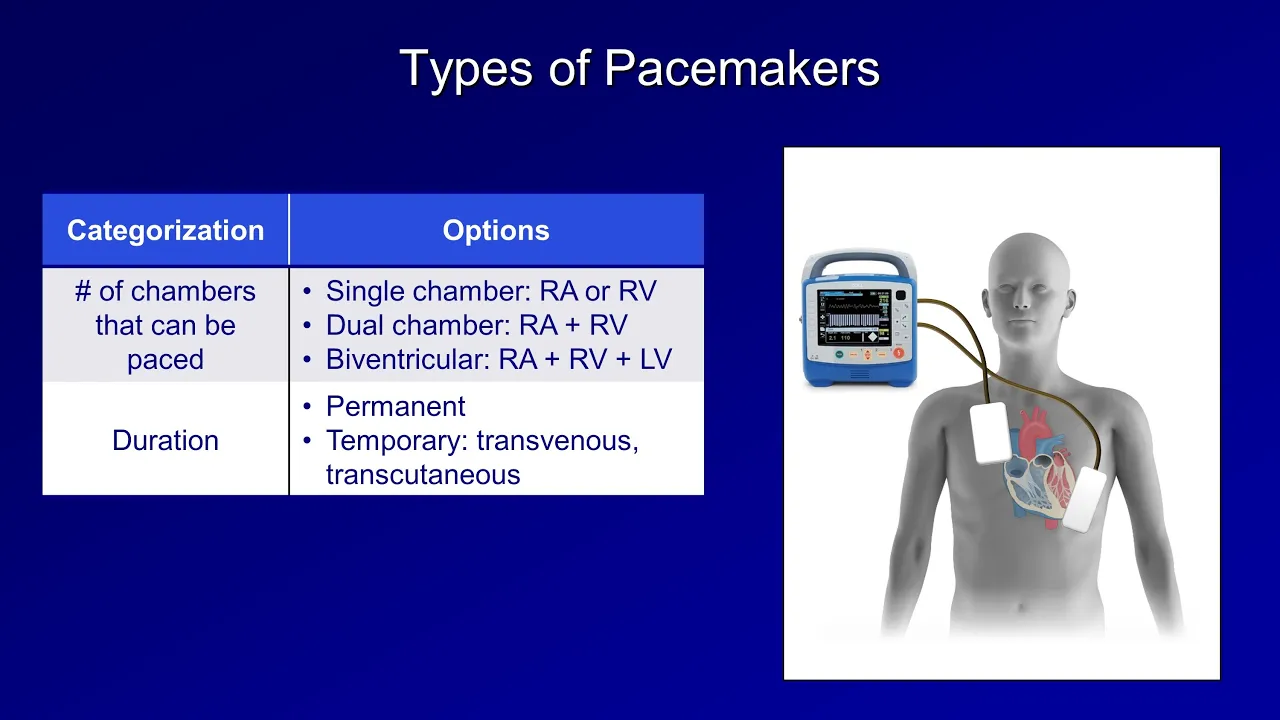
[Music] this is Eric from strong medicine and this is the first of three videos on the topic of pacemakers this one will cover the components of pacemakers there indications and their complications let's start off with what is a pacemaker it's any device which sends electrical impulses to the heart to stimulate cardiac contraction when its intrinsic electrical system is not functioning normally there are several different ways in which pacemakers can be categorized we can refer to pacemakers by the number of the heart's chambers that can be paced for example a single chamber pacemaker can either paste
the right atrium or the right ventricle a dual chamber pacemaker can paste the right atrium and the right ventricle and the biventricular pacemaker can paste the right atrium right ventricle and left ventricle pacemakers can also be categorized by their duration there are permanent pacemakers which is a little bit of a misnomer since the devices battery typically lasts only for five to ten years after which the part of the device called the generator needs to be replaced temporary pacemakers include transvenous ones in which the pacing wires are introduced into the body via one of the neck
veins and the actual power source and circuitry remained external such devices remain in place for several days to about a week or so temporary pacemakers also include transcutaneous pacemaker x' in which electrical current is applied to the patient's skin this is incredibly uncomfortable for the patient so this is only used during bradycardic arrests in order to buy time to place a transvenous pacemaker lastly there are epicardial pacemakers that are occasionally placed at the time of cardiac surgery and finally pacemaking devices can be categorized based on whether they do or do not have the ability to
defibrillate the heart in the event of ventricular fibrillation or sustained ventricular tachycardia which would classify them as an implantable cardioverter-defibrillator while most pacemakers do not have the ability to defibrillate almost all I CDs have some pacemaker function available whether or not the patient actually requires it the rest of this video and the second in this series will focus on permanent single and dual chamber pacemakers as these are the most common devices out there in the last video will cover biventricular pacemaker z' and ICDs permanent pacemakers consist of several basic components there is the generator sometimes
