[Music] hello i'm eric strong from strong medicine in today's lesson on cardiovascular physiology i'll be discussing hemodynamics by the end of the video you'll be able to apply the equations of fluid mechanics to the cardiovascular system and list the limitations inherent in doing so to explain the bedside determination of central venous pressure by physical exam and to explain the relationship between mean arterial pressure central venous pressure cardiac output and systemic vascular resistance i want to start by defining hemodynamics in clinical usage the word human dynamics most often refers to parameters of a patient's physiology such
as systolic blood pressure and heart rate when on a medical or surgical unit and cardiac output and mean arterial pressure when in an icu or an operating room in the context of physiology though the word hemodynamics has a broader definition it is the application of the physical principles of fluid mechanics to the cardiovascular system because hemodynamics is fundamentally as much physics as it is physiology there will necessarily be some simple equations included in this video please do not let this intimidate you we are not going to be quantitatively solving problems but qualitatively discussing the equations
are necessary to understand how different physiologic parameters are related to one another i'm going to start with pressure from a physics perspective this is defined as the force applied perpendicularly to a surface per unit of surface area when we are specifically discussing pressure in hemodynamics we could be referring to arterial blood pressure which can be subdivided into systolic diastolic and mean arterial pressure something called the central venous pressure which i mentioned a second ago which is pressure in the distal superior and inferior vena cava which is used as a surrogate for right atrial pressure the
pulmonary artery pressure or something called the pulmonary capillary wedge pressure which is used as a surrogate for left atrial pressure the typical units for pressure in hemodynamics are millimeters of mercury or in the case of the physical examination of the jugular vein centimeters of water these unusual units both come from the potential use of these fluids in barometers for example a pressure of 760 millimeters of mercury is the pressure necessary to support a column of mercury 760 millimeters in height the units they're just a consequence of a quirk of history that we originally used mercury
barometers to measure pressure and now we're unfortunately stuck with them i want to focus for a moment on something called hydrostatic pressure there are a few different ways in which hydrostatic pressure can be defined but in the following context i will define it as the pressure present in a fluid at rest due to gravity the hydrostatic pressure often written as a difference in pressure between two points at different depths is equal to the density of the fluid times little g that is the acceleration to earth due to gravity times the difference in heights between the
two points what's interesting about this equation is that the shape and orientation of the vessels or containers which hold the fluid are irrelevant for determining the pressure to see what i mean by this imagine that you hypothetically own two jellyfish each in its own tank in tank a there is a huge reservoir up top and a small chamber at the bottom whereas in tank b there is a huge reservoir at the bottom and a small diagonal column of water extending upwards if the total depth of the water is the same in both tanks when the
two jellyfish are at the bottoms of their respective tanks they experience equivalent pressures the shape of the tanks and whether a column is straight up and down or oriented at an angle it doesn't matter which feels counterintuitive to many people so how do jellyfish relate to cardiovascular physiology one prominent application of the concept of hydrostatic pressure is in the bedside determination of a patient's central venous pressure since the jugular vein is directly connected to the right atrium via the superior vena cava and the jugular vein is a highly compliant vessel meaning that it readily dilates
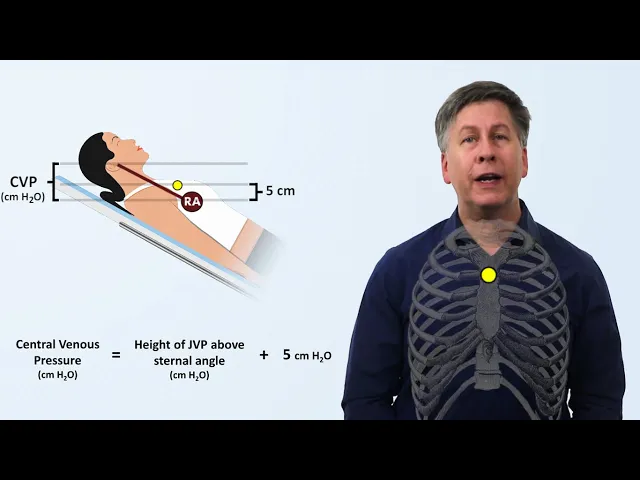
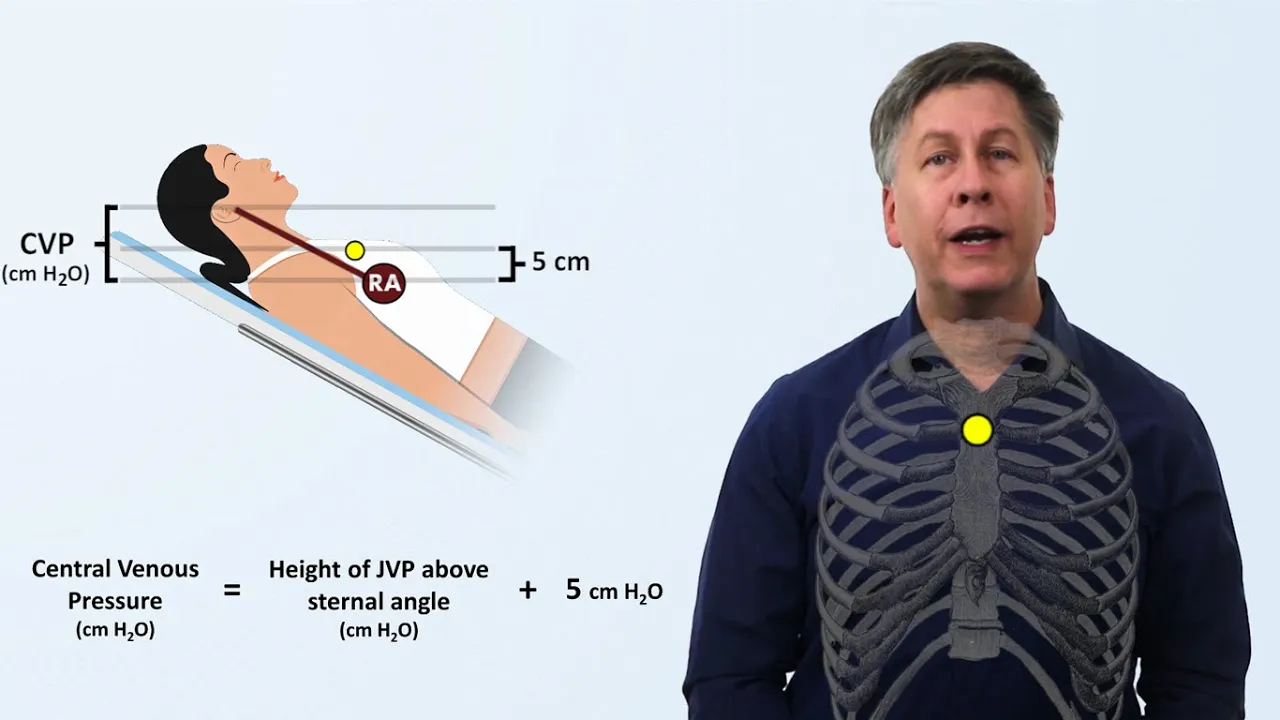
when filled with blood but collapses when it's empty we can estimate the right atrial pressure by examining how high the jugular veins distension extends in other words we use the internal jugular vein as a blood-filled barometer for example suppose a patient is fully upright at 90 degrees and the jugular venous pressure extends to this level we can say that the central venous pressure is equal to the density of blood times little g times the vertical distance between that level and the level of the right atrium and the simplified units we use units of centimeters of
