Bronchiolitis, by Dr Amanda Growdon. Learning Objectives. By the end of this video, the learner will have an understanding of the epidemiology and pathophysiology of bronchiolitis, its clinical presentation, and how to diagnose and care for affected children.
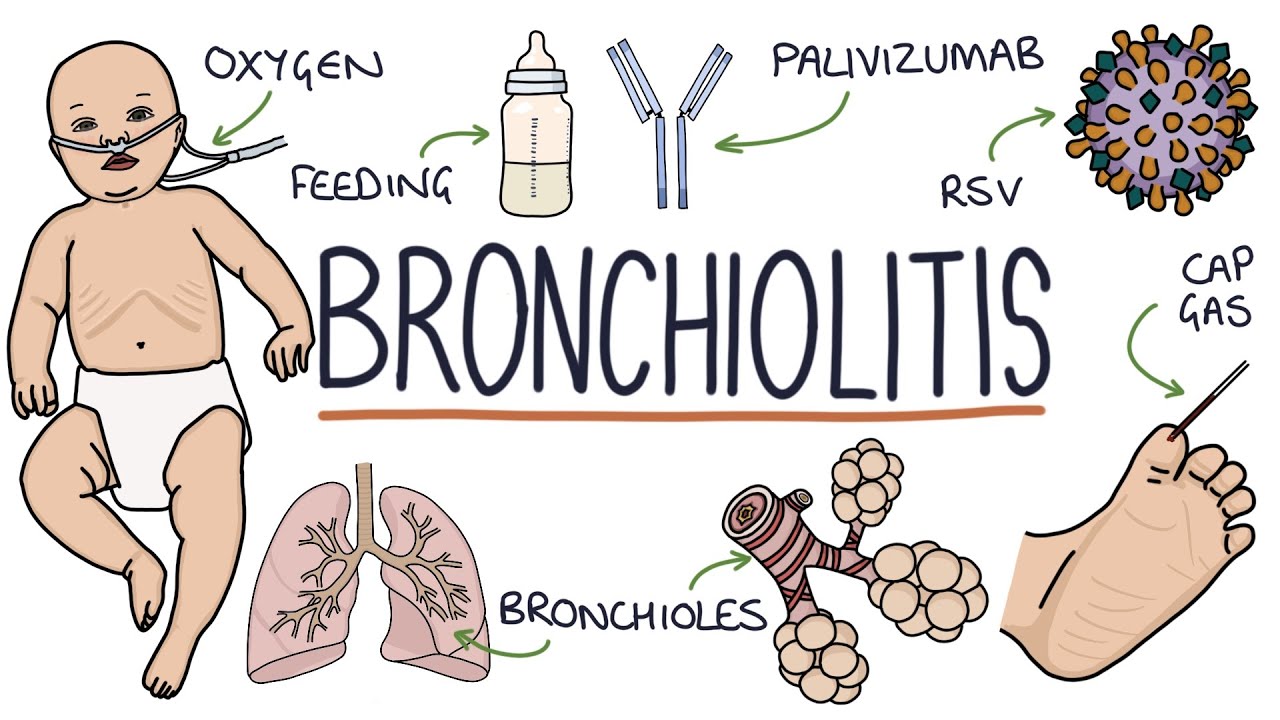
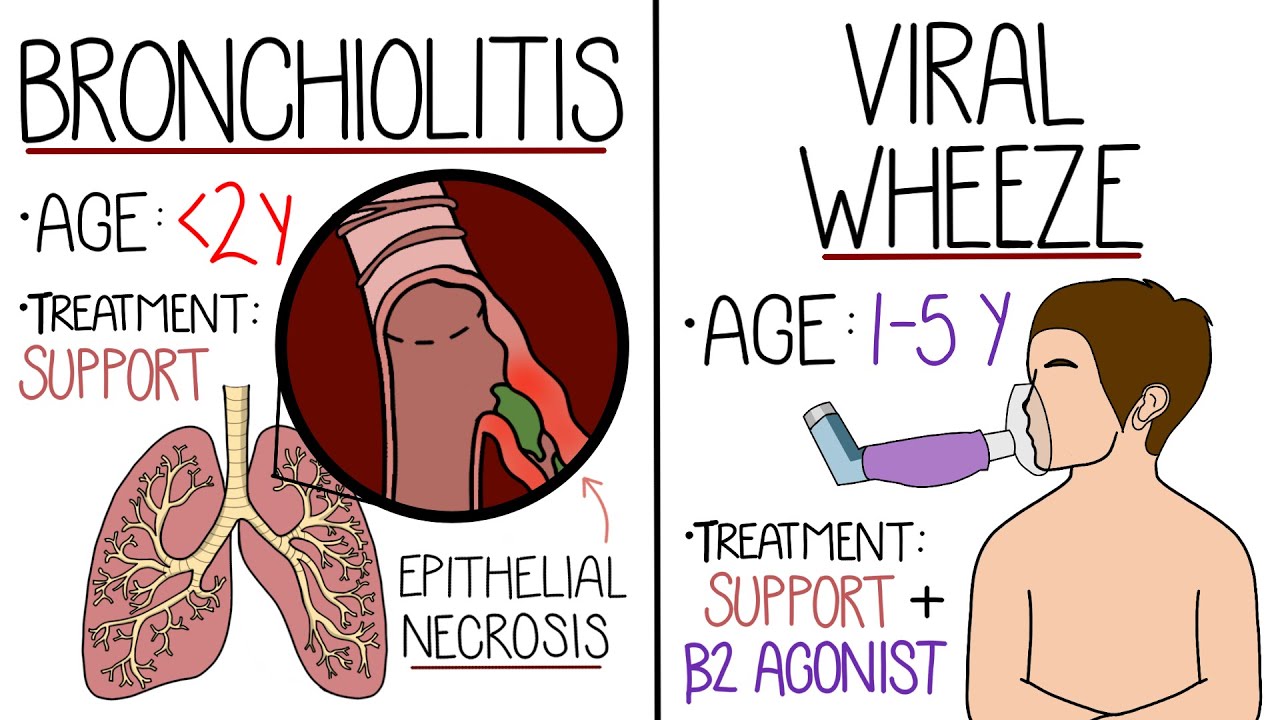
Introduction. Bronchiolitis is a viral lower respiratory tract infection affecting infants and young children, particularly in the winter months. It is a remarkably common infection in children less than two years old, with up to 20% of each year's birth cohort seeking medical attention for symptoms related to respiratory syncytial virus, also known as RSV.
While most children are managed as outpatients, between 2% to 3% of all infants are hospitalized for RSV, at an annual national cost of greater than $500 million. Though deaths related to bronchiolitis are rare in the US, RSV remains a significant cause of infant mortality worldwide. Children at higher risk for severe disease include those less than 12 weeks old at the time of infection, those who were born before 29 weeks' gestation, and those with underlying chronic pulmonary, neurologic, or hemodynamically significant cardiac disease.
Potentially modifiable environmental factors, such as exposure to secondhand smoke, may also contribute to more severe disease. Pathophysiology. While RSV is the classic cause of bronchiolitis and responsible for 50% to 80% of infections, many other viruses can cause similar symptoms, including rhinovirus, adenovirus, influenza virus, and parainfluenza virus.
After initially infecting the upper respiratory tract, the virus moves down to the terminal bronchiolar epithelial cells, where the infection and subsequent inflammatory reaction in the small bronchi and bronchioles result in epithelial sloughing, submucosal edema, and increased mucus production. Secretions tend to pool because of the loss of the ciliated epithelium, leading to airway plugging, distal air trapping, and atelectasis. Clinical presentation.
Children with bronchiolitis initially develop signs and symptoms consistent with an upper respiratory infection: rhinorrhea, nasal congestion, cough, and fever. Parents may also note decreased oral intake, general malaise, increased fussiness, and poor sleep, secondary to nasal congestion. The disease progresses to include signs of lower respiratory tract involvement, including increased work of breathing, worsening cough, and wheeze.