colloquially referred to as the can this is usually implanted in the left pectoral region under the skin and over the pectoralis major muscle the physical space which is dissected to make room for it is referred to as the pocket here's a u.s. quarter to provide an idea of its approximate size inside about half the volume is occupied by circuitry and half is occupied by the battery exiting out from the generator via the connector block also known as the header on top is one or more leads which consists of a wire surrounded by insulation at the
end of the lead is an electrode but usually has two poles in close proximity the leads are fed through the patient's central veins until the tips are against the myocardial of the relevant cardiac chamber there are several different mechanisms used to hold the leads in place but a metal helix referred to as the lead screw is the most common here's what a properly positioned dual-chamber pacemaker looks like on chest x-ray we see the generator with its battery and circuit this peach-colored line is the right atrial lead it's normal for it to curve slightly back superiorly
like this to be fixed within the right atrial appendage and the yellow line is the right ventricular lead the indications for placing a permanent pacemaker in a patient are long and complicated so I'll just provide a general summary of the most common ones class one indications that is those which are at universally agreed upon as having overwhelming benefits includes symptomatic sinus node dysfunction either sinus bradycardia or sinus pauses third or type 2 second-degree AV block regardless of symptoms and permanent atrial fibrillation with symptomatic bradycardia an exception to these class 1 indications are young unusually fit
patients who experience a symptomatic heart block but only while sleeping and then there are class two indications both 2a and 2b which collectively can be thought of as those for which there exists a minority dissenting opinion about either the presence or the degree of benefits situations in this category includes symptomatic Krona tropic incompetence which means a person's heart rate is fine at rest but the heart does not be more quickly with exercise or increased metabolic demand which often manifests as exercise intolerance also here is symptomatic pronounced first-degree or type one second degree AV block and
also patients who have syncope of unknown etiology with sinus node dysfunction uncovered or provoked during an electrophysiology study in the cath lab asymptomatic sinus bradycardia and asymptomatic sinus pauses are not indications for pacemaker placement regardless of indication reversible ideologies of the conduction disease must first be ruled out before placement of a permanent device reversible ideologies can include medications infection electrolyte disturbances and ongoing ischemia I'll close this video by going through the complications of pacemakers complications can be categorized based on those which are directly related to the implantation and those which are delayed by weeks months