water using the fact that the density of water and blood are approximately the same but how do we know where the right atrium is clinicians make an assumption based on an old observation that the right atrium tends to sit approximately five centimeters closer to the earth than a palpable external landmark called the sternal angle which is the subtle bony prominence in the center of the chest where the manubrium joins the body of the sternum so one can therefore determine the central venous pressure in units of centimeters of water as the sum of the height of
the jvp above the sternal angle and five centimeters in those patients who are unable to sit fully upright or if the jvp is not visible when a patient is fully upright the method stays the same it doesn't matter what angle the patient is at all that matters is the vertical distance to which the jugular veins distension extends though this requires the assumption that the right atrium will still be five centimeters closer to earth than the sternal angle irrespective of what inclination the patient is at however in practice there are limitations to precisely measuring cvp with
this technique two physical exam limitations one needs to be able to distinguish venous from arterial pulsations and in patients of large body habitus the jugular vein may simply not be visible at all there are also physiologic limitations measuring hydrostatic pressure by definition requires the fluid to be stationary which of course is not true of blood in the jugular vein as we can see the jvp oscillates with one period synchronized with the cardiac cycle and another synchronized with a respiratory cycle in the cath lab where there's a catheter that is directly transducing the pressure in the
right atrium the cvp is measured at end expiration but in 20 years as a physician i have yet to see a clinician at the bedside time there's jvp measurement to the respiratory cycle even the sacrosanct five centimeters that's added to the jvp is an oversimplification first the assumption that the right atrium is always five centimeters below the sternal angle irrespective of inclination of the patient's body and irrespective of the size of the patient is just not true the original description of this method in a 1946 paper is illuminating the authors openly adopted the five centimeter
number for simplicity and acknowledge the uncertainties and potential sources of error which many modern physical exam references seem to have forgotten so conceptually this is a valid technique to estimate the cvp as long as one realizes there is a significant range of error i'll move on to flow often abbreviated as q flow is the volume of fluid that moves past a certain point per unit time we can represent that mathematically as q equals v for volume over time when applied to hemodynamics the obvious example of flow is cardiac output flow in hemodynamics whether we are
talking about cardiac output or flow to a specific organ or vascular bed is given in either milliliters per minute or liters per minute imagine we have a tube or a pipe of variable width capable of conducting a fluid the fluid flow at point 1 must necessarily be equal to the flow at point 2. likewise if that tube were to separate into two separate branches the flow at point one the parent tube must necessarily be equal to the sum of the flows through the two branches let's go back to the single tube of varying diameter and
take a look at two arbitrary segments each of which consists of a cross sectional area and a length flow is defined as the change in volume over change in time the volume of a cylinder is area times length but we can regroup length with time which is equivalent to velocity so in other words the flow through segment one is equal to the segment's cross-sectional area times the velocity of fluid as it passes through segment one we can do the exact same thing for segment two and since we know the two flows must be equivalent we
know that the product of the cross-sectional area and velocity at one location of the tube or conduit must be equal to the product of the cross-sectional area and velocity in the other segment this is known as a continuity equation one common demonstration of the continuity equation can be seen with the flow of streams and rivers a river will move slowly when it's wide and deep while speeding up significantly when funneled into a narrow canyon the same phenomenon happens within the cardiovascular system for example we can apply the continuity equation to understanding the relative velocities of
blood flow at different points during the circulation let's first look at vessel diameter when blood initially leaves the heart there is only one conduit the aorta which is between two and three centimeters in diameter then as arteries branch off from the aorta the vasculature divides and divides again into ever smaller arteries becoming arterioles and eventually becoming capillaries capillaries are incredibly small typically under 10 micrometers in size and after a very short distance capillaries merge to become venials which then merge to become veins and then bigger veins and eventually the superior and inferior vena cava which