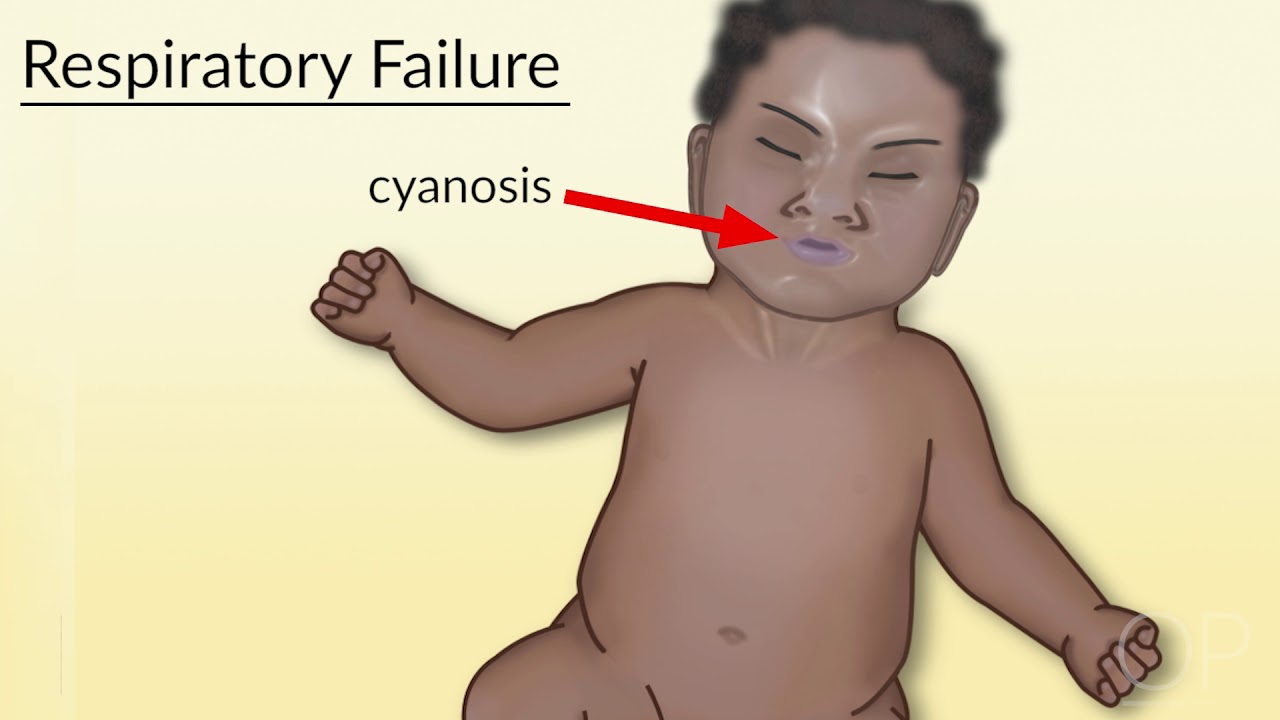
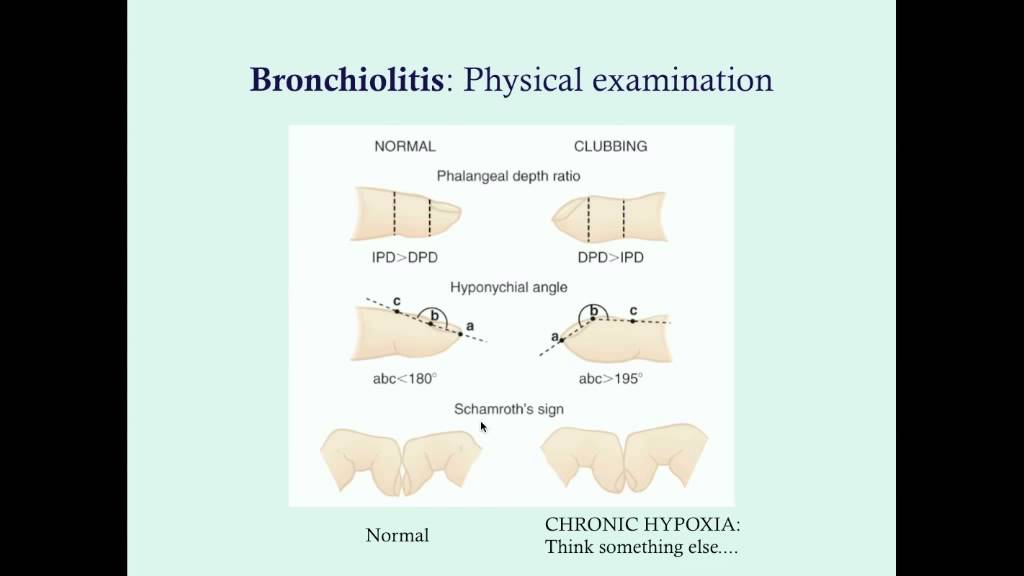
In addition to seeking details of these historical points, when seeing a child with possible bronchiolitis, you should ask about oral fluid intake and urine output, as dehydration is quite common. Also, make sure to ask about periods of cyanosis or apnea, as premature infants and infants less than two months old are at higher risk for apnea. When examining a baby with suspected bronchiolitis, first start with a review of the vital signs and an assessment of her general appearance.
Is the baby febrile, tachypneic, tachycardic, or hypoxemic? Does the baby appear interactive and playful, or is she lethargic or irritable? Assess for hydration status by checking fullness of the anterior fontanelle, presence of tears with crying, mucous membranes, and capillary refill.
Carefully observe for signs of increased work of breathing. Retractions can be supraclavicular, intercostal, or subcostal. If present, note whether these are mild, moderate, or severe.
