hey everyone Dr Jake Audi so this is video two in a series where I'm breaking down this paper here this is a piece of research that I was involved in so make sure you go back and watch uh the video one in the series and that goes through the justification for This research and some of the early results now the first results that we get from figure one is that there are a small group of non-steroidal anti-inflammatories very common drugs that inhibit the enlar P3 and flammasome and not the other inflammazone so this is a
semi-selective nlrp3 inhibitor and there are a small group of NSAIDs that we know are safe to take so it's very exciting research in the next couple of figures I'm going to break down how these drugs work now this is always a terrifying thing to and try and do discovering how a drug works is incredibly difficult paracetamol which we've been taking for decades and decades and decades we only really probably figured out the mechanism in 2017 and we're still not 100 sure but we think it might be something to do with cannabinoid receptors in your spinal
cord after being digested by the liver so paracetamol gets digested by the liver into another drug and so it's a very complicated pathway so when we went about this to try and discover how our NSAIDs might be inhibiting in lrp3 we were a little scared this could be a never-ending project now I will say I might just bury the lead a little bit we were very sure by the end of this paper the mechanism of action on how this how these drugs work but it turns out a subtle twist we're wrong and I'll tell you
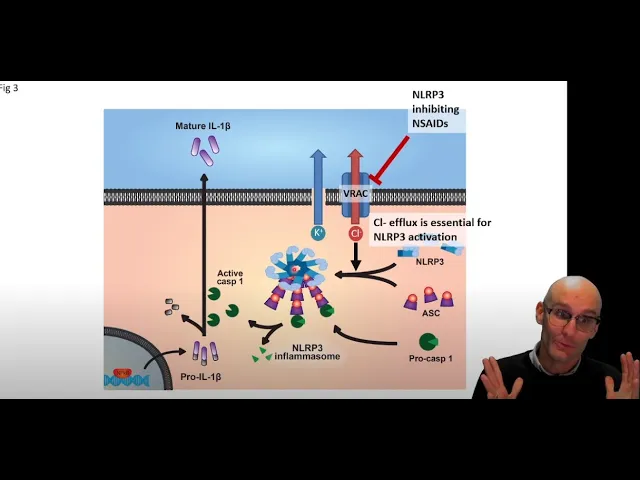
why we were wrong later and we didn't really figure out we were wrong until another four years after we published it so let me jump into it here we go okay so quick refresher we've got the nlrp3 pathway here so first we get NF Kappa B activation that causes the production of pro interleukin-1 beta which is not an inflammatory form of interleukin-1 beta it has to get cleaved first it gets cleaved by caspase one the enzyme but carespace one is is also in an inactive form called Pro caspase one now Pro Cast space one has
to get activated by typically the inflammazone so the inflammasomes will activate Procare space one including the inner rp3 inflamazone now the nlrp3 inflamism detects the perturbation in the cytosol it then oligomerizes into a ninja star it then recruits an adapter molecule cured ask and it recruits thousands of these ask molecules and each ask molecule can recruit a procat space one molecule and activate it so this is the inflammer Zone there now largely there are two critical ions involved in here we need potassium eflux so we need potassium to leave the cell and we need chloride
to leave the cell so the question is with our drug we are in the pathway is it inhibiting we know it's inhibiting in lrp3 we're in the pathway is it inhibiting iron flux is it inhibiting enol rp3 activation or ask recruitment or somehow care space one activation where in this pathway is it being inhibited so first up we wanted to look at ask ligamerization this kind of answers in lrp3 and esque simultaneously so to do this we took macrophages we genetically engineered them to put a fluorescent Probe on the ask molecule here so instead of
just being a regular ask molecule it now fluoresces either under a green or a red light we had both now what's cool about that is ask is normally floating around the cytosol but when it gets activated it forms this large clump it's actually microns wide it's as big as the mitochondria it's huge and so we can actually watch these specs form using live cell microscopy after we activate these macrophages and activate the inflammer zone so here we can see under normal situations you can see all the askers diffuse that's a whole cell there pretty much
so cytosol of a whole macrophage there so these diffuse blobs are just macrophages expressing the fluorescent-esque now when we activate them with ATP for example we end up with these type bright specks can you see these specs in each of these cells here there's a good cluster of them we tried to point to them a little bit because um in the in the paper you have to shrink the images so much but yeah you can see that there might be about 12 or 13 different specs on this page it hasn't happened to all the macrophages