are each almost as big as the aorta then we can consider the total cross-sectional area at each stage along the path of circulation in other words the average vessel cross-sectional area times the number of vessels for a certain level of blood vessel with the aorta there's only one so the total cross-sectional area is just calculated as pi r squared but as one moves through the circulation to the arteries and then arterioles and then capillaries the number of individual vessels increases faster than the cross-sectional area of each vessel decreases this means that the total cross-sectional area
is extremely high for the capillaries finally we can apply the continuity equation and see that as we move from the aorta down to the capillaries the mean velocity of blood traveling through those vessels decreases until it reaches a minimum in the capillaries which provides the red blood cells more time to exchange oxygen carbon dioxide across the capillary membrane resistance is impediment to flow of fluid through a conduit when applied to hemodynamics this is obviously referring to blood flow through a single vessel a group of vessels up to and including the entire systemic vasculature or flow
through a heart valve typical units for resistance are relatively less familiar to clinicians resistance is given in either dines seconds per centimeter to the fifth or units of millimeters of mercury minutes per liter the ladder of which is also known as either hybrid resistance units or wood units named after the cardiologist paul wood to see what factors play a role in determining resistance to flow let's take a tube of radius r and length l there's a relationship sometimes called posier's law but which is more accurately a corollary of possies law that allows for the calculation
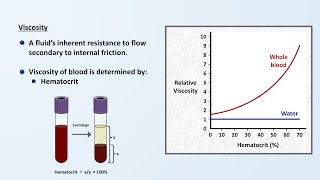
of the resistance of a tube as a function of its length radius and something called viscosity which describes the thickness of a fluid for physiology this specific equation is not as important to remember in its entirety but the simplified version is resistance in a tube is proportional to the viscosity of the fluid and inversely proportional to the fourth power of the tube's radius that fourth power relationship is huge by decreasing the radius of a blood vessel by 50 resistance is increased 16 fold and by decreasing the radius by 75 percent the resistance increases 250 times
although physiology textbooks will often refer to possibilities law when discussing resistance within blood vessels there are some huge limitations to strictly applying it to hemodynamics it requires flow to be constant the conduit for flow to be rigid in other words the walls have no elasticity to them the fluid must have a constant viscosity and the fluid flow must lack turbulence unfortunately none of these requirements are met within the cardiovascular system blood flow from the heart is pulsatile not constant our blood vessels are not rigid the viscosity of blood is actually not constant as i'll discuss
more in the next video in the series and there are places in the circulation that do have turbulence so do not apply this equation quantitatively in physiology it's enough to know that higher viscosity increases resistance and that the radius of the vessel has a very dramatic impact on resistance there are a few other points to make about resistance here if we graph pressure along the circulation path we can note a few things first the pulsatile nature of blood flow gets attenuated as the vessels become smaller resulting in flow being smooth by the time it reaches
the smaller arterials and vessels distal to them but also there is a steep drop off in the pressure as blood passes through the arterials this means that the arterials are the site of the greatest resistance to blood flow this is an important component of both the systemic and local regulation of blood flow arterials have muscular walls that can constrict or dilate to significantly alter vascular resistance to specific capillary beds in response to a variety of local and systemic signals another aspect of resistance relevant to hemodynamics is the concept of resistors and their arrangements within a
more complex system to understand what i'm talking about we're going to take the first of two brief detours into electric circuits which provides analogies to fluid mechanics you may recall circuit diagrams from either high school physics or a medical or nursing school entrance exam like the mcat straight lines represent wires which in the simplest representation are assumed to have no resistance at all and there are discrete segments known as resistors represented in the diagram as a zigzag flowing through the wire and resistor is current denoted by the letter i when we have multiple resistors within
