welcome to this lecture on osteoporosis in this lecture we'll cover what is osteoporosis what are the common risk factors and pathophysiology associated with osteoporosis what is the common complications associated with osteoporosis and then finally very briefly we'll look at how is it diagnosed how is it treated so osteoporosis is a term it's a compound word where osteo refers to bone porosis pause simply it just means our bones become weakened let's have a quick look at this particular diagram it's a typical bone and with all bones they have an outer covering this outer covering is known
as compact bone this compact bone is very dense bone tissue which means it's strong provides structural integrity but most importantly it stops compressive forces now deeper to compact bone which you can see in red is spongy bone this is less dense it has almost these little holes all the way through it which makes it look like a sponge and this is why it's called spongy bone but this tissue also allows for flexibility and strength but without the weight associated or as we found with the compact bone now when we look at bone i kind of
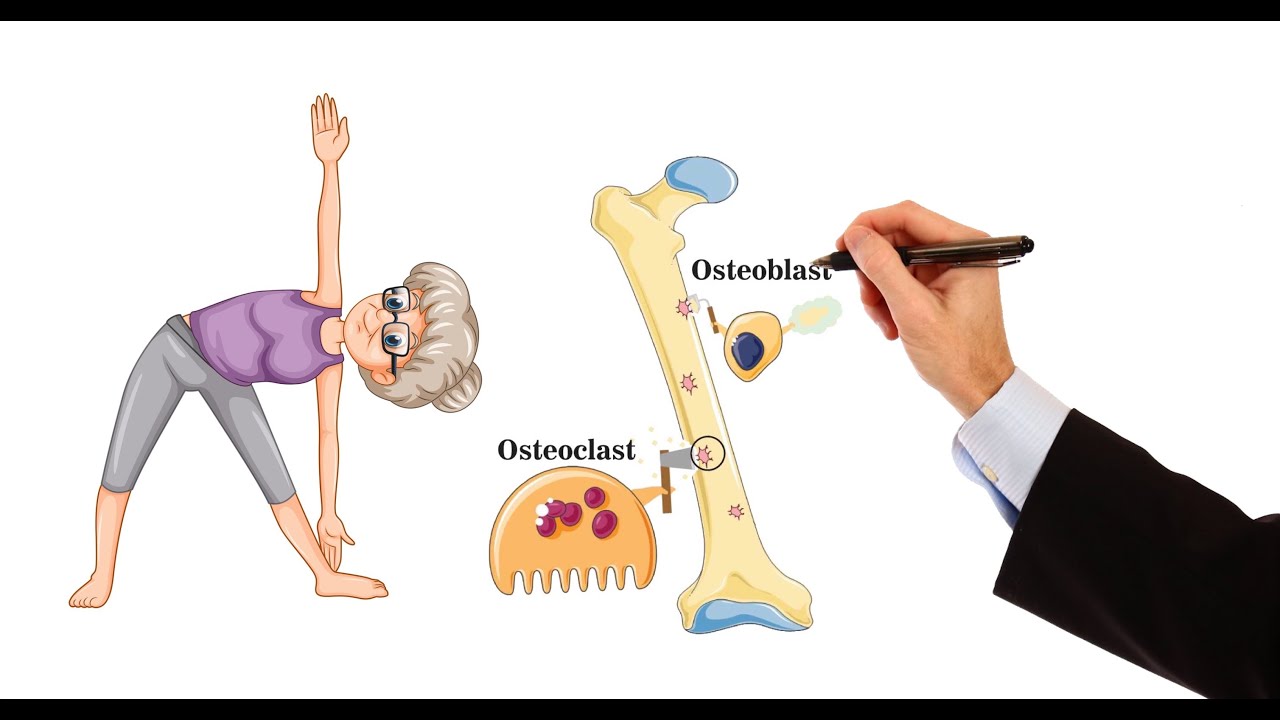
think of it like a a brick house we kind of think it's made it's there it's providing the support it doesn't do much else but in fact it's a very dynamic tissue which means it's constantly being turned over this this term is known as remodeling and actually this would prop this bone would probably remodel between four to ten years so the whole thing is reabsorbed and added back between four to ten years this is known as remodeling which is a balancing act between taking bone away which we call bone resorption and add a new bone
now the cells that take bone away is then known as osteoclasts now these are kind of like macrophages that take they eat away and take bone or reabsorb bone whereas bone cells that add new bone are known as osteoblasts so it's a balancing act between these two to keep this bone model remodeling process going now in our early ages of life so child adolescence the actual osteoblasts wind so we see more bone being formed which actually leads to the bone mass or our bone mass being peaked so we call this peak bone mass at the
ages of about 20 to 29 years so that means we have the strongest bones in this age so after this age peak bone max starts to drop off and we actually see approximately 0.7 dropping away each year that means the osteoclasts become more active after the 29 years in comparison to the osteoblasts so what kind of things in the early phases allow the osteoblast to be more active well probably the most important one are hormones so the hormones that we see that have the greatest effect on osteoblast activity would be estrogens more dominant in females
testosterone more so in males and growth hormone for both so these hormones which are higher in these periods would allow this cell to be more active in that phase other things is diet specifically calcium so calcium high amounts of calcium will activate or great greater activity for the osteoblasts and remember vitamin d increases calcium so those two kind of go hand in hand so diet is also important for that peak bone mass other things that are important is physical activity specifically loading physical activities is like putting your bones under stress like resistance training so this
is an important physical activity to generate the osteoblast activity now these things feed into the peak bone mass so if we don't have these things working or it's slightly reduced we actually see we have a lower peak bone mass which then would predispose someone to osteoporosis now with the peak bone mass because of the hormonal difference males will have slightly higher peak by mass than females so that's important to know why females will be at higher risk of osteoporosis it's actually at five to one so five females to one male and that's probably due largely
because of the hormone now other risk factors that come in to leading to osteoporosis i'm going to discuss now but before i do that it's just important to note there is two to two types of osteoporosis we have primary osteoporosis and secondary osteoporosis primary osteoporosis is broken into further two parts we have age related or senile osteoporosis and sex-related or post-menopausal osteoporosis and we'll talk about that when we talk about the hormones in a second the other type of osteoporosis is secondary that means you have a disease and osteoporosis is secondary to this disease now
