way they're outside they're wearing masks they're socially distanced this is a safe demonstration and the same here this is another safe demonstration so this young lady is wearing the full protective visor everyone is wearing masks everyone socially distanced as they make their political point welcome to this weekend's update now the so many things I would like to talk about this morning there's the increased cases in the United States this is the frightening severity of severe cases in in Yemen and how quickly individual patients seem to deteriorate there's the growing tragic situation in Brazil and Peru with increasing cases but unfortunately you're looking at my team I am the the research team and the presentation team and indeed very often the technical team so I've got to be very selective about what I do it just can't do everything so what I've done today and I want you to stick with this video this is one of the more important videos I've made now way back in January I was talking about this pandemic I was talking about the 1918-19 pandemic of course I got slammed for daring to compare these two pandemics how do I possibly say that this pandemic is similar to the 1918 pandemic which of course killed but words are 50 million people maybe as much as a hundred million people no one's quite sure and then I was slammed for saying is pandemic and causing fear and all sorts of things like that so but that doesn't bother me too much because unfortunately that the things are predicted back in january/february are coming to pass now and all it's not that I'm any special powers I just looked at the transmission characteristics of this virus and there's something else that's now come to my attention based on the transmission characteristics of this virus that I want to set share with you this morning now we know about case fatality rate so case fatality rate is the number of people that die related to the number of people that are diagnosed and we've seen that this has been fairly high in some European countries but we knew there was a lot of people that were undiagnosed that weren't picking up in this statistic so perhaps a more useful statistic is the infection fatality rate and that is the number of people that die related to the number of people that are infected and as we've seen some countries that might have a case fatality rate of say 10 percent from the diagnosed cases end up having a case fatality rate of perhaps nought point eight percent sorry an infection fatality rate of no point eight percent so the infection fatality rate is way lower than the case fatality rate because this depends on diagnosis but this depends on mystically knowing the number of people that are infected and of course we won't know this for sure until we have very Universal antibody testing so we know the the infection fatality rate the IFR is lower that's the first point to make now what I wanted to look at now a couple of studies that make predictions based on this infection fatality rate now this is based on this study predicted covered 19 fatality rates based on age sex comorbidities and health system capacities so what this study is not just before that center for global center for global development now this is an international think tank it's based in the United States it produces very high quality very well researched publications it's partly is funded by various governments and agencies around the world for example the Norwegian government recently gave it five million dollars such as is its ability to do useful work so that's what they're looking at now my way background here we know of course that older people are more likely to die younger people are less likely to die we know that men are more likely to die than women we know those with comorbidities for example from the South African data we looked at over the past couple of days we saw that people with HIV are about two-and-a-half times more likely to die if they can track covered 19 we saw that people with uncontrolled diabetes and managed diabetes and high blood sugar levels were about 13 times more likely to die we saw the people with high blood pressure about one and a half times more likely to die these comorbidities and the some of these have been quantified to a fairly good extent and we saw that in that very very useful South African stood a yesterday from the Western Cape health authorities so we know about these things but we also know that perhaps 80% of people are going to get a relatively mild illness so about 80% they're going to get a fairly mild illness that people to go that or even be asymptomatic about 15% of people are going to be quite poorly they're going to get a more severe illness but about 5% of people are going to be critical and for these 5% of people that get critically ill the quality of health care that they get will determine whether they live or they die it is very simple because they're going to need medical help to survive so for example they're going to need oxygen therapy they might need pressurized oxygen therapy such as CPAP or ventilation they might need intravenous fluids for their hydration they might need intravenous antibiotics for their Co infection they're going to need quite a bit of support but these people are also going to need quite a bit of support as well although they probably survive without the medical support but a lot of these won't and how well these people survive depends on the quality of the medical facilities so we see that the likelihood of survival for any given infection depends on how old you are what sex you are what comorbidities you've got and what access you have to health care there the PHA four main factors determining your likelihood of dying or surviving so how old you are what sex you are what comorbidities you have and what access to health care you have so this study was looking at that taking that information into into cognizance now what they found was when they looked at that that the fatality rate from covered 19 varies greatly across countries now this is to be expected because some countries have a younger demographic there would therefore would expect less people to die some countries have more old