what up lovely people this is mitochosis perfectionist where medicine makes perfect sense let's continue our endocrinology playlist so in this playlist we talked about anatomy of the endocrine glands embryology biochemistry now it's time to talk about physiology please please please watch these videos in order it matters before we continue today we'll go very quickly because most of the stuff has been discussed before if you want a slower pace check out my biology playlist i have several videos on the endocrine system let's go nervous stimulation versus hormonal stimulation nervous somatic or autonomic hormonal is always automatic
you cannot tell your glands to secrete more or less shut up nervous stimulation super fast nerve impulses but hormonal slow nerves are always firing hormones secreted only when needed hormones are secreted when needed in very small amounts we measure them in micrograms or even nanograms meanwhile hemoglobin is measured in grams per deciliter not with hormones we're talking about teeny tiny amounts hormones are highly active could be lipid soluble or water soluble as we have discussed before and they act via secondary messenger system like the g protein for example please refer to previous videos when a
cell secretes a hormone to act on the same cell is called autocrine when the cell secretes a secretion to act on the neighboring cell in the local area surrounding tissue this is called paracrine but when a cell secretes a hormone and dumps it directly into the bloodstream to take it to distant places all over your body this is called endocrine exocrine glands have ducts but endocrine glands are duct less remember the ceo general manager and then employees who is the ceo hypothalamus general manager pituitary who are the employees thyroid adrenal cortex gonads when the hypothalamus
secretes growth hormone releasing hormone it goes to the anterior pituitary tell her to secrete growth hormone or somatotropin soma means body trope means to grow iron protein growth hormone will help you grow growth hormone will also go to the liver to make the loyal sun of the growth hormone known as igf-1 insulin-like growth factor 1. you know why because insulin is anabolic insulin wants your cells to grow also growth hormone is anabolic it wants your cell to grow but when the hypothalamus secretes tomato satin it's a universal inhibitor it inhibits everything including the growth hormone
if the hypothalamus secretes good enotropin releasing hormone it will go to the anterior pituitary told her to secrete the gonadotropins like fsh and lh and then they will go to the gonads in females the gone is the ovary now the ovary will secrete estrogen progesterone and inhibin in males the gonad is the testus and it will secrete testosterone dihydrotestosterone and inhibin when the hypothalamus creates trh thyrotropin releasing hormone it will go to the anterior pituitary and tell her to secrete thyroid stimulating hormone tsh is going to go to the thyroid gland and stimulate it to
secrete the thyroid hormone such as t4 t4 t4 and some t3 when the hypothalamus secretes corticotropin-releasing hormone it goes to the anterior pituitary tell her to secrete adreno for the adrenal cortico adrenal cortex tropic growth hormone acth will go to the adrenal cortex and tell the zona fasciculata to release cortisol and tell the zona reticularis to release adrenal androgens how about the aldosterone from the zona glomerulosa well the aldosterone from the zone glomerulosa is not under the influence of acth the aldosterone is under the influence of the renin-angiotensin system that's why we call it renin
angiotensin aldosterone system next when the hypothalamus secretes trh yes it's the same trh as this one it will tell the anterior pituitary to release prolactin which makes milk its pro lactation but when the same hypothalamus secretes dopamine well it inhibits prolactin secretion that's why dopamine has another name or a nickname it is called prolactin inhibiting hormone or prolactin inhibiting factor and this concludes the anterior pituitary let's talk about the posterior pituitary first of all it does not make any hormones it stores the hormones that the hypothalamus made and these are adh and oxytocin from the
supraoptic and periventricular nuclei and the hypothalamus and then when your body needs them the posterior pituitary is just gonna dump them into the bloodstream but the posterior pituitary did not make them what's the function of antidiuretic hormone to preserve your blood pressure it wants to raise your blood pressure by two mechanisms v1 receptor is going to constrict your blood vessels and of course this will raise the total peripheral resistance which will raise your blood pressure adh acting on v2 receptor will facilitate water reabsorption in the renal tubules and this of course will increase the blood