some of the causes of this would be drugs so the most common drugs that can lead to osteoporosis would be corticosteroids proton pump inhibitors some anti-seizure medications and heparin they're the most common smoking and alcohol also can lead to that as well other causes of secondary osteoporosis would be endocrine disorders like too much cortisol too much thyroid hormone too much parathyroid parathyroid hormone or a drop in some of the gonadal hormones like estrogen testosterone some cancers can also lead to osteoporosis like multiple myelomas but we're going to focus on for the rest of this lecture
on specifically the age-related or senile and postmenopausal which are the primary causes so now let's look at how these risk factors feed into the pathophysiology of osteoporosis starting with age was as we said after the age of 29 years the osteoblast activity starts to drop in relative to the osteoclast so this becomes more dominant so age what will happen is age effects is the osteoblast number and activity will start to drop away that means bone formation will start to decrease another big factor which is important is estrogen levels and this is for the primary osteoporosis
being post menopausal osteoporosis so estrogen actually has a tropic effect to osteoblasts but also increasing or holding number so as ostrogen as estrogen starts to drop away after menopause the actual effect of this will start to diminish to a point where we lose two percent of compact bone per year and nine percent of spongy bone per year and this is why up to 40 percent of all females will have some degree of osteoporosis so estrogen having a huge effect for osteoblasts but also as the estrogen effect starts to drop away low estrogen will actually cause
the osteoclast activity to start increasing so that would be age and the sex effect physical activity will also see a drop in physical activity as we age so a drop in physical activity will will actually make the osteoblast activity less therefore we have a decrease in bone formation so that's the physical active diet and or diet this would be calcium and vitamin d also these things start to diminish in our diets as we age so that means bone formation also decrease drugs we spoke about but i'll just add one important one corticosteroids which we see
use for decreasing the immune response in some autoimmune conditions or asthma etc so corticosteroids would actually increase the activity of osteoclasts that means we have an increase in bone reabsorption and then finally genetics well this goes back to the peak bone mass in our earlier phases of life so it seems that caucasians and asians have a lower pigment bone mass compared to say africans so that's important for predisposing one to osteoporosis so from a decrease in bone formation and an increased reabsorption as we get older what that will do is decrease bone mass and by
doing that we have a decrease in bone strength now what happens is we start to see greater holes or spaces particularly in the medullary bone or the spongy bone which is why it's called porosis so this with a thinning of the compact bone is the most common changes that we see histologically in bones with osteoporosis so this is then going to predispose us to fractures the most common fracture location is the vertebra second to that is the neck of femur then we see wrist and ribs thereafter now it's important to note that the diagnosis for
osteoporosis is where we have a reduction in peak bone mass by at least 2.5 standard deviations away from the average so this would be the diagnostic objective point that would allow a diagnosis of osteoporosis how do we measure the peak bone mass well we can't just do it on a standard x-ray so we have to do a special x-ray which we call a dexa and this is a dual energy x-ray densiometer we can also use a quantitative ct but essentially these two will just look at the density of our bone finally how is it treated
how is it managed how the prevented well we want to ensure that our calcium and vitamin d levels are adequate adequate we want to ensure that we do the right physical activity other things that we could do is use drugs to decrease the reabsorption of bone these are bisphosphonates what they do is they decrease the activity but also they can cause apoptosis of osteoclasts we can also use some immunotherapy so monoclonal antibodies which stops the stimulation of osteoclasts or we can come across and for females particularly we can do some estrogen therapies so hopefully now
you've got a better insight into what osteoporosis is what it is pathophysiology risk factors how is it diagnosed and finally treated