people therefore would expect more people to die for those compared to the number that are infected some countries have mo more comorbidities for example we looked at South Africa with okay over 8 million cases of HIV so that's what we would expect so we're going to look at that in some detail I wanted to look at this now this is from The Lancet Global Health and again never take my word for these things always look them up for yourself I always supply the full notes and the full references and this is early estimates of the indirect effect of the coffered 19:00 pandemic so we've just said that there's going to be these direct effects people that are going to die as a result of the covered 19 but this study before we're going to look at the direct effects is looking in the indirect effects and a very keen we don't forget indirect effects so these are early estimates of the indirect effects of the cough in nineteen pandemic on maternal and child mortality in low-income and middle-income countries a modelling study now of course the whole process of pregnancy and delivery and the post delivery period is is replete with potential medical complications and this is why there's a high mortality rate in areas with poor poorer health care facilities in this particular field and then this is a well known this is a well known a problem throughout the world I mean that there's so many things you could talk about here one is the problem of what's called calf on the pelvic disproportion where the head the calf will apart the head of the child is too big to fit through the the opening in the pelvis of the mother because the mother was malnourished as a child and that can lead to obstructive pregnancies and all sorts of horrendous problems if medical facilities are not available but that's a slightly separate topic and maybe for another day but these are indirect effects now what we have is throughout the world there's a relocation of health care resources in the developing world now this is happening in in in my country as well where people are behind on things like chemotherapy and it's causing problems but the relocation of healthcare resources in the developing world is a huge issue and I've said right from the start of this pandemic that the people that are going to suffer most in this world are going to be the poorest people those in poorer less developed countries are going to be the ones that end up suffering most and I still think that's true and this is something I feel remarkably strong about strongly about the people in Africa and the people in poor parts of Asia and the poor people in South America just because they might look different from us just because the color of their skin is different from ours just because they speak a different language to us just because they have a different culture to us does no way influences their humanity these people are 100% human the same as we are they are our brothers and sisters all humans are very closely related and yet these people are going to disproportionately dolly and I just find it outrageous that we have whole groups of people around the world that are going to die just because they happen to live in a particular area or because they happen to be of a particular race and huge numbers are going to die in and I'm going to give you evidence for that and I'm just hoping that this video can go some way to preventing some of these deaths so these reallocations are being going on and this could contribute indirectly to over 1 million additional child deaths right Starlin said one death is a tragedy at least is it reputed the same one death as a tragedy a million deaths is a statistic and the poor people in foreign countries anyway you see this is just terrible this is baby human being babies we're talking about here each one of irreplaceable value and yet a million of them could die from these indirect effects because of lack of resources in addition to that there could be five hundred fifty six thousand additional mothers who could die and of course the mothers are young women for young people to die is a tragedy the trouble is in very many of these poorer areas they can either spend their resources on maternal care or they can have an unmitigated pandemic which is also not a good thing so we need an urgent review of health care provision around the world and really actually health care is actually quite cheap you know you can train up absolutely I've done it myself I've trained up absolutely brilliant nurses in various places it doesn't actually cost that much and they can save lots and lots of lives every day it doesn't actually cost that much a lot of the basic things are quite simple and yet the resources are simply not there for that meaning that people who just happen to be a different color from me just happen to be in a different country from me just happened to be a different race from me and of dying massively increased rates and it's just not acceptable now getting back to the main thrust of today's lecture or today's video what have you uncovered so I gave lectures for 27 years it's just bad habit doing what intend to lecture your eyes Julian infection fatality rate is difficult to quantify in many low and middle-income countries now why is infection fatality rate difficult to quantify well it's difficult to quantify it in my country and in Western countries never mind anywhere else now part of it is non-random testing now we had random testing that would be more representative and we could extrapolate into larger numbers but we don't have tests the testings not random so non random testing gives skewed biased data very many countries have incomplete vital registration system so we don't know who sick people could get sick and dying official statistics would never know about it estimates the estimate the adjustment to accelerate estimates from infection fatality rate right so this is saying it's difficult this paper saying it's difficult to estimate the adjustments required to extrapolate the estimates of infection fatality rates that we know about such as we do know about in high-income countries it's high to extrapolate that to low-income areas so just because the infection