volume which will increase blood pressure why v like adh where did you get the v from oh because the nickname of adh is called vasopressin because it constructs vessels i will press on those vessels and i will press the kidney to reabsorb water haha oxytocin is the love and bonding hormone it also lets the milk down from the breast to the baby's mouth hypothalamus releases trh goes to the antipituitary to secrete tsh which goes to the thyroid to release t3 and t4 what if i have too much of t3 and t4 they will inhibit trh
release and they will inhibit tsh release this is called negative feedback what if i have little t3 and t4 this will stimulate the secretion of more trh and more tsh from the hypothalamus and anti-pituitary respectively you have to understand the difference between primary secondary and tertiary if the problem is in the gland of concern it's called primary one step ahead is called secondary two steps ahead is called tertiary let me explain let's say that you have low levels of thyroid hormone now the question is who caused it all right who caused it is the thyroid
gland is toast okay so the problem is in the thyroid gland there for what therefore we call this primary hypothyroidism because the problem is in the gland of concern the gland here being the thyroid but what if the problem is not in the thyroid gland the problem is that the anterior pituitary is not making tsh oh now you'll call the secondary hypothyroidism but what if the problem is not in the thyroid and it's not in the anterior pituitary the problem is that the doofus hypothalamus is not making trh we'll call this tertiary hypothyroidism easy cool
what if we have hyperthyroidism same story it could be primary hyperthyroidism secondary hyperthyroidism or tertiary hyperthyroidism the 10 commandments of endocrinology is by far my favorite part of the lecture you have to understand primary versus secondary versus tertiary and then you have to understand the difference between positive feedback and negative feedback all right let's start by negative feedback because it's more common in your body if low t3 and t4 is gonna tell your pituitary to secrete more tsh we call this negative feedback okay what if we have more t3 and t4 and this tells the
pituitary to shut up and release less tsh this is also a negative feedback many students will look at this and say oh this is high therefore positive or this is high therefore this is positive feedback nonsense if the arrows are opposite this is negative feedback low causing a high or high leading to a low both are examples of negative feedback but if increased estrogen release is going to increase lh which will increase estrogen release which will increase lh which will increase estrogen when the arrows are moving in the same direction this is positive feedback an
example of this is the lh surge in the menstrual cycle my gland is hyper secreting we have talked about this before in the pathology of endocrine system this could be an adenoma adeno carcinoma or just hyperplasia the operation manager is the pituitary but the chief executive officer is the hypothalamus the anterior pituitary gland makes and stores but the pistiputeri stores only it does not synthesize anything there are three glands that listen to the anterior pituitary we call these the employees and these are the thyroid agile cortex and gonads their secretions are usually fat soluble therefore
slow as we have discussed before the three independent contractors could not care less about the pituitary or the hypothalamus they are the parathyroid instead of thyroid adrenal medulla instead of cortex and pancreas some hormones will be freely floating in the bloodstream others will be bound on plasma proteins only the free is physiologically active the bound is not active only the free hormones can exert physiological action exert positive or negative feedback or cause clinical symptoms when they are high or low there is insulin land and there is glucagon land all the hormones are in glucagon land
insulin stands alone eagles fly alone and insulin is an eagle it's the land of abundance it's anabolic all the other doofuses are catabolic and we have talked about the tale of two hormones in previous videos secretions versus continuous secretions there are two modes of secretion let's say that your hypothalamus is secreting gonadotropin releasing hormone we can secrete this in a continuous fashion secretion secretion secretion secretion secretion all day long or we can do it in a pulsatile manner secretion and stop boom secretion and stop boom secretion and stop the pulsatile gives you a stimulatory effect
