hi this is Pam Johnson with today's resident presentation on gated chest CT pearls and pitfalls so when do we use a gated acquisition well the role of a gated acquisition is to minimize cardiac motion and gating can be performed retrospectively or prospectively because the motion artifact from the beating heart can cause all kinds of artifacts that mimic pathology and also limit the quality of the study particularly in coronary artery imaging in aortic valve evaluation we have to image with gating so that we maximize our temporal resolution and decrease the motion artifacts that limit image quality
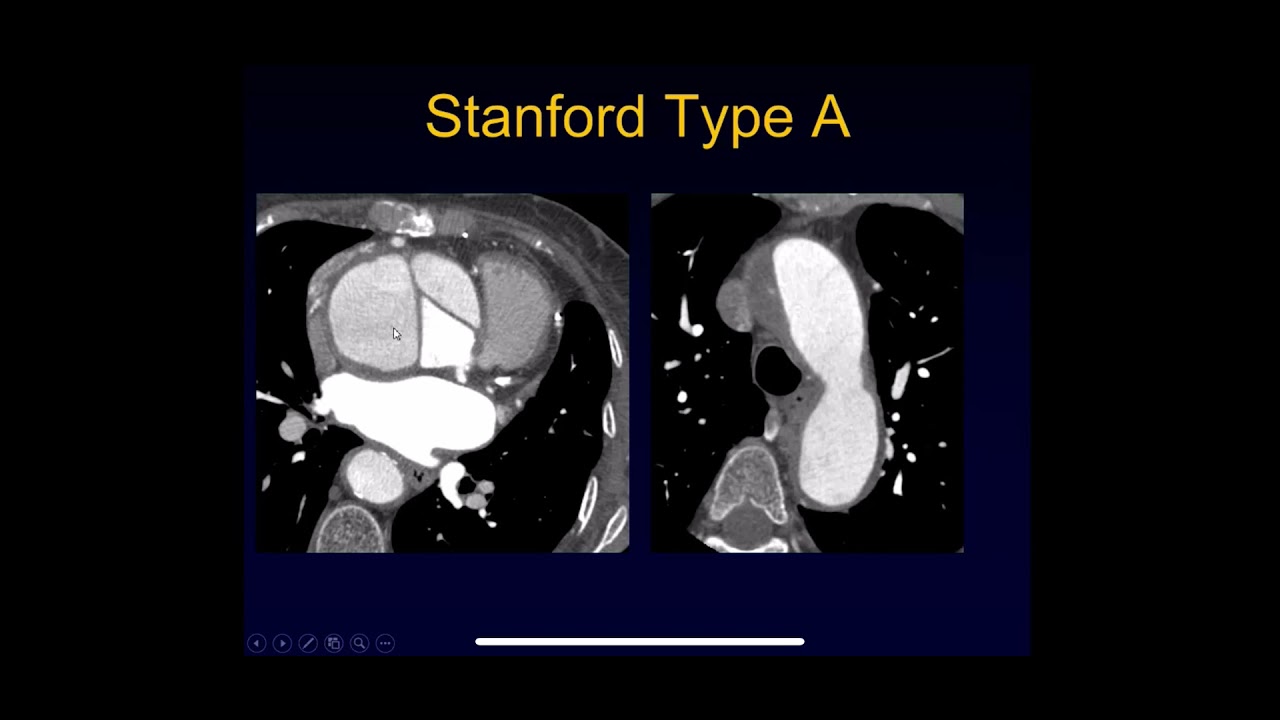
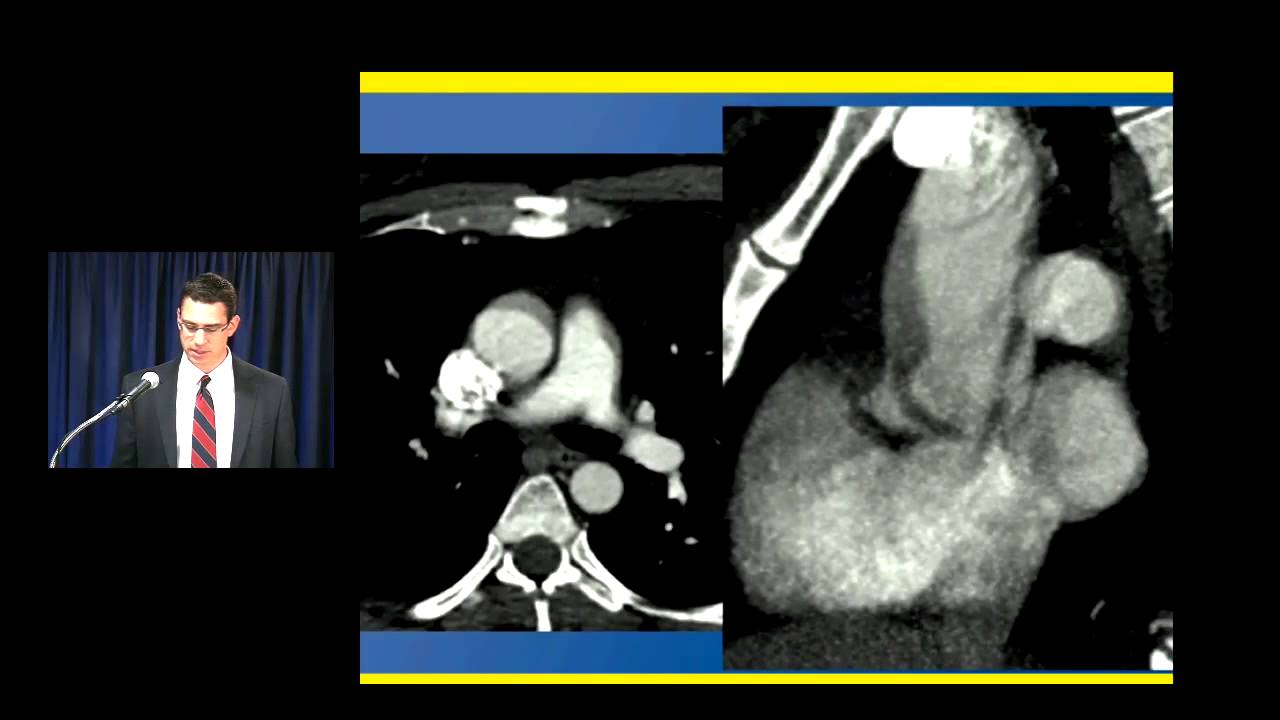
so let's look at this unguided study on a young woman who came in with chest pain and has what looks like a small dissection in the a semi thoracic aorta now we have all seen the pulsation artifact that looks like a dissection and in this case very well could be a pulsation artifact but she had a very strong clinical suspicion for dissection and we couldn't be absolutely sure that this wasn't a dissection so she was imaged the following day with a gated study look at the difference the case on the right there is no artifact
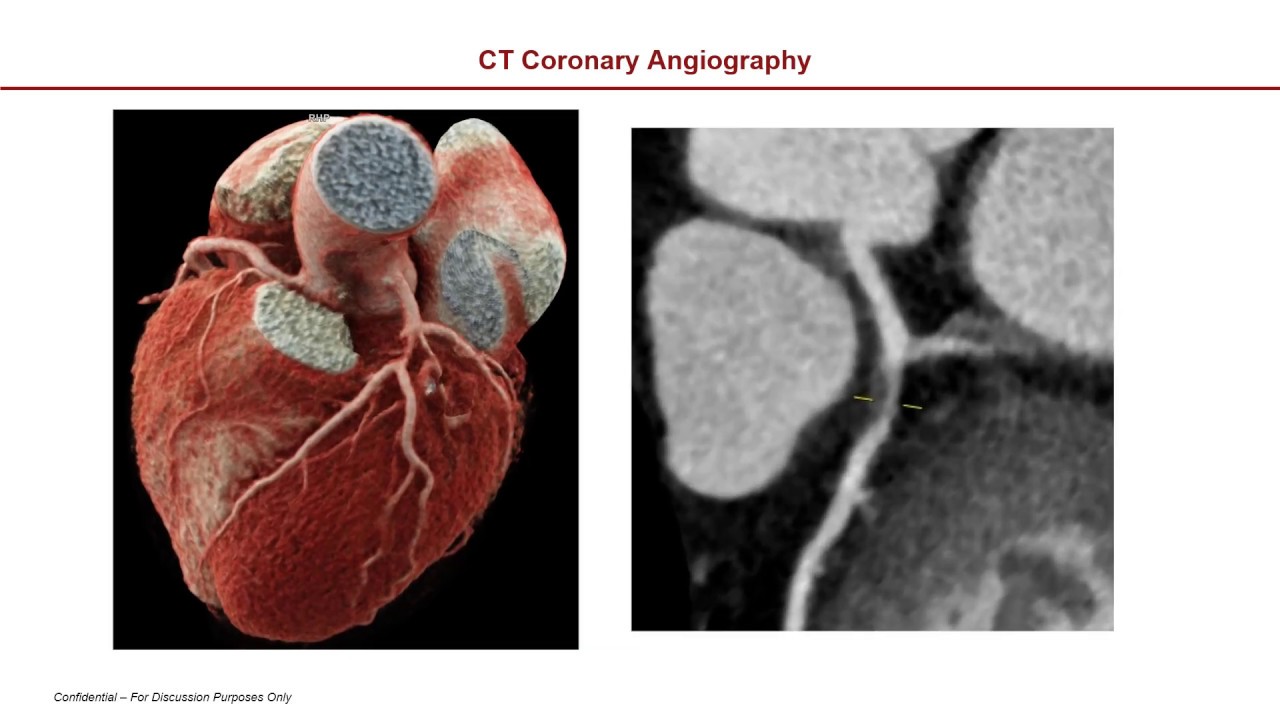
there is no dissection and there is no question so patient with chest pain and a concern for a sending thoracic dissection you have to perform a gated acquisition same patient every set of presentations axial sagittal coronal looked like there was a dissection on the first undated study and is clearly normal on the gated