the heart has four chambers two upper chambers the left and the right atrium or together the Atria and two lower Chambers the left and the right ventricles atrial flutter is used to describe when the Atria contract at really high rates about 300 beats per minute but sometimes as high as 400 beats per minute why flutter well there's a wave of muscle contraction that flows through the Atria that looks a little like it's flapping or FL in hence the name normally an electrical signal is sent out from the sinus node in the right atrium it then
propagates out through both atrias super fast causing the Atria to contract usually that signal Moves In One Direction from the Atria to the ventricles through the AV node it then moves down to the ventricles and causes them to contract shortly after after each ventricular contraction The ventricle has to wait for another signal from the sinus node with flutter a re-entrant rhythm starts in either the right or the left atrium re-entrant signals loop back on themselves overriding the sinus node and setting up an endless cycle that causes the Atria to contract again and again and again
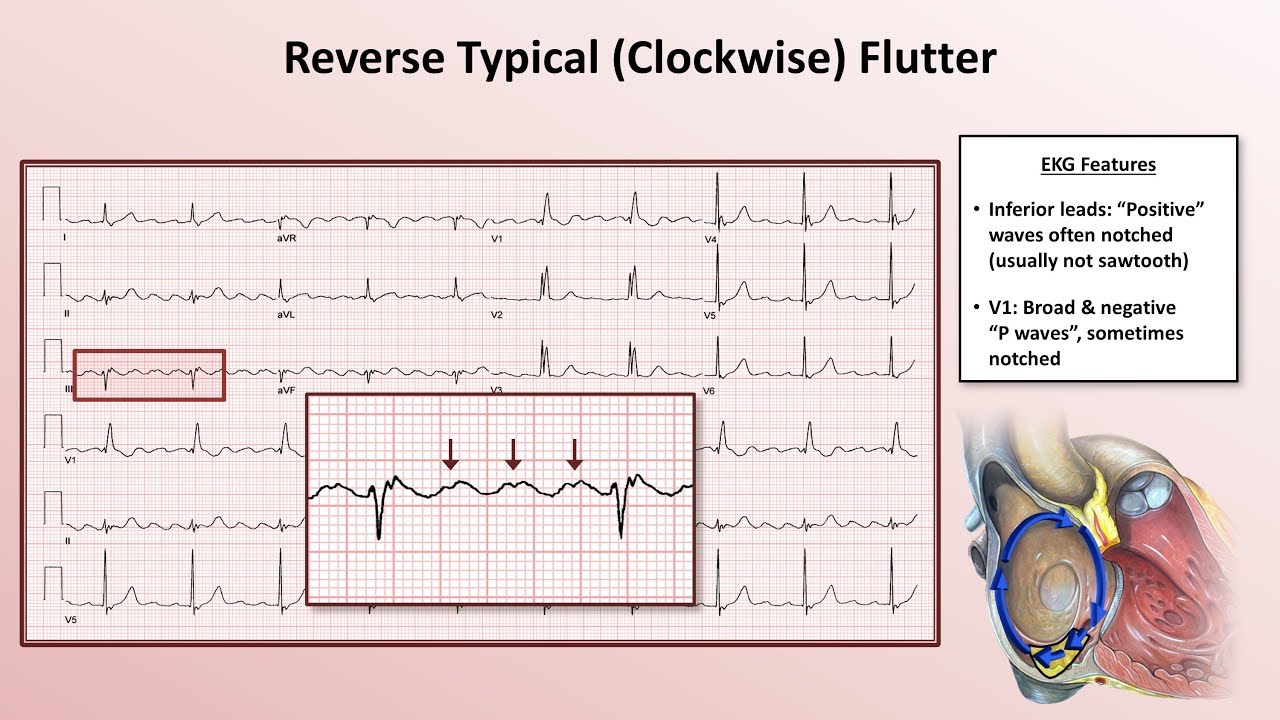
at really fast rates there are actually two types type one or typical atrial flutter is more common and is caused by a single re-entrance circuit that moves around the anulus or the Ring of the tricuspid valve of the right atrium usually in a counterclockwise Direction when viewed looking up through the tricuspid valve okay so imagine that you're this eyeball looking up through the valve you'll see the Superior vnea or SVC the inferior vena or IVC and the coronary sinus or CS in this case a stretch of tissue along the pathway called the Cavo tricuspid ismus
propagates the signal more slowly than the surrounding tissue tissue that was just activated can't be activated again until a certain amount of time is passed which is called the refractory period so that slow propagation through the ismos gives the tissue enough time to be out of refractory and therefore the circuit can loop back on itself type two or atypical atrial flutter is where a re-entered circuit develops in either the right or the left atrium but the exact location is less clearly defined again though we've got a similar setup where a wave of activated tissue or
depolarization hits a bit of tissue in such a way that it creates a loop of depolarization that keeps going around and around all right since everyone has a Cavo tricuspid ismiss but not everyone has atrial flutter there must be something else at play here that causes a re-entrance circuit in most cases there's some underlying disease like esea that makes the heart cells more irritable which can change some of their properties like the refractory period making it more likely re-entrance circuits develop in addition usually the circuit is initiated by a premature atrial contraction or PA P