fatality rate is say so in my country is going to be a say naught point 8 percent that doesn't mean to say it's going to be that in in other countries it could be higher it could be lower it's difficult to extrapolate and that's the really clever thing about this study now I've read this study and it's it seems to me to be quite a superb study and don't pretend to understand it all it is quite mathematical there's mathematical models in place I think I understood enough of it to get the gist of it and to realize it's a reliable study so this is hard to do it's hard to say well these are the figures in the UK therefore this is what the figures will be in South Africa that's hard to do but the team are attempting to do that with some degree of success I believe so the account for differences in age the differences in sex and the differences in relative comorbidities which of course we know are the main factors will come on to the health services in a minute these are grounded in fatality rates from countries with advanced healthcare systems so the data we have is from countries with advanced healthcare systems where of course we can treat the poorly people so this paper tried to make adjustments to adjust for poor quality healthcare so their adjustment reduces the the demography based advantage now what they're saying here is these poorer countries have got a younger demographic there are more younger people because a lot of the older people have died already which is another tragic story of course they shouldn't have died about it they should still be enjoying their retirement but they're not they're dead and that's for many other reasons so so had been thought that the younger demographic in poorer countries would mean they have a lower infection fatality rate but when they add in the effects of lack of healthcare the adjustment reduces this demographic advantage now this is where I want to give you some specific examples of this let's get rid of me right so for example sub-saharan Africa that there's a billion people now if they had the same death rate taking into account age sex and comorbidities then their infection fatality rate should be 11 in a thousand 0. 11 so in other words for every thousand people that get infected you would expect 11 to die based on the data from Western countries nor point 1 1 percent but when they are just that for the lack of health care that jumps up to naught point 4 3 percent because remember 80 percent get mild illness 15 percent get more severe illness 5 percent get critical and how many of these survive or indeed if any of these survive and how many of these survive depends on the quality of health care so if you take away good quality health care many more of these will die so using very advanced mathematics and clever modelling they've worked out in sub-saharan Africa we can expect the infection fatality rate to be naught point four three percent pretty hard numbers Latin America South America 430 million people now given the demographic given the comorbidities given the age profile the sex profile we would expect the infection fatality rate in Latin America to be nought point three nine if they had the same health facilities that we have in more advanced countries that's what you would expect but this data shows that's going to be much nearer one percent in fashion fatality rate so nought point nine five is going to the infection fatality rate in Latin America much higher because of the lack of Health provision Eastern Europe including parts of Russia it should be nought point six eight should be the infection fatality rate you can see it's quite a bit higher than sub-saharan Africa for example because of the the older demographic so Eastern Europe 209 million people it should be nor point six eight percent but because they don't have access to the health care facilities of having Western countries that should be turn out to be one point eight three percent because of the older demographic what more people are going to die so this is these are quite startling figures really now what I want to do now is actually run through a few a few real examples here so I'm just going to give ourselves a bit more magnification if I can there we go now hit hit here's the first here's the first group now Western sub-saharan Africa now so this is countries like wool Nigeria Ghana Sierra Sierra Leone like Liberia would all be Western sub-saharan Africa now this graph is very clever what this team have done now this gray pipe so first of all the total height of these lines represent the demographic going from younger to older so this is the number of people in the demographic so we see there's more younger people there and less many fewer older people there so younger people also I'm not quite sure it is ten twenties 30s 40s 50s 60s 70s 80s 90s that kind of thing in fact I think that's what it is so the height of that line shows the number of people in that demographic this dark line at the top shows the number of people with comorbidities in that demographic so as you would expect as we get older we see more people with comorbidities so for example if we look at southern sub-saharan Africa here we can see that quite clearly so in this in the younger demographic few people have comorbidities but as we get into the older demographics a much higher proportion of people have comorbidities till here and here is more than 50% of comorbidities so they're the things that are going to influence death primarily and they've taken into account the male-female distribution here as well of course and what they work out for these Western sub-saharan countries is that the infection fatality rate should be around 1. 1 percent but when you adjust it for poor health care facilities it's going to be nought point three percent because based on this this amounts are based on these comorbidities here and based on these demographics here they estimate that in this population one point four what one point four three percent are going to get serious disease so that's the number they're going to get severe disease and of that forty forty M 0.
