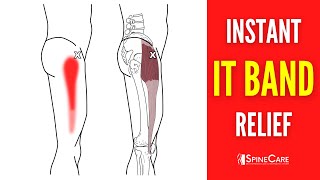
today i'm going to discuss the it band including its anatomy and function review and dispel previously held beliefs outline what's currently known and provide exercises and management strategies for it band related symptoms the iliotibial band commonly referred to as the it band is named for its attachments to the ilium or pelvis and tibia or shin bone it is the lateral thickening of the fascialata which is the deep fascia that envelops the thigh like a sausage casing in addition to its origin at the pelvis the it band receives fibers from two muscles of the hip all
of the tensor fasciae latae and most of the gluteus maximus as it travels down toward the knee the it band firmly inserts onto the femur patella and tibia the expansive nature of the it band allows it to contribute to stability of the hip and knee as well as store and release energy to make bipedal walking and running more economically efficient iliotibial band friction syndrome was first described by james wren in 1975 based on his clinical observations of military personnel experiencing lateral knee pain during walking or running that developed after long distance running or hiking he
noted that all patients had focal tenderness over the lateral epicondyle of the femur which is a bony prominence on the outer portion of the knee ren also discovered that he could reproduce his patient symptoms by having them stand on their affected leg and bending 30 to 40 degrees based on his findings and previous anatomical descriptions up to this point wren concluded that the it band was repetitively rubbing back and forth over the lateral epicondyle of the femur resulting in irritation and inflammation hence the name iliotibial band friction syndrome in 1978 dr arava supported these findings
with 88 patients of his own he described iliotibial band friction syndrome as an exertional non-traumatic disorder connected with increased physical activity in 1979 dr noble expanded on this idea by explaining that it is usually the result of training error and developed a diagnostic assessment in which the clinician applies direct pressure to the lateral epicondyle and brings the knee from a flexed position to an extended position a positive test would recreate the patient's symptoms usually at about 30 degrees of knee flexion over the years a tight it band was thought to be one of the primary
drivers of this condition which was assessed with what is known as ober's test if your ober's test was positive then it was believed you had a tight i.t band that needed to be stretched to elongate it or foam rolled to break up scar tissue and release adhesions our understanding of the it band has improved since then for example papers by fair clawdal in 2006 and 2007 reported the perception of movement of the it band in a forward and backward direction over the lateral epicondyle of the femur is actually an illusion created by changing tension in
its various fibers during bending and straightening of the knee based on their anatomical investigations the it band is firmly attached to the femur so friction is not possible in 2016 will it at all found that ober's test doesn't assess tightness of the it band even if it did which it doesn't papers by fairclaw falvey and chaudry suggest that permanent deformation or elongation of the it band is unlikely therefore treatments shouldn't be aimed at trying to change its structure if friction isn't the culprit what is the current predominant hypothesis based on the work of orchard at
all in 1996 and fair cloud all in 2006 is that underlying adipose tissue or fat which can be highly sensitive is being compressed between 20 to 30 degrees of knee flexion during repetitive activities such as running but you also want to know why you have pain most people do and despite what you read or hear there's not always a simple clear-cut answer but there is a simple framework that we can apply based on a seminal paper by scott dye in 1996 he introduced the envelope of function which he described as a method of representing the
functional capacity of the knee and of other joints to accept transfer and dissipate loads let's use an example to illustrate what this means load is on the y-axis frequency is on the x-axis assuming you can train a few times per week you have a certain capacity to withstand various stressors on your knees without having an injury maybe you can jog three miles and squat 225 pounds if you take a few months off your capacity is going to decrease and your ability to withstand stressors is going to decrease if you train regularly over time your capacity
should increase and with it your ability to handle more stressors however if you have a spike in load or frequency that far exceeds your current capacity such as attempting to squat 400 pounds or jog 10 miles you might get injured and while it may not be to that extreme this is often the case with it band related pain you do a little too much a little too soon and push beyond your current capacity the good news is that the poison is also the antidote whether you're a runner cyclist or avid hiker the first thing you
want to do is reduce the intensity frequency and or volume of the aggravating activity to a tolerable level you might have to sacrifice some short-term training goals to achieve long-term success scale back but don't rest completely in the meantime you can incorporate other forms of cross-training to help maintain your fitness as well as the resistance exercises mentioned later if you're a runner it is often suggested to minimize downhill running trail running and running on uneven surfaces until you're able to run in a straight line on flat ground comfortably keep that in mind but you can
always test out what works for you although load management and activity modifications are the priority running retraining may play a small role for some individuals prospective research by nora nidol in 2007 found that female runners who developed it-band-related pain exhibited significantly greater hip adduction and knee internal rotation during the stance phase of gait a follow-up study by hamel at all in 2008 reported that the strain and strain rate of the it band and the involved limbs were greater than those of the uninvolved limbs and controls with strain rate being statistically significant another study by mir
dinodal in 2012 found that running with a narrow step width increases i t band strain and strain rate finally a study by boyer at all in 2015 reported that shortening your stride length leads to a wider step width and less hip adduction as well as decreases in both it bend strain and strain rate therefore a simple strategy to potentially decrease the load on your knee while running is to increase your cadence by five to ten percent which will shorten your stride length increase your step width decrease your hip adduction and decrease it band strain and