Nasal flaring or grunting can be seen with more significant respiratory distress. Although you have yet to auscultate her lungs, you have already gathered some of the most important information that you'll need about her clinical status just by observation. The classic description of the lung exam of a baby with bronchiolitis is sounding like a "washerboard," with coarse crackles heard on inspiration and expiration.
Babies will frequently have associated wheeze, which is higher-pitched and polyphonic. Note whether there are specific areas where breath sounds are diminished compared to other areas. Because areas of mucus plugging can shift with cough, the areas of decreased aeration may shift over time.
Prolonged expiratory phase is also common. Diagnosis. The diagnosis of bronchiolitis is a clinical one.
Typically, chest X-ray and labs, including specific respiratory viral testing, are not necessary to make the diagnosis, nor are they recommended in the current guidelines from the American Academy of Pediatrics. Targeted testing in selected patients, for example, those with preexisting medical conditions, may be helpful to exclude alternative diagnoses. Viral testing may be helpful to cohort patients or in discontinuation of anti-influenza treatment.
Unusual features in the history, such as poor growth, recurrent or severe symptoms, or a clinical course that does not follow the anticipated pattern, should prompt consideration of alternative diagnoses. Bacterial pneumonia is a frequent consideration, particularly when auscultation reveals a consistent area of decreased aeration or when there is a high or persistent fever. Chest X-ray may be helpful in this situation, but caution must be taken to avoid overinterpretation of atelectasis as an infiltrate.
Recurrent viral-induced wheeze or reactive airway disease can be difficult to distinguish from bronchiolitis. Additional considerations may include oropharyngeal dysphasia leading to pulmonary aspiration, foreign body aspiration, chronic pulmonary disease, such as cystic fibrosis, or cardiac disease, such as heart failure. Management.
The care of children with bronchiolitis is mainly supportive, as there is no curative therapy. Supplemental oxygen should be used to avoid hypoxemia, and most guidelines suggest that maintaining oxygen levels greater than 90% to 92% is a reasonable target. In rare cases, bronchiolitis can be severe enough to require non-invasive ventilation or intubation for respiratory failure.
Nasal suctioning to clear secretions may be helpful, particularly before feedings, though care must be taken to avoid nasal trauma that can result in more swelling. The use of bronchodilators for either inpatients or outpatients is somewhat controversial. Current AAP guidelines recommend against the use of inhaled bronchodilators or inhaled or systemic glucocorticoids in the management of the first episode of bronchiolitis.
However, future studies may allow clinicians to prospectively identify children who are more likely to benefit from one or more of these interventions based on history, exam, and viral and/or bacterial testing. Indications for hospitalization include poor oral intake, leading to dehydration, hypoxia, apnea, or moderate to severe respiratory distress. Children without these features can be managed as outpatients with parental education on avoiding dehydration and reasons to return to care.
Bronchiolitis is a self-limited illness and will resolve in most children without complications. Interestingly, children with bronchiolitis severe enough to be hospitalized have an increased risk of recurrent wheezing and asthma, even into early adulthood. These children are also more likely to have eczema, high eosinophil counts, and a family history of asthma.
These observations have led researchers and clinicians to wonder whether bronchiolitis causes lung injury, which leads to asthma, or whether the underlying susceptibility to asthma also confers risk for severe bronchiolitis. The answer is still unknown, with some conflicting data, but the bulk of the evidence seems to point toward shared underlying susceptibility rather than direct lung injury inflicted by a viral infection. The best way to prevent transmission of the viruses responsible for causing bronchiolitis is to practice good hand washing techniques, using either alcohol-based hand sanitizers or soap and water, and to avoid contact with people who have an active infection.
Palivizumab is a humanized monoclonal antibody to RSV, given as monthly IM injections during the RSV season. It has been shown to decrease the risk of hospitalization among significantly premature infants and those with chronic lung disease or hemodynamically significant cardiac disease. But its routine use is reduced because of its prohibitive cost and need for monthly administration.
Currently, several new approaches to develop a safe and effective vaccine are being explored, but none is yet available for clinical use. Influenza vaccination should be given annually to children over six months of age. In summary, bronchiolitis is a viral lower respiratory tract infection affecting infants and young children, particularly in the winter months, and classically presents with increased work of breathing and coarse breath sounds.
Bronchiolitis accounts for a significant number of admissions and spending of health care dollars. Infants at higher risk for severe infection include those born prematurely and those with underlying pulmonary or cardiac disease. The most common viral agent is RSV.
Treatment is largely supportive, with particular attention paid to pulmonary toilet and correction of dehydration. Hospitalization with bronchiolitis is associated with future recurrent wheeze and asthma, though the causation has yet to be firmly established. Thank you for watching this video on bronchiolitis.