AC which is an electrical impulse that's sent out early in the atrium before you'd normally expect one the exact cause of P's generally isn't known and they can even happen in otherwise healthy people so let's just say tissue a has a short refractory period and tissue B has a longer refractory period if a Pac is timed just right one tissue might depolarize and one might not and this can propagate an abnormal wave of depolarization which can go through the Atria and initiate a re-entry circuit in order for the ventricles to contract though that signal needs
to move down through the AV node luckily the AV node has a relatively long refractory period meaning it can't conduct every single impulse being sent from the Atria and typically maxes out around 180 beats per minute meaning it has to wait a minimum of about 1/3 of a second or 333 milliseconds until it can relay another signal so if the atrial rate's higher than 180 beats per minute you'll end up only getting a ratio of atrial beats to ventricular beats like 2: 1 or 3:1 in this case it might make a little more sense if
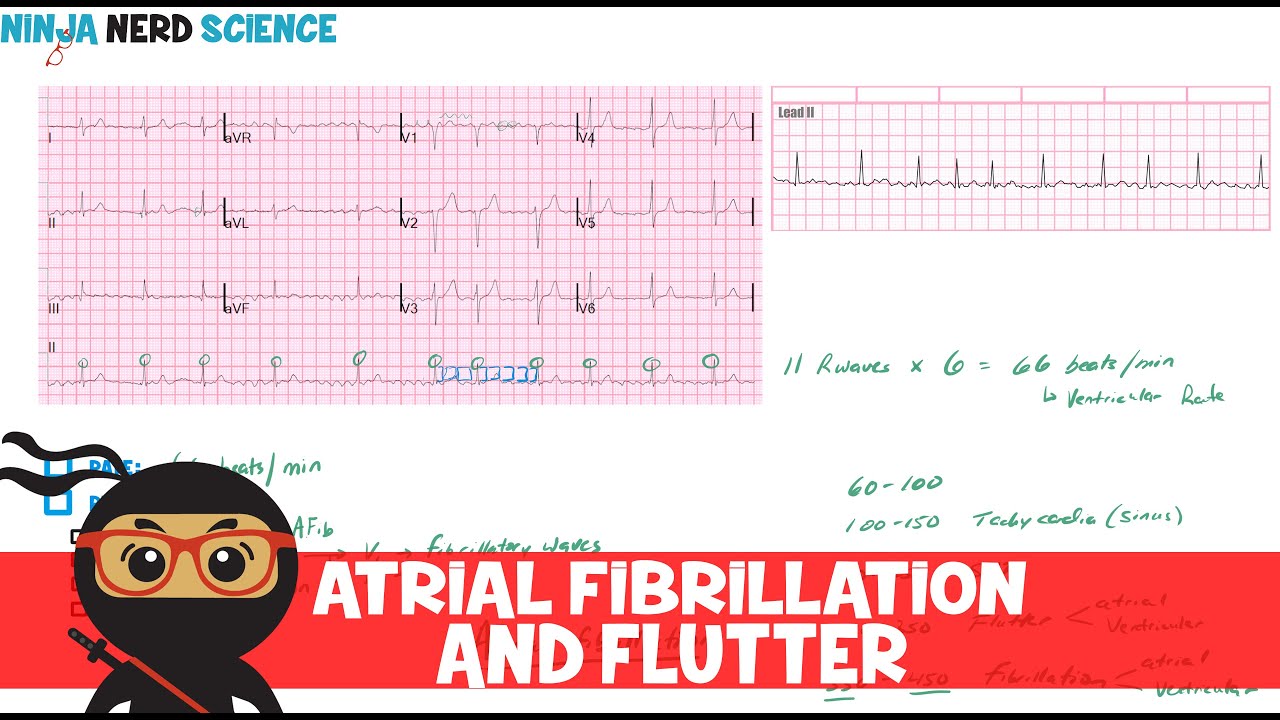
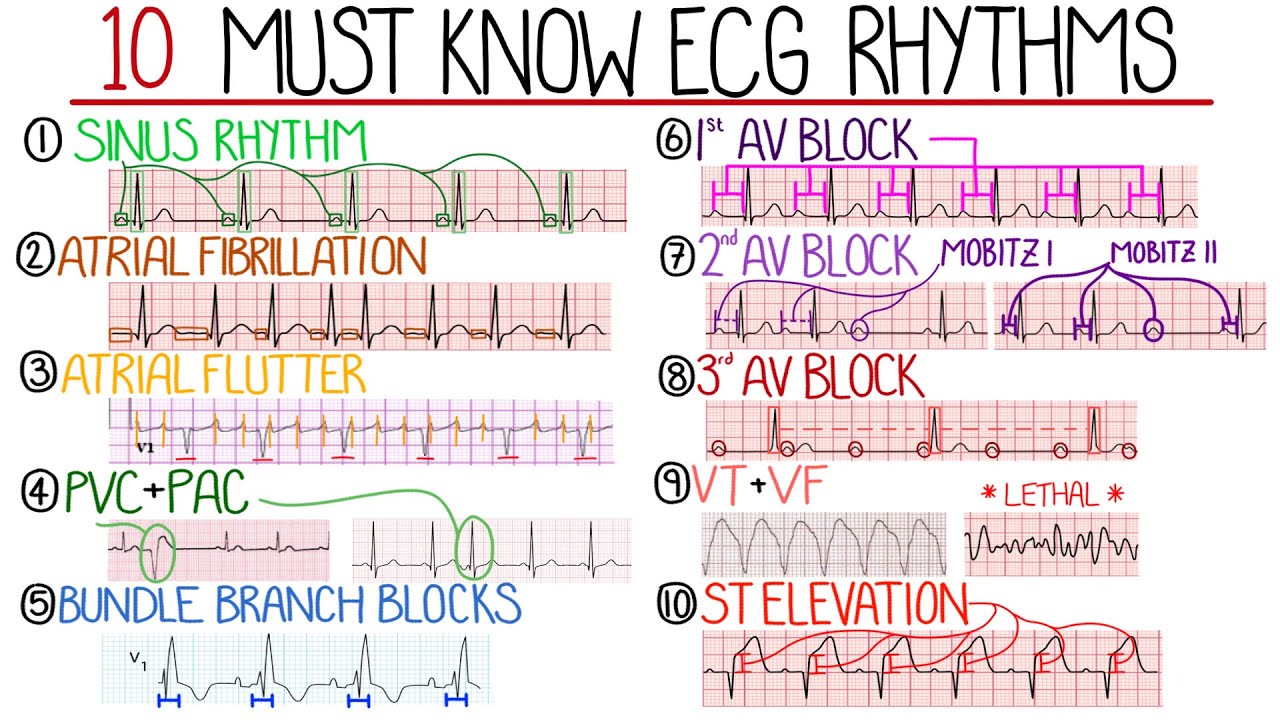
we look at an ECG now normally the depolarization wave originates in the SA node and produces what's called a p-wave the normal firing rate from the SA node is 60 to 100 beats per minute but in atrial flutter the electrical signals are coming from a re-entrance circle which moves much faster let's say 350 beats per minute in this case there are no normal p waves instead they're called flutter waves or f-waves and they take on this Sawtooth shape starting with this guy it goes to the ventricles and contracts the ventricles causing this QRS complex if
the cells in the AV node need to wait about 330 milliseconds the next atrial contraction which happens in about 170 milliseconds won't be able to conduct to the ventricles the next atrial event after that though lands at about 340 milliseconds from the first one which means that the AV node out of refractory and ready to go so it conducts this one in this example therefore we've got a 2:1 atrial to ventricular rate because for every two atrial contractions only one of them will lead to a ventricular contraction so in this example there were 350 atrial