but some of the macrophages have these very large specs in now with ibuprofen which is a no doesn't inhibit the inflammazone we can see we've still got all these bright white specks throughout the image but flu phonemic has that we have no specs we've still got that diffuse looking macrophage so the esk is not a ligamerized under flu phonemic acid so when we quantify it um speaks per um per image basically um and we express it as a percentage of vehicle we can see that Ibuprofen has the same amount of specs whereas methanamic acid and
flufenamic acid have both inhibited ask spec formation so we've inhibited the formation of those inflammosomes so we know it's not this path we know that this is inhibited which would suggest that it's Upstream so maybe it's in lrp3 or maybe it's the chloride efflux but we did also just want to check to see if some Outcast phase one was being activated if we were right at that conclusion was correct that we have blocked inflammosome activation and the formation of this ninja star we should see no Active Care space so to do this we used a
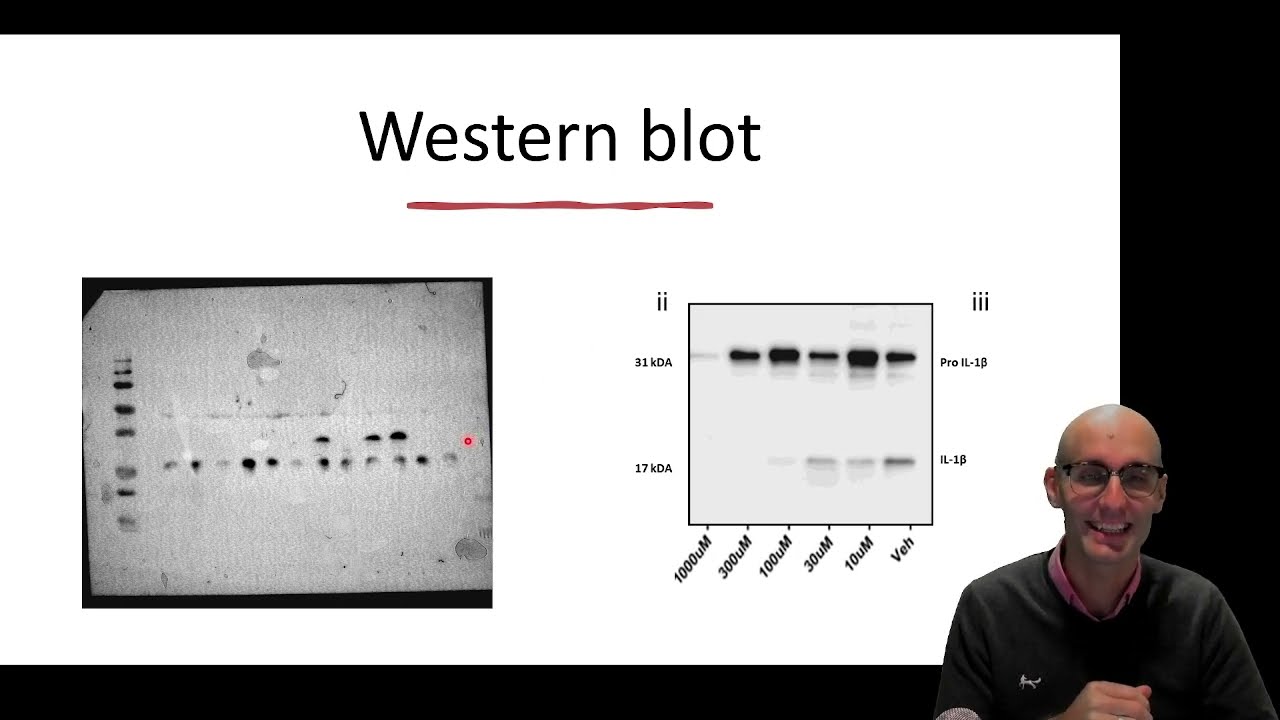
western block which sorts proteins by abundance and size and we did a western blot for caspase one we were looking to see whether the pro domain had been cleaved off so now we had active caspase one so we know it's not this is the case based one and so to do this we do a western block now this is the dirty Western bot we actually got way better at these Western Lights it was very hard to find a good antibody and all this kind of stuff but this is staining for caspase one and we know
that this active caspase best correlates with this fragment here it's the 10 kilodon fragment of caspase one now thanks to Kate Schroeder's work up in the University of queensome we actually know it's not this fragment that's active but we do know that this fragment correlates with caspase one activity it's it's sort of a pre-digestion uh form of the caspase that's active and then I guess digested down to the 10 kilodol and so it correlates well with the activity of care space one if this blob is darker we know that caspase one is more active so
um and when we don't activate it this time we used a bacterial toxin to activate the inflammasome called Nigerian when we don't put Nigeria sun on we don't get Active Care space one when we do put Nigerian on here we do get caspase one so if we have a look there when we've got Nigerian and no other drugs we do get this active caspase-1 fragment when we look at ibuprofen it has gone down just a little bit just a hint of activity there but not significantly their dark blob there is still roughly the same size
as this maybe a little bit further down but not too bad um but then when we look at fluvidemic Acid we've completely almost completely got rid of the active caspase one component of this Western blot and so well man we made the blocks way better later on I wish we could republish our data um and so we've sort of confirmed this again and again and again with less speckle and all this kind of stuff there's a lot of optimizing to Western blocks um but yeah we can see fluvonamic acid is blocking the formation of active
caspase one oh look at that okay so next um I didn't expect that okay so next we wanted to figure out okay it's interacting with something I don't know we still don't know what we know it's blocking the spec formation we don't know if it's directly binding to the spig or what's going on there next we kind of wanted to figure out maybe because we're trying to narrow it down and we're still and in nowhere we just know that in lrp3 is inhibited we sort of narrowed down any specific proteins it could be a never-ending
