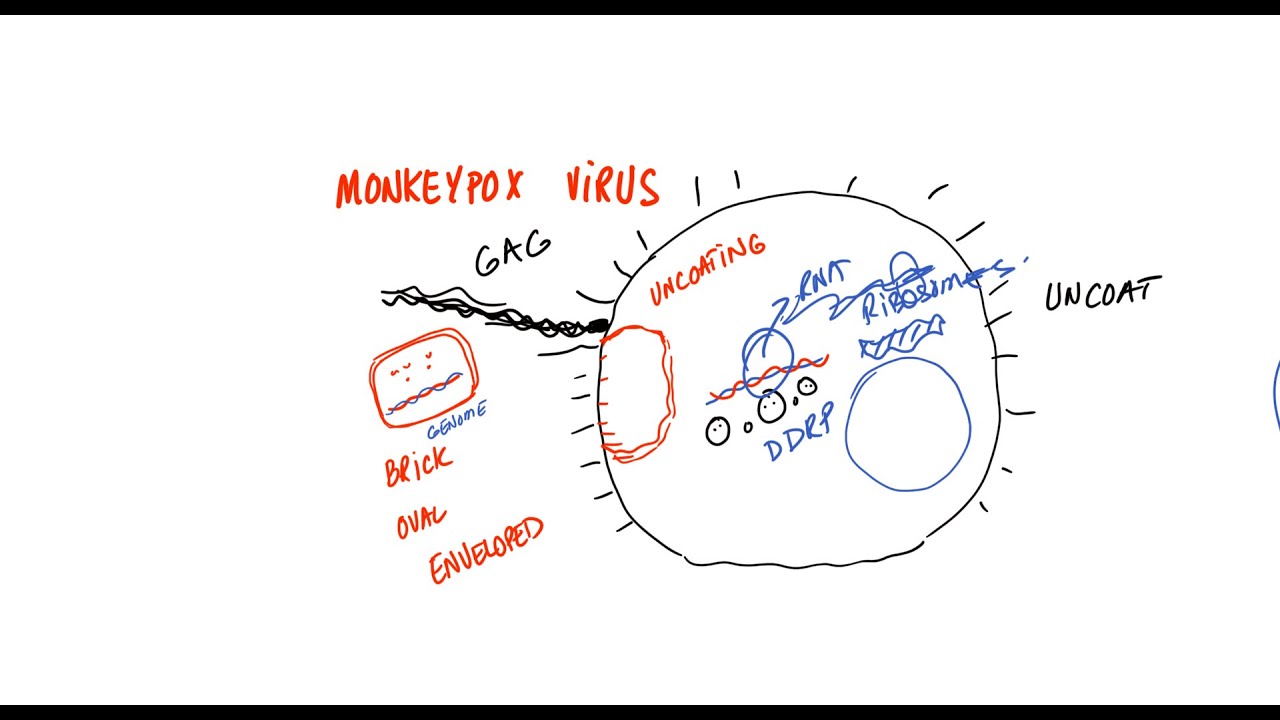
in this session we're talking about mpox which was previously known as monkey pox so this is a disease caused by infection with a virus known as the impox virus and this impacts virus is a pox viridae virus and it's in the genus Ortho pox virus is in the same genus as smallpox so it can cause a prodromal or a flu-like illness at first and then cause a rash later so it looks like smallpox but it's not going to be as severe and it's going to be less infectious than smallpox now mpox virus is a relatively
large virus and it's often described as brick-alike in appearance and it is a double-stranded DNA virus now mpox is a zoonotic infection meaning that it is spread from animals to humans but when it gets into the human population it can spread from Human to human but humans are incidental hosts meaning that they're not the hosts that this virus actually is looking for the virus is looking for particular animal hosts which we'll discuss in the next slide now there has been an increasing prevalence recently of infections with this particular virus and an outbreak did start in
2022 and as of early 2023 there have been over 30 000 cases reported in the United States now let's discuss a brief history of this virus some of the first known cases and how it has spread so this particular virus was actually first isolated in lab monkeys that were sent from Singapore to Denmark in 1959. these monkeys arrived in Denmark and became ill and this particular virus was actually the cause of their illness this is the first known case of this virus so that was in a monkey and this is why the term monkey pox
came to be but the first human infection was actually reported in Zaire which is modern day Democratic Republic of Congo in 1970. there were then additional cases in Cote devoir Liberia Nigeria and Sierra Leone so some of the earliest cases started in central Africa and then we started seeing more on the West Coast of Africa then over the next couple of decades cases of this virus start to increase in Central and western Africa and this increase in cases may be due to the cessation of the use of the smallpox vaccine the smallpox vaccine is known
to actually suppress or limit the ability of impacts to cause infection or it leads to a milder form of infection so smallpox was eliminated in the world in 1977 and then afterwards the use of smallpox vaccine started to be in Decline and then after that point we start seeing more cases of mpox even with these increasing case numbers it was still limited to Western Africa until 2003 when the first cases started to appear in the Western Hemisphere so this was due to transportation of animals from Africa to the United States then we start seeing cases
appear in the United States but we don't really see a large amount of human-to-human transmission most of it is from animals to humans but starting in May 2022 we start seeing more human to human trans Mission this is when we start seeing increasing Global case numbers initially we start seeing cases in the United Kingdom that first came from a traveler from Nigeria so initially there's only a handful of cases but by the end of 2022 there's thousands of cases that have been identified on all inhabited continents and as we previously mentioned over 30 000 cases
have been identified and reported in the United States alone let's discuss how this particular virus is transmitted so one way that this virus can be transmitted is through droplets so droplet contact is going to be from close contact so if you're up close with an individual and they are talking to you there can be some respiratory droplets that are exuded out but you would need prolonged face-to-face contact it's not going to be something where you walk by an individual and you get infected you have to be in close contact for a long period of time
another very important way that this virus can be transmitted is through direct contact so some of the ways that this has been previously transmitted via direct contact is through contact with infected animals so these include prairie dogs or squirrels or monkeys or pigs or other animals as well including hedgehogs and it does seem to be the case that the natural reservoir for this particular virus is African rodents we mentioned before that humans are incidental hosts monkeys are also incidental hosts as well so they're not the host that the virus is looking for they just simply