acquisition coronary artery imaging we need a gated acquisition so that we can evaluate these small vessels we're at a point in the cardiac cycle where the motion artifact is minimized here is a patient who had was being imaged actually for the ascending
aorta and we can see also has coronary artery disease many of these patients will have concomitant disease in the aorta and in the coronary arteries functional valve imaging requires retrospective cardiac gating and let's just take a quick review of the aortic valve there are three cusps during diastole the valve is closed and the cusps meet centrally which is called co-option and during systole the leaflets retract to create a triangular opening which is the aortic valve area with retrospective gating we image over multiple cardiac cycles and we can image the aortic valve over time and see
some a or tick function here's a nice example of a normal valve on the left during diastole the valve is closed the leaflets have completely co-opted on the right during systole the valve is open we can measure the aortic valve area as the valve becomes diseased the leaflets will not close completely during diastole resulting in a or Decor agitation and they won't open properly during systole resulting in the aortic stenosis so as we see in this case I have the normal valve on the top set of slides and then below this here is an abnormal
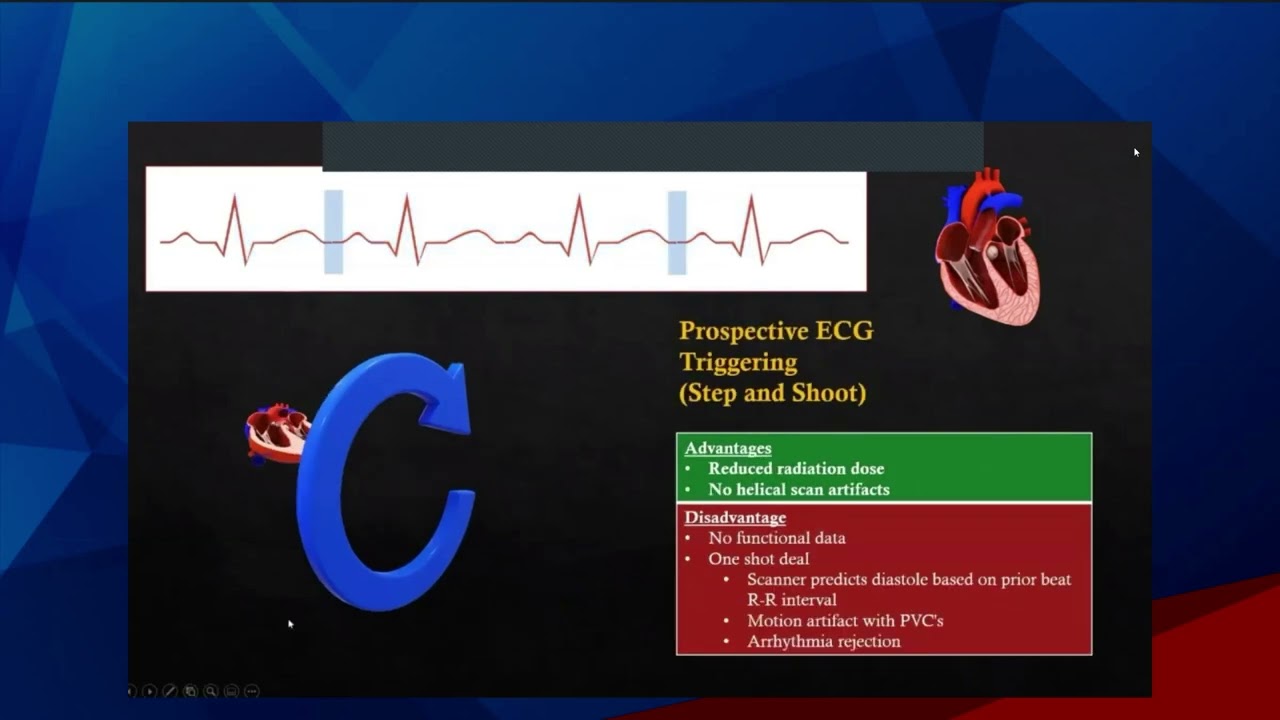