hunt but we kind of wanted to know what kind of inhibitor it is so there's two major kinds of Inhibitors um there's a a drug inhibitor might come in and occupy the spot that the normal signaling molecule will work through or it'll somehow bind to the protein and prevent it from making that conformational change so if there's an enzyme that might fit into the enzyme without cleaving if it's a receptor it might fit into the receptor like this without activating the receptor so that's a drug inhibitor and so it might be doing this now there's
two kinds um and so now you can see the signaling molecule can't get into the pocket because it's been occupied by the drag inhibitor now sometimes drug Inhibitors can be irreversible and that means that they may be permanently bind to their targets so they really lock themselves in here we've got this binding to that receptor there and so then you can't wash it out you can't get rid of it and it's not until that protein gets digested by the cell and a new receptor is produced that that drug will stop working so these are very
potent long lasting drugs because they permanently bind to their drug Target and that's called an irreversible inhibitor now a reversible inhibitor is different it will go into the pocket but then it will come out of the pocket and then it'll go back in in the pocket and so they'll actually kind of take turns between the signaling molecule and the reversible inhibitor and what you can do is saturate it with reversible inhibitor so that more often than not it's another drug that comes in and replaces the drugs so there's far more drug than signaling molecules so
you drown it out and that's a reversible inhibitor so we wanted to know that and so what we did was we did our macrophage prep where we did the macrophages treated them with LPS treated them with ATP but we treated them without drugs before we treated them with ATP and then we tried to wash our drugs off so we treated them with the drug for five to ten minutes and then we did three Replacements of the media to really wash our drug off and then we gave the ATP after we'd done their washing to see
if we could reverse it right so here we can see with no wash flu phonemic acid is very potent so when the drug is there when we try to activate the inflammasome it's very potent but when we wash it we can wash it out so we can wash out flu phonemic acid now in this experiment and we can wash our methanamic acid in this experiment we had a reversible inhibitor this is a caspase inhibitor that we know is a reversible one and we had this drug M and S which we know is an irreversible inhibitor
it binds permanently to its drug Target and so it didn't wash out and so this was really nice confirmation that we had a reversible inhibitor it was inhibiting something not sure how but it is at least reversible that's helping to narrow down potential targets there so next up we wanted to look at these iron fluxes potassium and chloride and we actually got some collaborators involved who could do electrophysiology so they could actually measure based on the manipulation of the electrical currents in these macrophages they could measure where the where the positive cation flux was still
occurring or negative iron flux was still occurring in the presence of the drugs so this group really helped us out in figuring out which ion may be being interfered with with our drug so first up they looked at potassium influx so this is a positive ion so they're looking for positive iron flux and what's happening to that in our macrophages when we uh with and without the drug and what we can see at 100 that's our control and so both the fluvidemic acid and mefenamic acid are not significantly different from our control so they are
performing they're having the exact same amount of potassium flux or positive iron flux with the treatment of fluconamic acid and methanamic acid as our control so this suggests these drugs are not modifying potassium efflux so we know it's not potassium reflex next they look at chloride flux or negative iron flux is probably more specific and what they saw there was that fluvinemic acid and mefenamic acid actually inhibited negative iron flux whereas ibuprofen and diclovenac had no effect on negative iron flux so here we found out something quite important and pretty cool we've found out that