can cross a species barrier infect monkeys or humans and then that can be an incidental host but the natural reservoirs are the main hosts that this virus is going to use along with contact with infected animals you can have contact with the animal reservoirs themselves these again include African rodents like gambian rats is one of those species another way of getting this by direct contact is through ingestion of contaminated animal products and then what's been driving the most recent outbreak from May of 2022 has been human to human spread and this human human spread is
going to be via skin-to-skin contact and the majority of these cases have been through sexual transmission so skin to skin contact especially through sexual transmission this has been the main driver of the most recent outbreak and other ways that this can be transmitted is through indirect contact so indirect contact is going to be contact with clothing or other Fabrics that have had contact with the skin lesions or other bodily fluids and another one would be fomites fomites would be furniture for instance if there's bodily fluids or if there's been contact with the fluid from skin
lesions this can all be ways that transmission can occur and then another method of spread is through vertical transmission so vertical transmission is going to be from pregnant female to developing fetus or infant so it can be in the blood of the pregnant patient it can cross the placental barrier and infect the develo helping fetus in all of these methods of transmission are going to be due to the fact that this virus can be at high levels or high concentrations in not only the fluid from the skin lesions themselves but can also be in high
amounts in the bodily fluids of patients who are infected this can include the saliva the blood vaginal fluid and semen so all of these can have high amounts of this virus that can Aid in transmission of the virus to other individuals let's talk about the pathophysiology of infection with mpox virus so if you're exposed to this virus either through droplets or through skin contact it can enter into and penetrate through the oropharynx or the nasopharynx so some of those mucosal membranes can also get in through the skin as well so again we talked about that
skin to skin contact before and the inbox virus is going to use particular viral surface proteins to enter into host cells and one of those viral proteins is known as f-13 and when it actually enters into its site of inoculation it can then spread into local lymph nodes so local lymph nodes are going to be the first site we're going to see this virus going to and then it can multiply in those lymph nodes and then eventually enter into the blood it will enter into the blood in what we call the initial viremia stage so
this is the first time it enters the blood it's going to be the initial vairmia so viremia is just a word for virus in the blood and then after this initial viremia stage is going to enter into other organ systems it can spread into other organist systems via the blood and then it will stay in those organ systems and then it will eventually leave those organ systems and enter into the blood again and that is what we would call secondary viremia and this is when we actually have symptom onset of this particular condition which means
that the time at which we get the virus and it goes through the lymph nodes initial viremia and goes into the organ systems and then leaves the other organ systems to enter the blood for the second time that secondary viremia that is the incubation period and that incubation period can go anywhere from 4 to 21 days and approximately most cases are going to be around 12 days so the incubation period is going to be the time at which you first get infected and then you start seeing symptoms so again it takes up to 21 days
now let's talk about the clinical findings or the signs and symptoms of an mpox virus infection so we're first going to have a pre-erruptive or prodromal stage this is going to be a stage where the patient feels like they have a flu-like illness and it's going to occur one to four days prior to onset of the rash so when we think about mpox virus infections we're thinking about the rash but there's actually going to be this prodromal stage that occurs before the rash so one to four days prior to onset of the rash we're going
