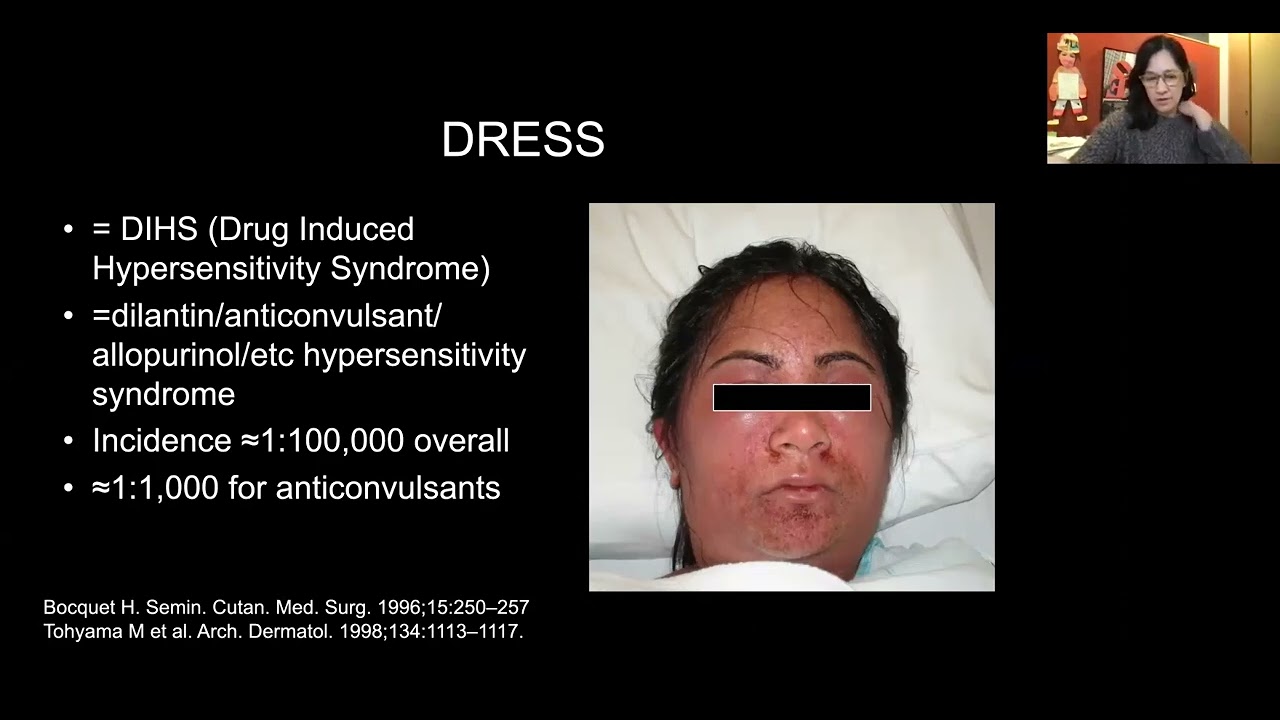
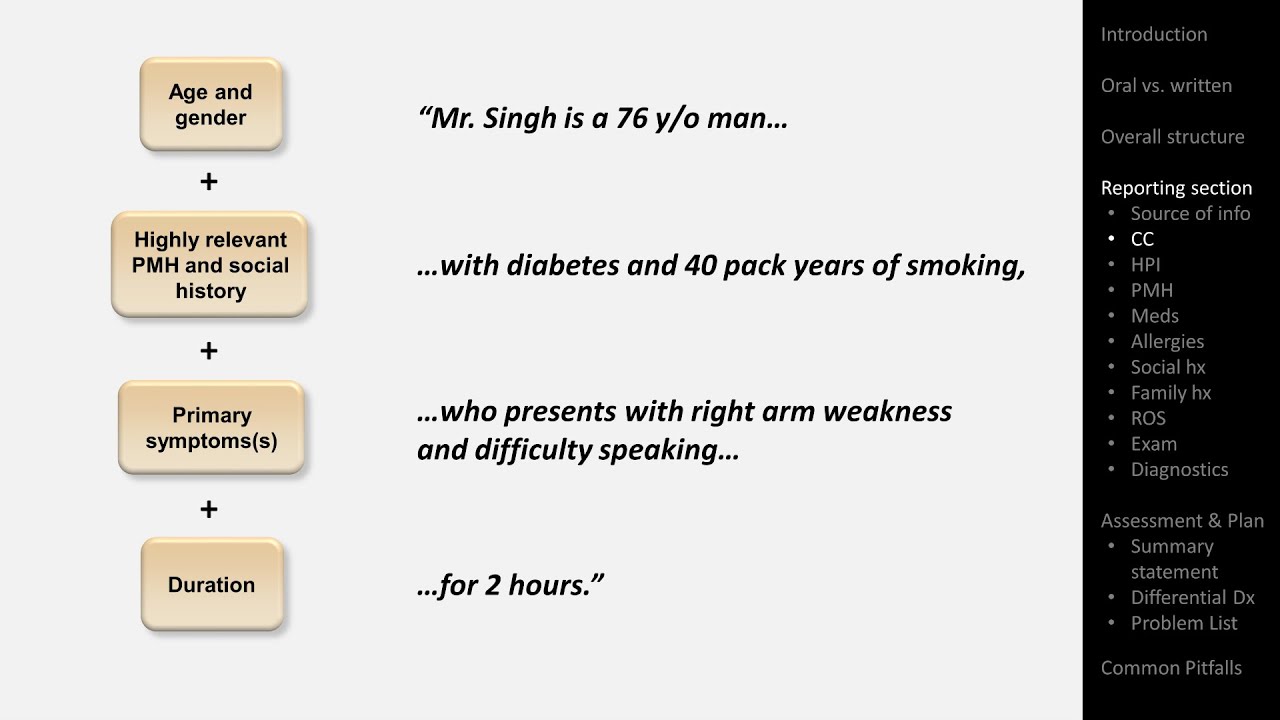
hello it's eric strong from strong medicine and today i'm discussing dress in brief dress is an acronym that stands for drug reaction with eosinophilia and systemic symptoms in short it's a severe potentially fatal drug reaction with prominent skin manifestations and which can cause multi-organ failure let's start with the clinical presentation the typical onset is two to six weeks after initiation of the causative medication with a mean delay of three weeks this is a bit longer than most serious adverse drug reactions the most readily apparent clinical manifestations are those of the skin which can take a
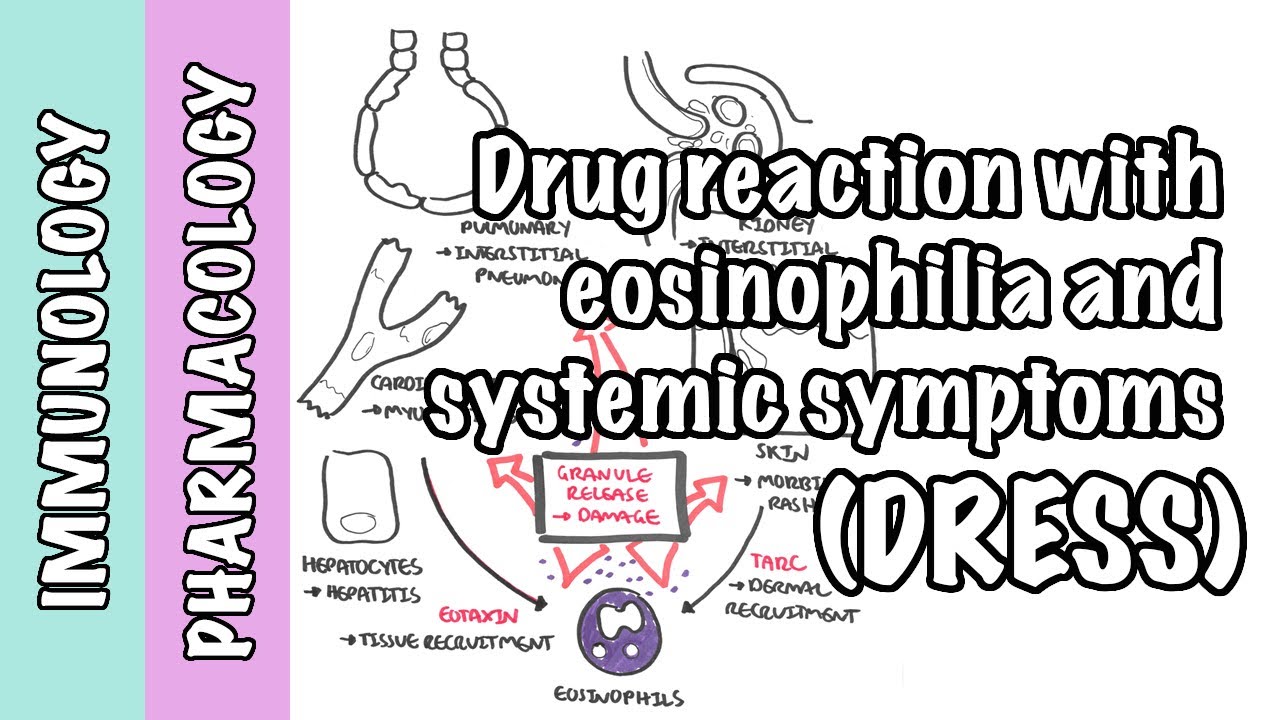
very wide variety of different appearances including a more biliform maculopapular rash the word mobiliform literally means a rash that looks like measles other possible skin manifestations include pustules and vesicles facial edema erythroderma which is a diffuse generalized inflammation of the skin and purpura among the systemic manifestations the most common and earliest to appear is fever which can be observed several days before the skin manifestations develop others include lymphadenopathy various hematological abnormalities including eosinophilia leukocytosis and the presence of atypical lymphocytes and most notably dress can cause organ dysfunction roughly in decreasing order of prevalence liver ranging
from modest lft elevation to acute hepatic failure kidneys including asymptomatic proteinuria interstitial nephritis and kidney failure lungs including pneumonitis and ards and the heart manifesting as a myocarditis the pathogenesis of dress is not well understood but it appears to be a t-cell-mediated hypersensitivity reaction dress has been strongly associated with the reactivation of viruses from the herpes verdier family particularly hh v6 however the specific nature of this association is unclear regarding which meds can trigger dress the most commonly implicated include allopurinol aromatic anti-convulsants which include phenytoin and carbamazepine among others sulfonamides including bactrim and sulfazalazine the
