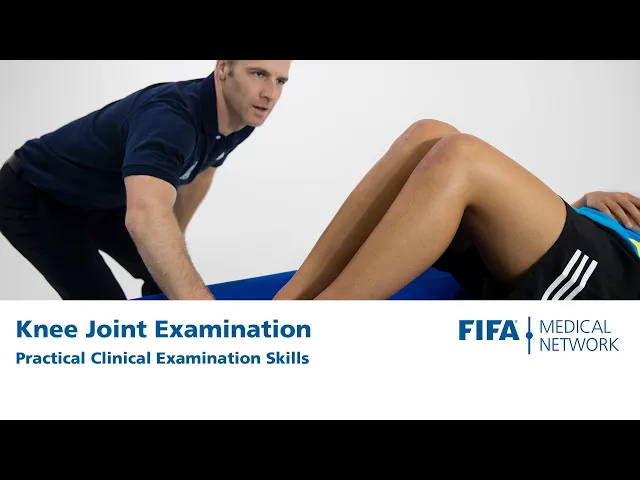
[Music] hi my name's mike fulcher and in this clip we're going to learn how to examine the knee so we've got martin with us martine if we get you to start by just doing some walking so we're looking at martin's gate looking to see if she has any problems walking and where there's any evidence of an intelligent gate and she's obviously walking fairly comfortably the next thing i like to do in standing is get the athlete to do a squat on one leg a single leg knee bend so if we get you on one leg
martin we're going to get you to squat up and down so the things i'm looking at from the front is is she able to keep her pelvis nice and level and is her knee heading inward so or is her knee able to stay nice and lined up over her foot which is desirable so martin's got good pelvic alignment there and her knee tracks nicely over her second toe be able to show us what what not so good looks like martin so knee dropping inwards pelvis wobbling around so it's a good functional test to assess how
the knee is moving in space so martin we might get you to hop up on the uh the end of the bed here and lie down lying on the bed here we're just it's a good opportunity to have a look at the knees have a look to see if there's any obvious swelling or scars or skin changes we can see that martine has an old surgical scale over her right knee here and i like to pick up her heels and see whether her knees will drop into normal extension where there's a block to extension or
any pain with that and you can see that they're both very symmetric there then we're going to examine martin's right knee here so i'm going to add extension and a bit of over pressure so when someone has joint disease often the knee doesn't move very well and it becomes painful or restricted towards the end of the range so that seems to be painless and extends normally i'm going to flex right up and see whether we can achieve full flexion where there's any pain or problems and we're having a look at martin's face to make sure
that she's feeling comfortable and then what i do in extension is have a look for an effusion so it's a little different to the look feel move that you may be used to but i think this is a good start to finish way to examine the knee so fusion we're doing a swipe test we swipe upwards pushing any fluid up into the suprapatellar pouch and then we swipe down on the outside looking for a bulge in the middle knee here so swiping up and then down the outside swiping down we can also palpate for an
effusion sometimes a larger effusion you don't have such a nice swipe so we can see is the knee feel full relative to the other side or we can do a patellar tap test when the knee is very swollen so we have a hand above the knee pushing fluid down into the knee proper pushing the patella see whether we can push it down tapping on the femur underneath so that's how to look for an effusion then i like to bend the knee up to 90 degrees comfortable in that position and so this is the best position
i think to palpate the major landmarks around the knee so i start at the medial femoral condyle so that's where the medial ligament attaches and where that that spot can be tender when someone injures the immediate ligament then i drop down onto the medial joint space and palpate the medial joint line so that's generally tender as soon as a minuscule tear or chondral defect in the medial compartment round onto the tibial tuberosity which is tender when an athlete has osgood schlatters disease palpate along the patellar tendon and around the inferior pole of the patella proximal
patellar tendon which is the site people have tenderness when they have patellar tendinopathy and then around the lateral knee joint line superior tib fib joint and we can also palpate around the patella and the quadriceps tendon so we've palpated fairly extensively there i then take the knee back into extension in an extended position the patella is more mobile and we can also palpate the patellar tendon a little bit better and we can elevate the inferior pole of the patella so we can palpate the deeper surface of the patellar tendon and athletes with patellar tendinopathy that's
often much more provocative than palpating the knee with the knee flexed so having done that i now assess the ligaments in the knee so first we're going to assess the collateral ligaments so with the medial ligament we apply a valgus stress so first with an an extension is there any laxity or pain then we take the knee into 30 degrees of flexion valgus force any pain or problems with that so that's rock solid similarly for the lateral ligament we're going to take the knee and extension and a virus force and then 30 degrees knee flexion
and a various force and so we can feel a good endpoint no pain or problems with those tests if there's laxity and extension we're thinking a much more significant injury than if there's laxity with 30 degrees knee flexion our next test is lockman's test that's a way to assess the anterior cruciate ligament so to do that we need to stabilize the thigh we need to make sure martin's nice and relaxed and we're trying to move the tibia anteriorly relative to the femur so we grab the tibia and we're pulling anteriorly and we can feel a