strain rate this can be done by using the features on your garmin watch or an app on your phone with regards to resistance exercises there's research by messier at all in 1995 frederickson at all in 2000 and freed it all in 2020 that found weakness of the hip and knee in individuals with it it-bend-related pain however there's other conflicting research so it's possible that the weakness is secondary to pain rather than the cause of symptoms for that reason the exercises will serve two primary purposes one train the joints muscles and movements most associated with running
to prepare you for its demands two improve the load tolerance of your knee in positions that are usually most aggravating for individuals with it band related pain i'm going to provide two exercise progressions per category so you have the option for variability based on comfort convenience preference etc exercise progression number one the first quadriceps focus movement is a split squat progression level one split squat isometric start in a stride stance and lower yourself straight down so that your back knee is hovering over an egg that you don't want to crack shorten the range of motion
or use your hands if it's too difficult aim for three sets of 60 seconds before progressing level two rearfoot elevated split squat isometric the overall technique of the movement and position of your torso should be similar so use an object to elevate your back foot that isn't too high the majority of your weight should be through the lead leg aim for 3 sets of 60 seconds level 3 deficit rearfoot elevated split squat you're going to elevate the front leg using a two to four inch object to start over time you can progress the height aim
for three to four sets of six to twelve slow and controlled repetitions add weight as needed the second option is a step up step down progression level one step up use a stair or object stacked six to seven inches high focus on putting all of your weight through the working leg and just gently tap up and down with your other heel if it's too difficult decrease the height or use your hands for assistance aim for 3 sets of 20 reps per leg level 2 lateral step down same exact cues except this movement will allow for
a little more knee travel aim for 3 sets of 20 reps per leg level 3 forward step down or elevated lateral step down you can either step forward off the step or continue to perform the lateral step down while gradually increasing the height of the step aim for three to four sets of eight to fifteen slow and controlled reps per leg exercise progression number two the first hamstrings focus movement is a slider progression level one feet elevated long lever bridge isometric with a slight bend in your knees about 30 degrees bridge up keep your glutes
squeezed and hold this position bend your knees more if it's too difficult aim for 3 sets of 30 seconds level 2 double leg eccentric slider bridge up keep your glute squeezed slowly slide your legs out drop down bring your feet back to the starting position and repeat if you can work up to 3 sets of 12 reps progress to the next level level 3 double leg slider aim for three sets of twelve reps level four single leg eccentric slider aim for three to four sets of four to eight repetitions the other option is to do
a nordic hamstring curl for three to four sets of four to eight reps exercise progression number three option one is a side plank progression level one short side plank start on your forearm and knees while keeping your trunk in a straight line hold this position level two side plank straighten your legs stack your feet and keep yourself in a straight line level three side plank hip abduction position yourself in the same way as the previous exercise but slowly move that top leg up and down with good control aim for three to four sets of 60
seconds as you work through each exercise option two is a band progression level one crab walk with a band around the knees the band can be placed above or below your knees depending on what's comfortable if the exercise is too difficult or painful use a lighter band no band or straighten your knees aim for three sets of 12 to 15 steps in each direction level two crab walk with the band around your ankles aim for three sets of 12 to 15 steps in each direction for levels one and two keep a slight bend in your
hips and knees your feet facing forward and lead with your knees minimize leaning with your trunk or bobbing up and down level three single leg fire hydrant isometric stand on one leg with the band around your knees spread the band by separating your knees and remain as still as possible aim for three to four sets of 45 second holds per leg you can also just increase the resistance of the band over time to progress any level exercise progression number four option 1 is a heel raise with knees straight and option 2 as a heel raise
with knees bent level 1 double limb heel raise on flat ground slowly rise up on the balls of your feet as high as you can and slowly lower yourself down aim for 3 sets of 25 repetitions level 2 single limb heel raise on flat ground aim for 3 sets of 15 slow and controlled repetitions level three single leg heel raise on a step aim for three to four sets of six to twelve repetitions add weight as needed in summary itban related pain is not a friction syndrome due to tightness of the it band that requires
vigorous rolling or stretching although the exact mechanism isn't fully understood it's thought that an error in workload such as a large spike in running mileage or intensity is a primary contributing factor therefore the focus of rehab should be on load management and activity modifications to find a tolerable level of your preferred activity while maintaining your fitness through other means if applicable you can trial an increase in your running cadence by five to ten percent to decrease your stride length increase your step width and decrease the strain and strain rate on your it band lastly you
can incorporate resistance exercises two days per week on days that you aren't running the focus should be on progressing them over the course of three to six months the exercises don't necessarily have to be pain-free but should be tolerable somewhere around a 2 out of 10 pain or less thank you so much for watching please if you enjoyed the video hit that like button subscribe turn on notifications and leave any questions or comments down below peace




![6 Exercises to Fix a Tight IT Band / ITB Syndrome Pain [for GOOD!]](https://img.youtube.com/vi/UnP2HFcr7FY/mqdefault.jpg)