beats per minute but only 175 ventricular beats per minute now let's say the atrial we're going at 400 beats per minute The First One conducts then it's 150 milliseconds to the next one then the next atrial beat after that would land at 300 milliseconds and the AV node still wouldn't be ready right meaning the ventricles wouldn't contract until the third atrial beat comes in at 450 milliseconds in this case it's a 3:1 atrial to ventricular rate 400 atrial beats per minute to 133 ventricular beats per minute because the ventricles are Contracting at a rate greater
than 100 beats per minute and because the source originates at above the ventricles this is considered a supr ventricular tacac cardia all right having higher ventricular rates like 133 or 175 beats per minute isn't usually life-threatening but if it's happening at rest it's generally not something most people want to experience if somebody has an underlying condition where they aren't able to physically tolerate High ventricular rates like this they might feel symptoms like shortness of breath chest pain dizziness and nausea over time from prolong episodes of tardia the ventricles can tire out and decompensate and people
can develop heart failure also since the Atria aren't Contracting very effectively blood tends to stagnate or pull in the atrium and this can lead to formation of blood clots that can embolize to the brain and cause a stroke usually because of the potential for embolism people with atrial flutter are given anti-coagulants or blood thinners to reduce the chance of clot formation they might also be given medications to control atates in the ventricles like beta blockers or calcium channel blockers alternatively an electrical cardio version can be performed to stop the episode of flutter these essentially depolarize
all the atrial tissue at once and let the sinus node take control again finally depending on the type of flutter type one versus type two patients might be good candidates for a radio frequency catheter oblation essentially the Cavo tricuspis is destroyed such that no signals can propagate through it and therefore no circuit can develop around the tricuspid valve all right as a quick recap atrial flutters when the Atria repeatedly contracts at really high rates usually due to an underlying condition combined with premature atrial contraction faster atrial contractions in turn increases the rate of ventricular contractions
which can cause shortness of breath chest pain dizziness and nausea in certain people over time atrial flutter can lead to heart failure blood clots and strokes helping current and future clinicians Focus learn retain and Thrive learn more