valve you can see that it is deformed with thickening of the cusps it's not opening completely and this is what a diseased valve looks like okay let's discuss the two different kinds of gating there's retrospective gating and prospective gating some scanners are not capable of prospective gating the advantage of prospective gating is that a much lower radiation doses administered the advantage of retrospective gating is that we image over time and we can perform functional analysis of the valve as I showed you in the last case even with retrospective gating we can limit the dose to
the patient by applying the maximum dose at a point in the RR cycle in the cardiac cycle that is optimal for imaging the heart and the coronary arteries so we begin with an EKG tracing of the patient we look at the heart rate we look at the RR interval we look at the cycle and the technologist will place what we call a pulsing window at the portion of the RR interval that is optimal for imaging the heart during the remainder of the cardiac cycle a much lower doses administered so in this way we can reduce
the dose somewhat although the dose from the retrospective study is still much higher than the dose from a prospective study with a prospective acquisition the radiation is only applied during the critical part of the cycle and during the remainder of the heart cycle there is no radiation administered at all at here's a paper that was published in radiology showing that there is a much lower dose administer with a prospective scan and yet there was no compromise in quality for coronary artery imaging all right so some of the pitfalls of gating and this is really something
that technologists need to understand and I think it's important that radiology who are interpreting this study should also understand that there are pitfalls that are primarily related to the patient's heart rate and these include applying the wrong pitch and applying the wrong pulsing window both related to the heart rate so the pitch is calculated according to the baseline heart rate however the heart rate may substantially change from baseline during inspiration and during contrast administration in this case the initially selected pitch is incorrect and this compromises image quality so what our technologists do is they watch
the heart rate over time we actually perform a test bolus to see if the patient's heart rate will go up during inspiration or during contrast administration and we do our best to select the optimal pitch based on what the heart rate we think the heart rate will be during the examination similarly the pulsing window that I described previously that's applied during the critical part of the RR cycle depends on the patient's heart rate so again we have to watch make sure the heart rate doesn't change over time and if the heart rate changes at the
time of the study then we're applying the pulsing window at the wrong portion of the RR cycle and we get a reduction in image quality so as I mentioned the text will monitor the heart rate during inspiration and during the test bolus administration so remember if you suspect a sending aortic dissection gating is essential and it's also critical for coronary artery imaging and for assessment of the valve that's all for now thanks and have a great day