antibiotic vancomycin and the hiv medication navirepine other less commonly reported meds include beta-lactams nsaids dapzone omiprazole olanzipine and fluoxetine some data suggest that different drugs can lead to different clinical syndromes within the spectrum of dress for example the observation that dress caused by allopurinol is more likely to be life-threatening when it comes to making a diagnosis of dress there is no path in demonic test result or biopsy finding the diagnosis is a clinical one made by a combination of skin findings labs and a consistent medication history although several roughly similar sets of specific diagnostic criteria
for address have been proposed no one set of criteria has become the consensus standard as a representative of what these criteria look like here's just one of them for this criteria all three of the following features must be present in order to diagnose stress accutaneous drug eruption either eosinophilia or atypical lymphocytes and at least one manifestation of acute systemic disease among those that i mentioned earlier with the exception of fever due to the wide spectrum of cutaneous and systemic findings and the longer than average delay between drug initiation and symptom onset diagnosing dress is not
always straightforward and they can be mistaken for a number of other conditions these include other forms of cutaneous drug reactions including a common isolated morbidiform drug reaction which is a maculopapular rash predominantly on the trunk often colloquially referred to as a drug rash also on the differential diagnosis are the less common but far more serious conditions of stevens-johnson syndrome and toxic epidermal necrolysis the fever multi-organ dysfunction seen in dress can mimic sepsis the combination of rash fever and lymphadenopathy can mimic a variety of acute viral illnesses especially in children the cutaneous manifestations of dress can