nice solid end point hopefully you can see that too if you've injured your acl then there's no firm end point that's very relaxed and it can be uncomfortable people with large thighs that can be quite hard to do to examine the knee so a useful technique is to use your thigh to support the femur so we want to explain what we're doing martin do you mind if i put my leg under your leg so we've got nice control over there the thighs sitting comfortably on my leg patient usually feels more comfortable with the knee flexed
a little bit and we do the same sort of movement if someone's injured their anterior cruciate ligament there's also another test called a pivot shift test which sometimes is pretty difficult to do when the athlete's knee is sore and is more easily done under anesthetic but it's still worth trying to do and basically the test tries to replicate the sensational feeling that the athlete has when they tear their acl so to do this test we take the heel put the leg into internal rotation apply a valgus stress and we take the knee from a position
of full extension up into flexion so internal tibial rotation valgus stress extension deflection and that should reproduce a clunking disconcerting feeling that is something like what the patient felt when they ruptured their acl the next ligament test we're going to do is a an anterior draw or posterior draw test so we bend the knee up to 90 degrees again we have to get the patient's permission i'm going to sit in your foot so we don't want to just jump on their foot because it gives them a fright so sit on your foot and what i'm
going to do is pull first anteriorly and then posteriorly so anteriorly solid end point no laxity there posterior drawer looking at the pcl very solid no laxity no pain if we think the patient may have a pcl injury we can do a different test looking for a posterior sag so we flex both knees up so they're sitting next to each other and we have a look at the tibial tubercles to see whether they're sitting at the same level if a patient's injured their pcl we may see one of the tibia sitting more posteriorly relative to
the normal or contralateral side having done that we're now going to move on to do some meniscal tests so the premise or basis for all these tests is can we capture the injured meniscus between a flex thigh and the tibia so any sort of test that has a degree of knee flexion and rotation can aggravate the meniscus so one test is to palpate the the joint line have your fingers on the medial and lateral joint line and to simply just tibial rotate the tibia so internal and external rotation and seeing whether that aggravates the patient's
pain mcmurray's test involves full flexion valgus and rotation or full flexion internal rotation and a virus force moving from flexion to extension so that's mcmurray's test the patellar femoral joint is also a common cause of knee pain so there are a few different things that can happen with the patellar femoral joint the first is patella patellofemoral dysfunction or patellofemoral pain and it's quite a difficult diagnosis sometimes because the pain is very vague and non-specific so a test where we compress the patellofemoral joint can be quite a useful thing so we basically apply a downwards or
a compressive force through the patella with our thumbs as we gently flex and extend the knee and we're seeing whether that reproduces any of the patient's pain or problems so is that a provocative thing does that reproduce something akin to your pain and the problem with that is it's often very sensitive and very provocative so we have to be sure that it's reproducing the patient's problem and it's also a different feeling to the other side so is that aggravating the patient's symptoms the other test that we can do is looking for patellar instability so the
patella apprehension test so when people dislocate their kneecap they dislocate laterally almost always so can we push the patella laterally as we're flexing and extending the knee the positive test is not so much pain it's more a sensation that something bad is going to happen so is the the knee feeling like it's going to dislocate having done that we're going to martine to roll onto her tummy into a prone position and lying prone we can inspect the popliteal fossa looking to see if there's any swelling so is there a baker cyst is there any obvious
asymmetry between the two and there are two tests that are worth considering in prone so the first one is the grind test the aptly grind test so it's a meniscal test we stabilize the femur apply an axial load through the heel and through the lower leg and we move the leg into external and internal rotation seeing whether it aggravates the patient's symptoms so these are very non-sensitive or low sensitivity tests the final test to have a look at is the dial test so this is a useful test if someone's had a more significant injury and
you think they may have injured the postal actual corner structures in the knee so we take both feet flex the knees to about 30 degrees and then externally rotate those feet so we're looking for any asymmetry and if there's an increase in external rotation of more than 10 degrees then you think that there may be an isolated posterolateral corner injury if you take the knees up to 90 degrees and there's an increase in laxity in this position we're thinking that there might be an isolated post retro corner injury and a posterior cruciate ligament injury so
that's quite a lot to get through but that's the approach i take to examining a footballer with an injured knee [Music]