but continuous secretions will lead to sensitization adaptation negative feedback eventually it will not cause any activation of the target organ therefore let me ask you a hypothetical question imagine that a kid is not growing due to deficiency of growth hormone should the doctor inject him with growth hormone once a day or should the doctor give a continuous venous drip of growth hormone of course if you want to stimulate the target if you on the kid to grow give it in a pulsatile manner so i'll inject you today the injection takes like 20 seconds and we
stop and then you come tomorrow i inject you for 26 and stop this is a pulsatile fashion it will stimulate the target organ such as bones cartilage muscles etc so that the kid can grow the distinction between the lipid soluble hormones and the water-soluble hormones was discussed in previous videos in this endocrinology playlist so please pause and review and pause and review only the free is physiologically active that's the good news the bad news is that it's free it's not bound to plasma protein therefore it will be filtered through the kidney and you will see
it in the urine lipid soluble on the other hand is usually bound to plasma protein because the blood is made of water and this is lipid lipid cannot float in water you have to carry it on plasma protein therefore it's not physiologically active when it's bound like this that's the bad news good news it will not end up in the urine for the most part of course but time medicals how about urine cortisol in patients who have cushing's syndrome all right you just said cushing syndrome right patients who have cushing's syndrome have too much cortisol
right and when you have too much cortisol you have overwhelmed the system all of your plasma proteins are saturated that's why cortisol will begin to show up in the urine in abundance the ligand alone is not active the receptor alone is not active only the ligand receptor complex is active they have to hug and kiss each other in order to get activated therefore pathology can hit you here or it can hit you here if it hits you in the ligand we usually call this type one if it hits you in the receptor we call this
type two case in point diabetes type one the problem is that you do not have insulin in type 2 well the answer is fine is that the receptor is not listening same thing in diabetes insipidus it's just different terminology type 1 is central diabetes insipidus no adh type 2 well we have adh it's that the kidneys receptor is not listening see medicine makes so much sense once you understand what the flip you're talking about control of hormones the hormones of course are under hypothalamus control negative feedback and positive feedback although mostly it is negative feedback
because positive feedback is explosive and they are no circadian rhythm for instance cortisol is secreted more in the morning growth hormone is to create more at night why alright cortisol is an anti-stress hormone yep most stressful situations happen in the morning because you wake up early in the morning you go out and into the world you drive like a maniac and other drivers will start cussing at you that's a stressful situation you need lots of cortisol in the morning however when you're sleeping at night you're lying flat down therefore the effect of gravity is eliminated
it's easier for you to grow vertically from head to toe this is your metabolism if i'm going this way i'm burning stuff to get energy break down the carbohydrate into glucose the protein into amino acid the triglycerides into free fatty acids this is called catabolism who's the hero of catabolism glucagon and his friends which include epinephrine cortisol thyroid hormone but if you're going in the opposite direction from glucose to carbohydrate from amino acids to protein or from fatty acids to triglycerides this is called anabolism who is the hero of this insulin alone insulin is anabolic
protein anabolic glycogen anabolic triglyceride anabolic but glucagon is catabolic glucagon is protein catabolic glycogen catabolic triglyceride catabolic not glucagon only but glucagon and his friends in other words insulin alone is in one land all the other hormones are in the other land how about growth hormone growth hormone is in the middle it is borrowing the first characteristic from insulin and the second characteristic from glucagon growth hormone is protein anabolic like insulin it is glycogen and fat catabolic like glucagon what does growth hormone and prolactin have in common they are polypeptides secreted by the anterior pituitary