a circuit the total net resistance of the circuit depends not only on the magnitude of the resistance within each individual resistor but also on how these resistors are arranged for example resistors can be placed along the same branch of wire one after another which is referred to as resistors in series in this case the total resistance is equal to the resistance of each individual resistor added together alternatively resistors can be arranged in parallel branches in this case the total resistance can be calculated as follows the reciprocal of the total resistance equals the reciprocal of the
resistance from each individual resistor add it up together both of these formulas apply whether a circuit has only two resistors a dozen resistors or thousands of resistors when we consider how this might apply to human dynamics there are certainly examples of resistors in series within the body but the more obvious example is the consideration of arterioles as many resistors in parallel for example in an extremely simplified model we can think about the set of arterials supplying each organ as acting as one resistor just as the amount of current that each branch of a circuit would
receive is related to the resistance within that branch the blood flow to each organ is most affected by the resistance to flow specifically to that organ if through selective vasodilation the resistance to an organ were to dramatically decrease the blood flow to that organ dramatically increases this can be due to hormones or signals from the nervous system or it can be due to inflammatory mediators you'll think about how an infected part of the body can become red hot and swollen selective vasodilation can also occur in response to an accumulation of metabolic byproducts like carbon dioxide
and lactate that could be seen in exercising skeletal muscle on the other hand selective vasoconstriction can also occur or something like focal atherosclerosis or an acute arterial blood clot in which the resistance to a specific organ were to dramatically increase this would dramatically decrease the amount of blood flowing to that organ although this increases the net resistance to the entire cardiovascular system because there are so many other possible paths for blood to take the increase in net resistance is usually negligible whatever blood would have normally gone to that one organ gets redirected to all the
others and the impact on the functioning of the heart itself is usually negligible one very notable exception to this are large pulmonary embolisms which are blood clots that form in these systemic veins and then break off and travel via the venous system through the right side of the heart and become lodged somewhere in the pulmonary arterial tree these clots can be large enough and numerous enough to reduce the total cross-sectional area of the pulmonary vasculature to the point that a clinically relevant increase occurs in the resistance to blood flow out of the right side of
the heart the ability of the body to selectively regulate blood flow to different organs is a critical component of human dynamics while a healthy heart can increase cardiac output four to five times in response to exercise or illness the increased metabolic demands of individual organs can temporarily increase much more than this this increased metabolic demand cannot be met only by increasing cardiac output there also needs to be a way to redirect blood away from the organs which have reduced need at that particular moment the body changes the resistance to individual vascular territories in addition to
this being done to meet metabolic needs it also plays a role in temperature regulation for example how vessels which normally perfuse the skin vasoconstrict in cold weather before we move on there is just one more very brief term to mention the conductance of a vessel is defined as one over the resistance there are situations in which either talking about conductance is more intuitive or using conductance in equations is quantitatively easier by this point we've discussed some basic concepts behind pressure flow and resistance now i'm going to show you how these three general physiologic parameters are
related in the most important equation in cardiovascular physiology but to do this i'm going to employ the second analogy with circuits imagine the simplest possible electrical circuit we have a single battery represented by a set of alternating parallel lines across which there is some electric voltage we have a single resistor and we have current moving through the circuit and resistor from the positive terminal to the negative terminal of the battery and let's suppose we are told that the battery is a 12 volt battery and the resistor is a 4 ohm resistor an ohm is just