to have these symptoms these include a fever so the fever can be 38.5 to 40.5 degrees Celsius so it can be a relatively high fever so this is actually going to be the most often the first sign of infection and then patients can often have chills and sweats as well they can also have a severe headache myalges and back pain so myalges are going to be muscle aches and pains they can also have anorexia reduced appetite so all very common with a viral infection they can also have malaise and fatigue so feeling generally unwell and
tired and then they can have pharyngitis or sore throat dyspnea or shortness of breath in a cough so again very vague and non-specific flu-like symptoms but something also very important with regards to this prodromal stage is that they can have lymphadenopathy we talked about the fact that the virus can enter into the lymph nodes and then more multiply in those lymph nodes they can cause lymphadenopathy again lymphadenopathy is going to be swollen tender lymph nodes and it occurs within two to three days of fever onset this is actually going to be the most important sign
to distinguish monkey pox from other pox virus infections in the locations where we can have these swollen tender lymph nodes are often going to be related to the initial place of infection and some of them can include the cervical chain so some lymph nodes in the neck the submental so this would be under the chin submandibular so along the jawline and then inguinal in the groin area so again the cervical chain the submandibular and submental lymph nodes and then the inguinal lymph nodes can all be places where we can see these swollen tender lymph nodes
and then after those one to four days of the prodromal stage we can have what we call the eruptive or xantham stage this is where we see a skin rash so the skin rash is going to look like this the rash is often going to begin on the oral mucosa so inside the mouth and then spread to the face and other areas of the body so very key and interesting point to make note of here we can see it on the trunk the extremities and the scalp and then it also may have a predilection for
occurring on the palms of the hands and the soles of the feet as well in cases in the most recent Outbreak The lesions seem to first appear on the perianal and genital areas so this can contribute to that skin to skin transmission the skin rash is going to slowly develop into a vesicular or vesicle pustular rash we'll talk about this in more detail in the next slide and the lesions can be anywhere from 3 to 15 millimeters in diameter emitter and the skin lesions can be up to thousands of them and these particular skin lesions
will develop in stages over the course of 14 to 21 days let's talk about those stages of this particular skin rash so it's going to start out as macules and papules so macules are going to be flat skin lesions and papules can be slightly raised skin lesions so they can start off flat or slightly raised and then they're going to go through a set of different stages so they can become vesicles which are raised skin lesions with a little bit of fluid in them they can then become pustules or pus-filled so they can have a
little white head on them they can then undergo umbilication which is the formation of little dot in the middle so umbilication is connected to umbilicus which is a belly button so these skin lesions can be described as having a little belly button or a spot on them or a little indentation on them over time they will then start to dry out they'll cross over and then they will start to de-squamate or start to sloth off so they can have their skin start to peel off over time this can occur over two to four weeks and
some of these skin lesions can leave scarring so we can see pitting scars on some patients now there are other important complications with impox viral infections these include secondary bacterial infection you can imagine that if you've got these open wounds on different parts of your body you're more likely to have a secondary bacterial infection so bacteria getting into those open wounds and causing a skin infection some patients can also have respiratory distress some patients can also have eye issues like keratitis and corneal ulceration and then in other patients the infection can be so severe that