43% will probably die so what I've done just as an example if I've taken these three subsets these are sub-saharan African countries so this is Eastern Eastern and this was Eastern sub-sahara so that's like Kenya Tanzania Uganda Somalia Eritrea this one central sub-saharan Africa so Chad Sudan Congo Cameroon South Sudan so did you just taking those countries anyway for example now what that adds up to if we have those three areas together and we look at the we look at these overall figures so this is the number of people would expect to get critical in these areas here that's the number it would get critical normally they'd all be saved but we can't save them all because you have got the health care facilities in these countries so what that means is that's what the case fatality we would expect in that area that's what is suggested for after we look at the lack of health facilities because of that number of severe cases and it turns out there's this one 0:09 that's just over a billion people a thousand million people in that area now this this this next bit is crucial to understand if this disease carries on reading it will carry on spreading till 70 or 80 percent of the population are infected then there will be herd immunity and I think we know that from previous videos so what that means what that means is 80 percent of this 1 billion people could get infected and that works out to 807 million people could potentially catch this virus and as we see about noir point 4 3 nought point 4 4 Sonor point 4 3 of those end up dying that were meaning in this area 3 point 7 million people are going to die in this area of sub-saharan Africa so just in the area of sub-saharan Africa this data indicates there is the real possibility for 3. 7 million people dying as a result of this pandemic that's going down so if we take this area here southern sub-saharan Africa so southern sub-saharan Africa here yeah so again that works out if you actually work that out South Africa in places like that so this is the number of people there there's there's 80 eighty two point three six million people in this area that number of people two point six six could become critically ill naught point six nine percent could be the adjusted infection of fatality rate because of the lack of access to healthcare services and that would work out at in this area alone that would work out at five six five a nod five hundred sixty five thousand people potentially dying in that in that area South Asia here so this is countries like India Pakistan Bangladesh and we see there's already quite a lot of older people here and there's quite a lot of a pre-existing comorbidity that we see taking that into account that means severe cases could be two point three three percent of the population that will give an adjusted infection fatality rate of naught point nine percent which would mean that there could be twelve point nine people or twelve point nine million people that would potentially die in this area based on this data now the other thing to bear in mind here is these figures are also going to depend on how quickly these cases occur so we know this we know this famous graph here now that we've looked at it many times so we've got this graph here and what this graph is is in the middle so this is increasing number of cases here and this is a time along here now the Health Services in most countries have an ability to cope with a certain number of cases that's the number of cases the health services can cope with so as our cases increased in the UK we managed to keep the numbers down so the health services could cope and now the numbers going down so that was the whole aim of this game now if game hardly a game that was the whole aim of this strategy if we hadn't taken lockdown measures then our numbers would have gone up more quickly like that we would have had that sort of pick what we have in in these poor countries where there's limited health services is the numbers are going to go up and even if the numbers go up slowly they're still going to overwhelm the ability of their particular health services to cope so obviously the number of cases that a poor health service could cope with will be will be much lower so those cases would be exceeded or the quicker even if it was a relatively low number so even if the numbers have been the same as they were in the UK in that line there then their health authorities would still I've been overwhelmed but what is going to happen it happen is that the case they're going to grow rise much more quickly than this as we see for example in Brazil at the moment it's going to take a while for them to go down and remember this line here is the ability of their health services to cope that line there so we can see they can cope with these people here and they can cope with these people here if they get into the hospitals and we saw that tragic case just a couple of days ago on the video of a father who couldn't get into the hospital but that means all of these cases here are going to be above the ability of their health services to cope in those particular in those particular countries this is why we're looking at such large potential and such large potential fatality reigns now going on to look at some other countries so here for example we have a Latin America these are the latin-american countries so we've got Latin America Latin America and Latin America they're these three areas of Latin America the way they're classified the countries here is a bit old-fashioned actually to tell you the truth but we can we can work it out so for example what we have here is uh these Latin American countries so anyone take these Latin American countries there so if we take those Latin American countries there so we've got 685 there 62 there oh no that says you're sorry that's it 60 to 62 million there turns 58 million there 100 219 million there so those those three countries there that comes to a total of five hundred and thirty nine million eighty percent of that number of eighty percent get infected is 431 million and that will give a fatality rate based on these figures here love so there we see it's 0. 92 there we see it 0.
97 there we see it's one point zero two so that's going to give us an infection fatality rate of about 4.