or even years implantation related complications include a hematoma in the pacemaker pocket a pocket infection pneumothorax hemothorax lead dislodgement which is when the lead slips out of place within a handful of days after implantation and very rarely cardiac perforation by the lead resulting in cardiac tamponade delayed complications include a lead fracture which refers to a discontinuity of the conducting wire within the lead a break in the insulation which results in current leaking out of the lead infection of either the pocket or the lead the latter of which can complicate endocarditis thrombosis or stenosis of the
veins through which the leads travel there is something called pacing induced cardiomyopathy which a patient can experience a drop in ejection fraction and thus systolic failure on account of dis synchrony between contraction of the right and left ventricles which is caused by the fact that the RV lead necessarily causes RB depolarization before the LV mimicking the effect of a very pronounced left bundle branch block this problem is particularly amenable to cardiac resynchronization therapy as will be discussed in the third video in this series there's another complication called pacemaker syndrome pacemaker syndrome has very definitions but
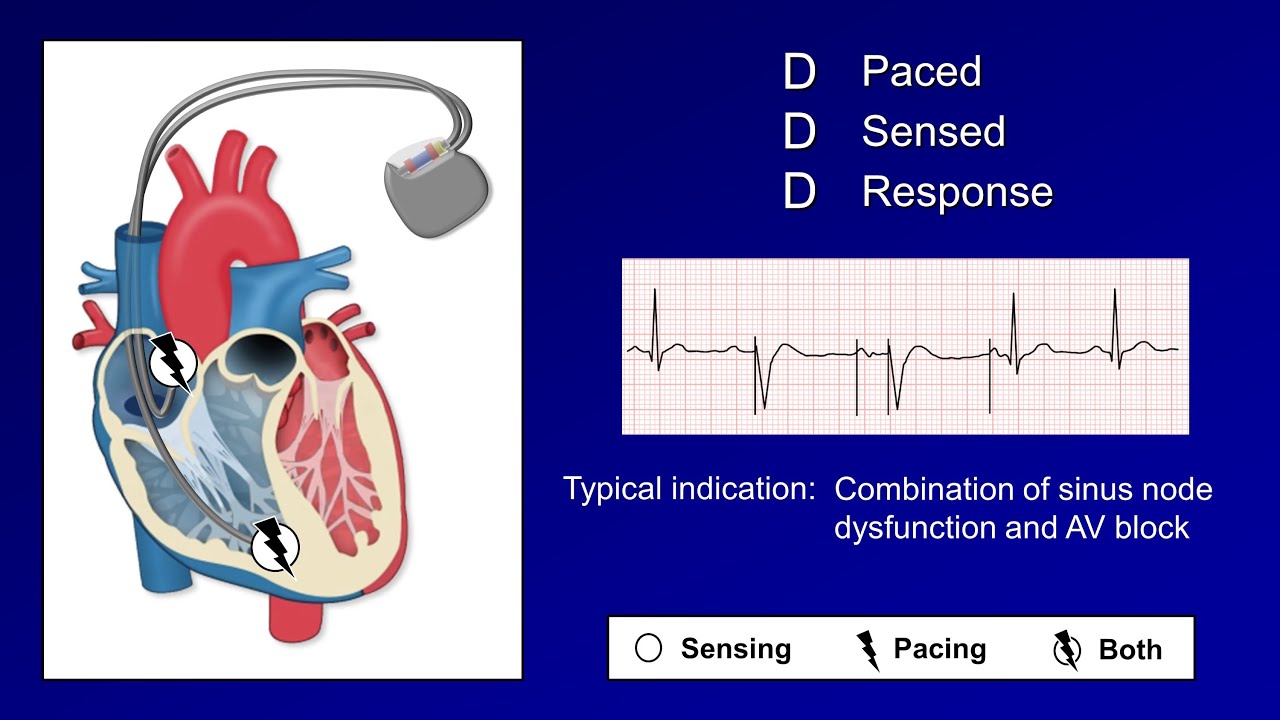
most commonly is considered to be the constellation of dyspnea chest discomfort palpitations and neck fullness which is specifically caused by atrial ventricular dissociation because of the overlap in symptoms and the usage of the terms pacing induced cardiomyopathy and pacemaker syndrome it's been suggested that these be renamed vv2 synchrony and abd synchrony respectively but this has not caught on the last complication is pacemaker mediated tachycardia or PMT which occurs when the pacemaker interprets a pacing spike in one chamber as a native electrical impulse in the other for example a ventricular pacing spike sends a retrograde P
wave back to the atria which is sensed by the atria lead as native atrial depolarization triggering another ventricular pacing spike leading to an endless loop it looks like an atrial sensed ventricular paced rhythm at or near the devices operate limits also called the maximum tracking rates newer pacemakers use algorithms to detect the presence of this arrhythmia and to terminate it that's it for this video the next one in this series will cover pacemaker modes and settings [Music]