a measure of electrical resistance and we are asked to calculate the current to do this we can use one of the most commonly taught and used equations in the field of electricity and magnetism ohm's law ohm's law states that the voltage equals the current times the resistance a relationship abbreviated as v equals ir so in this case if we were tasked to quantitatively determine the current we would plug in 12 volts and 4 ohms into the equation and determine that 3 amps of current are running through the circuit and we could add a layer of
complexity by changing the one resistor to several in parallel each with a different resistance but after calculating the total resistance present ohm's law would still apply and as you might remember from high school physics not only does ohm's law apply to the entire circuit it also applies to each individual resistor so if we knew the specific resistance in each of these resistors we could calculate the current through each one separately if we took the current through each individual resistor in parallel and added them together it would equal the current running through the entire circuit just
like fluid flow through one tube must necessarily equal the sum of fluid flow through separate branches of that tube to continue the comparison with fluids we can replace our battery with a fluid pump with a heart the wires become tubes or blood vessels and the parallel resistors become the vascular beds to individual organs our ohm's law for fluids then becomes the change in pressure equals the flow times resistance and substituting in values from physiology we have the mean arterial pressure minus the central venous pressure equals the cardiac output times systemic vascular resistance the last of
which is sometimes called either the total vascular resistance or total peripheral resistance this is in my opinion the most important equation in cardiovascular physiology and in particular in the bedside practice of cardiovascular medicine however as there was with possies law there are limiting factors to applying this equation quantitatively first while map and cvp can be directly measured with a pressure transducer with high degree of accuracy accurate assessment of the cardiac output is not quite as easy and we have no practical method for either measuring or calculating systemic vascular resistance aside from this equation second as
mentioned before the presence of turbulence influences resistance as does elasticity of large arteries and the fact that flow is pulsatile rather than constant so in other words the resistance is not constant from one moment to the next last some physiologists have suggested that using cvp as the downstream pressure in this equation is overly simplistic and a higher value known as the critical closing pressure the pressure at which arterioles literally collapse shut is what should be used instead but the bottom line although it's common to employ this equation quantitatively at the bedside to track changes in
svr in critically ill patients it is important to not be overly reliant on this one calculation when making clinical decisions in life-threatening situations when i refer to it as the most important equation in cardiovascular physiology i mean that in a qualitative sense as it allows for an understanding of the relationship between four key physiologic parameters there exists an equivalent equation for the pulmonary circulation in which the mean pulmonary artery pressure minus the pulmonary capillary wedge pressure equals the cardiac output times the pulmonary vascular resistance in summary when it comes to human dynamics there are four
equations to remember the definition of flow the continuity equation the corollary deposits law showing the relationship between resistance viscosity and the radius of the vessel and the hemodynamics version of ohm's law for fluids some other takeaway points central venous pressure can be estimated from the physical exam using the concept of hydrostatic pressure the level of blood vessel that has the greatest total cross-sectional area and thus the location of the lowest blood velocity is the capillaries the radius of a blood vessel has a very dramatic impact on the degree of resistance the body can regulate blood
flow to specific vascular territories by selectively changing the radius of certain arterials and last the classic equations of human dynamics presented in standard medical textbooks and in this video are only approximations due to pulsatile flow the presence of turbulence the inherent elasticity of blood vessels and the non-constant viscosity of blood that concludes this video on hemodynamics if you found it interesting and helpful please remember to like and share it and consider subscribing to strong medicine for the rest of this ongoing series on cardiovascular physiology as well as a diverse collection of other medical topics [Music]