sometimes look like cutaneous t-cell lymphoma including cesarean syndrome prominent eosinophilia can alternatively suggest one of the hyper eosinophilia syndromes and the combination of rash fever and multi-organ dysfunction can also be seen in lupus treatment options in dress are relatively few and none have been rigorously studied first for all patients the clinician must identify and immediately stop any potentially causative medication and should avoid any new meds if possible particularly those of a similar class or those with an established high risk of causing dress while the patient is recovering if the patient has mild to moderate cutaneous
manifestations with or without mild lft elevation and no other organ dysfunction topical steroids for symptomatic relief is typically all that's necessary beyond medication cessation for patients with severe cutaneous disease and or organ dysfunction systemic leukocorticoids such as oral prednisone or iv methylprednisolone are the first line if that's insufficient then cyclosporine and or ivig can be tried i'll end with prognosis the mortality rate from dress is a non-trivial five to ten percent the mechanism of death is most commonly reported to be liver and or cardiac failure among survivors full recovery takes an average of six weeks
from cessation of the causative medication during recovery relapses are common often triggered by the tapering of steroids and even after full recovery patients remain at an increased risk of recurrent dress including that triggered by meds which are structurally dissimilar to the original culprit they also have a higher risk of subsequently developing autoimmune disease whether these increased risks are because of a common genetic susceptibility to both autoimmune disease and dress in general such as hoa polymorphisms or whether they are the result of a permanent alteration to their immune system caused by the original address episode is
unclear that's it for this brief introduction to dress or drug reaction with eosinophilia and systemic symptoms if you found it interesting or helpful please consider subscribing to strong medicine and checking out other videos in this series on under-appreciated diseases