specifically by the acetopheles and they use the jack stat pathway as we have discussed before i have an entire video about the jack stand if you look close into the anterior pituitary the red squares are the acetophylls the blue squares are the basophils as you see growth hormone and prolactin are secreted by the acetophils all the others basophils look at this lovely growth hormone or somatotropin it has some actions that are similar to insulin and some actions that are the opposite of insulin similar to insulin protein anabolic i want you to build up muscle i
want you to build up carthage and bone how did i do this i summoned my son who's your son it's called igf-1 insulin-like growth factor 1 also known as somato meden c because it's the middle man of somatotropin tell me about your anti-insulin actions growth hormone i will break down glycogen into glucose i will help gluconeogenesis and i will break down the big fat into small free fatty acids this chart was discussed at nauseum in the previous videos here are the effects of different hormones on the female breast estrogen will make the nipple and the
duct progesterone will make the s and i or the alveoli all right these are empty sacs so far who's gonna fill them with milk prolactin because i'm pro lactation who's gonna let the milk down into the baby's mouth oxytocin i have a video on my channel called dopamine and neural pathways if you remember dopamine in the striatal pathway was pro movement if you do not have dopamine you're not moving if you have too much dopamine you're moving like crazy but dopamine in the mesocortical limbic pathway is pro mode too little dopamine i'm so sad depressed
life is meaningless what's the purpose anyway too much dopamine oh my goodness life is awesome third dopamine in the tubero infundibular pathway is anti-prolactin if you do not have dopamine prolactin will run amok no one is inhibiting it prolactin will be uninhibited and will cause hyperplactinemia which will cause galactoria and it will suppress gonadotropin-releasing hormone which will decrease fsh and lh in females this causes amenorrhea in males this causes impotence in gynecomastia in other words impotence in males is equivalent to amenorrhea in females never ever forget this again dopamine is anti-prolactin what if i have
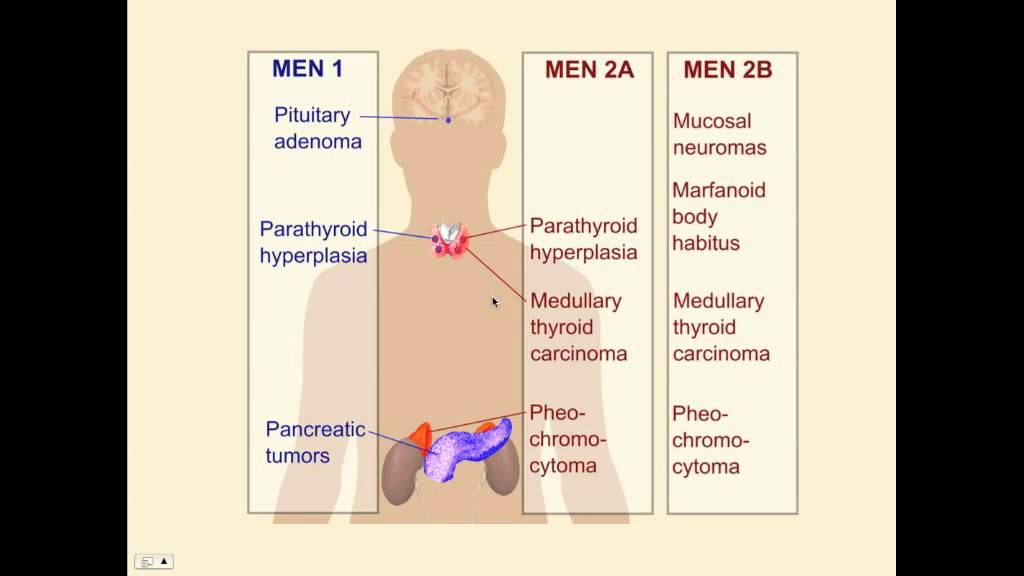
too much dopamine you will inhibit prolactin not just prolactin dopamine hates everybody it hates gnrh and growth hormone as well i had a patient with schizophrenia i gave the patient dopamine antagonists known as antipsychotics one of the side effects of them is well they are anti-dopamine therefore pro-prolactin therefore can cause hyperprolactinemia with all of these symptoms let me give you another case there is a patient who has a tumor in the brain known as pituitary adenoma prolactinoma to be specific his pituitary is secreting too much prolactin how do i treat it you can treat it
medically or surgically surgically is easy you just remove it through a trans sphenoidal surgery how about medically give dopamine agonists something that is pro-dopamine and therefore anti-prolactin to inhibit the prolactinoma such as the medication known as bromocriptine capergulene etc all right keep in mind that prolactin and estrogen hate each other prolactin is pro-lactation but anti-ovulation all right i understand that it's prolactication how is it anti-ovulation it suppresses gnrh and it suppresses lh and fsh conversely estrogen anti-lactation but pro-ovulation prolactin and estrogen are enemies that's why when mommy is pregnant she's not lactating but when mommy
is breastfeeding she cannot get pregnant most of the time not all the time in fact we cannot just rely on prolactin as a contraceptive method at any rate do you know why prolactin and estrogen are enemies yeah easy because lactation and pregnancy are time consuming resource consuming very expensive and draining phenomena that's why prolactin inhibits estrogen okay i'm busy lactating right now the baby is sucking the life out of me do you think i have energy to get pregnant shut up so i'm gonna inhibit lh and fsh conversely i'm pregnant right now do you think
i have any energy to breastfeed shut up so i will inhibit prolactin economics is the study of scarce resources which have alternative uses since the resources are bloody limited we need to economize and we shall continue in the next video i have an otakoids pharmacology course on my website as well as an endocrine pharmacology course learn about the different types of insulin how to calculate the dose etc at medicosusperfectstatis.com thank you for watching please subscribe hit the bell and click on the join button you can support me here or here go to my website download
my courses be safe stay happy study hard this is mitochosis perfectionist where medicine makes perfect sense