in lrp3 uh in lrp3 inhibiting uh NSAIDs were inhibiting negative iron flux which is awesome suggesting that we were modifying chloride flux and that was what was modifying the nlrp3 inflamazone a real important Point here is that the literature hadn't quite established that negative iron flux was critical to nlrp3 so this was a really surprising result is we were starting to be some of the first people that were drug targeting this negative iron Flex in order to Target the enlar P3 inflamazone very very cool stuff now there's a lot of negative ion channels that might
be responsible for this negative iron flux but one that we thought might be is a a channel called b-rack or volume regulated anion Channel anion mean negative ions so it's a volume regulated chloride uh Channel basically so could it be this guy so next we did a couple of experiments what we did was we did flip phonemic acid methanamic acid and here we did a chloride Inhibitors these are non-specific drugs that inhibit chloride channels and we found that they also inhibited the inflamazone so this is a really important step it shows that just inhibiting all
chloride flux does inhibit the enlar P3 inflamasone as I said the literature hadn't really settled on where the negative ion flux was critical in the inner lap E3 Activation so it was really important for us to show that but next we actually found a drug that is a supposedly very selective b-rac inhibitor so it just inhibits this one receptor volume regulated anion Channel essentially what this channel does is as the cell begins to swell up the volume regulated anion channel will open up to allow chloride to eat to leave and with osmosis where an iron
goes water goes so water follows ions so salt sucks that's osmosis so as does chloride ion leaves water will follow it so the idea is that as the cell stretches the channel opens that allows the chloride out and then the water goes out with it and then it allows the cell to relax right so um yeah we tested the specific v-rack inhibitor and it too inhibited uh io1 Beta release so we've got i1 Beta release here when we put the ATP on which we know aggravates it uh in lrp3 we get io1 Beta release and
when we put the specific v-rack inhibitor on it blocks it so our drugs are acting exactly like v-rack Inhibitors and this is sort of the first time the v-rake have been specifically identified as an nlrp3 inhibitor and targeted with drug targets so it was a very very exciting result um and so uh figure two and three we're in the pathway are inside in lrp3 Inhibitors working we think it's likely a reversible v-rack inhibitor preventing chloride reflux and this inhibits enlarp3 activation and ask spec ligamerization which we showed with the fluorescent tag and caspad's cleavage which
we showed with the Western block and so yeah this is where we think our drag is working and by and because chloride flux is a central phenol rp3 activation by inhibiting vrec we have inhibited nlrp3 uh forming now the birds flips in the tail that happened several years later is we generated a v-rack knockout Mouse and they have regular in lrp3 activation um and a half flu phonemic acid still worked in Indianola P3 in a v-rack knockout mice so we're not sure it could be that it is working through vrec and when you knock out
v-rec another protein is upregulated that's very similar to vrec and our uh our v-rack inhibiting insides actually inhibit a range of anion um anion fluxes negative iron e-fluxes so chloride effluxes and actually we're confirmed it time and time again with some very clever experiments involving things like certain um gluconate yeah and some very specific experiments we've shown that chloride efflux is definitely essential for inflammozome Activation and v-rank is probably involved as one of the channels that allows anions the problem is is that there's probably lots of channels that allow chloride efflux and that our drugs
just happen to block all these channels so it seems like a dirty drug and a dirty process allowing lots of chloride out through a lot of different receptors there there's just a little twist in the tail what happened about three or four years after we published this paper