we can have septicemia or an infection in the blood and then there can also be in some cases infection into the brain leading to Encephalitis or an inflammation of the brain these other complications are going to be more likely to occur in patients who are immuno compromised so very young patients very old patients patients on chemotherapies or who have cancer or patients who are diabetic or have co-infection with HIV or Aids so all very important to make note of when we talk about these complications now let's discuss how clinicians make the diagnosis of mpox viral
infection actions so the diagnosis is going to be via laboratory methodology so taking a sample from a suspected case and then looking at that sample either in culture so if the m-pox virus is isolated this is one way to make the diagnosis other ways include PCR identification of the impacts virus and then electron microscopy if there's electron microscopy that demonstrates an orthodox viruses can be enough to make the diagnosis as well and then other diagnostic criteria can be used without laboratory investigation although this would be less preferred this way of making the diagnosis can involve
the fact that if the patient has had contact with a known infection or known infected individual and they have symptoms that are the symptoms we just talked about in this lesson at up to 21 days after exposure that can be enough to make the diagnosis as well if it's past 21 days or if there have been no symptoms after 21 days then we don't have to worry about this as we mentioned before the incubation period goes up to 21 days and then other blood work can be performed which can show leukocytosis this is a high
white blood cell count and then serology testing can be performed to see if the patient has antibodies against impox virus how do clinicians treat this particular viral infection so the treatment of mpox viral infections is often not going to be required because this particular infection is going to be self-limiting so it's going to typically resolve on its own over the course of two to four weeks most of the time what is going to be used is supportive treatment so just helping the patient along with some of their signs and symptoms we talked about before so
treating the symptoms because oftentimes this is going to resolve on its own if it is in one of those cases where there is a complication if it's in a patient who has immunocompromise oftentimes we're going to need other treatments these can include antiviral therapies so one of them is going to be tecoviromat or teapots this was initially a treatment for variola virus and it works by blocking that f-13 Viral protein we talked about before so this is a potential antiviral treatment for this condition and then in patients who have ocular mpox so if they have
those ocular findings we talk before systemic antivirals can be important again tachoviramate and adding trifluridine can be important as well and some other important prognostic information with regards to empox viral infections include the fact that having impox infections can be fatal it can lead to mortality so some of the earlier estimates before the last outbreak showed that in African populations who were infected with mpox there was approximately one to ten percent mortality rate but what's important to point out is that the mortality is most often going to be due to a secondary infection or in
patients who have immunocompromise we talked about some of those complications before septicemia and Encephalitis for instance so the mortality rate is definitely going to be higher if co-infected with HIV or being immunocompromised and we did talk earlier about the smallpox vaccination which is known as vaccinia if you were vaccinated with vaccini you're likely to have a milder form of this particular disease and there are some vaccinations for mpox that can be utilized as well help reduce the severity of infection please check my lesson on vaginal candidiasis and gonorrhea and if you haven't already please like
And subscribe for more lessons like this one thanks so much for watching and hope see you next time