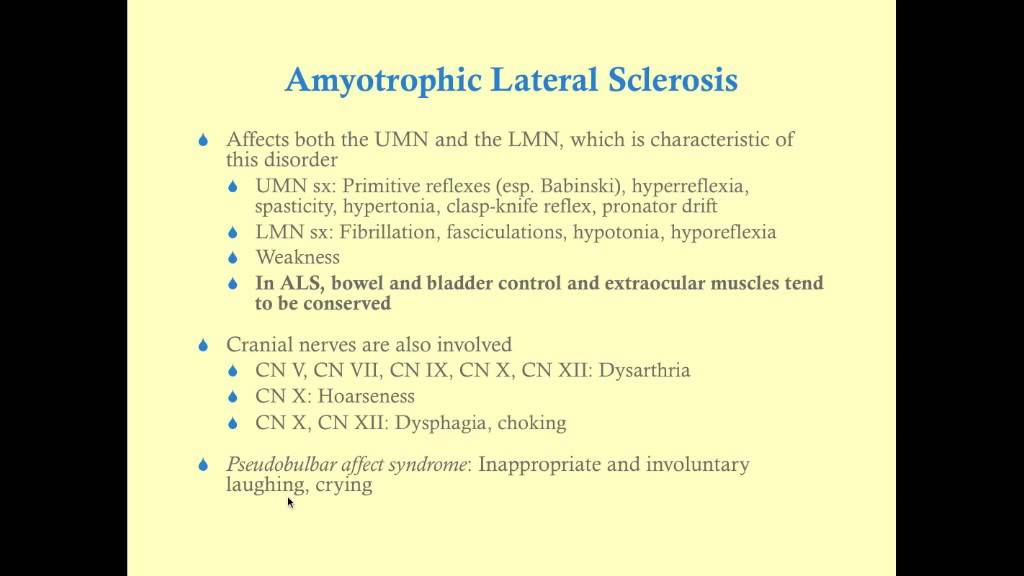
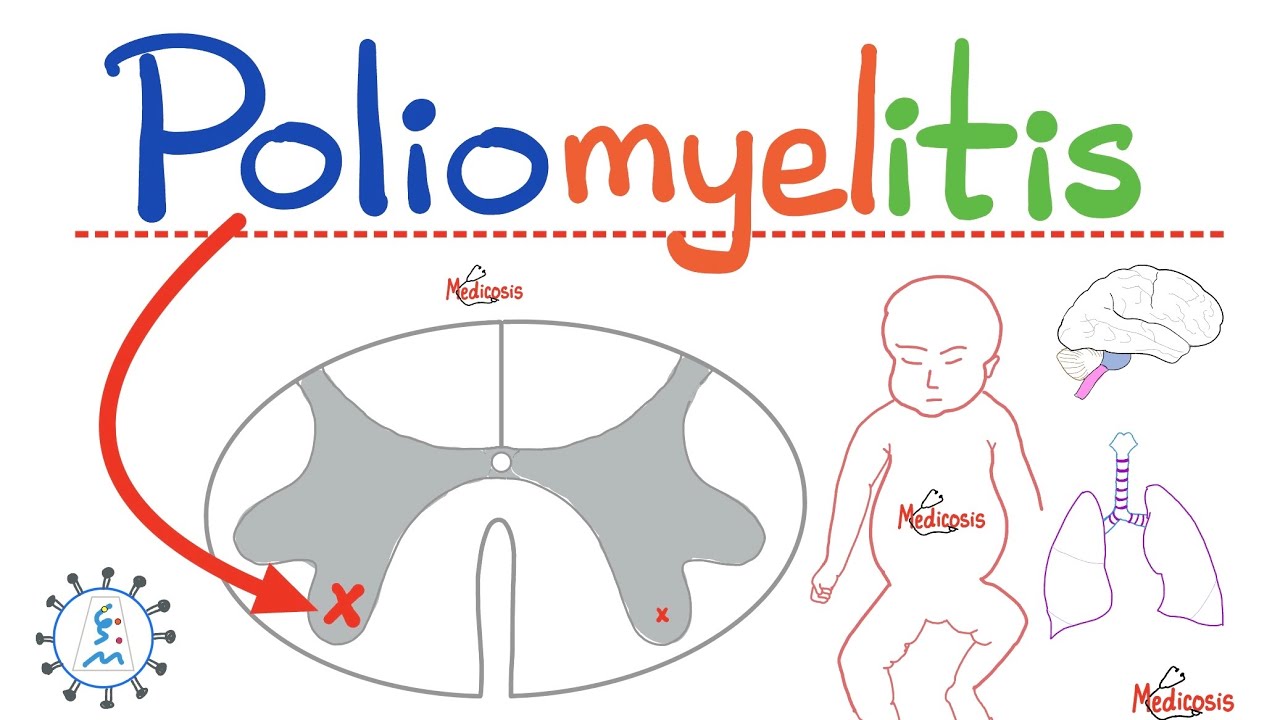
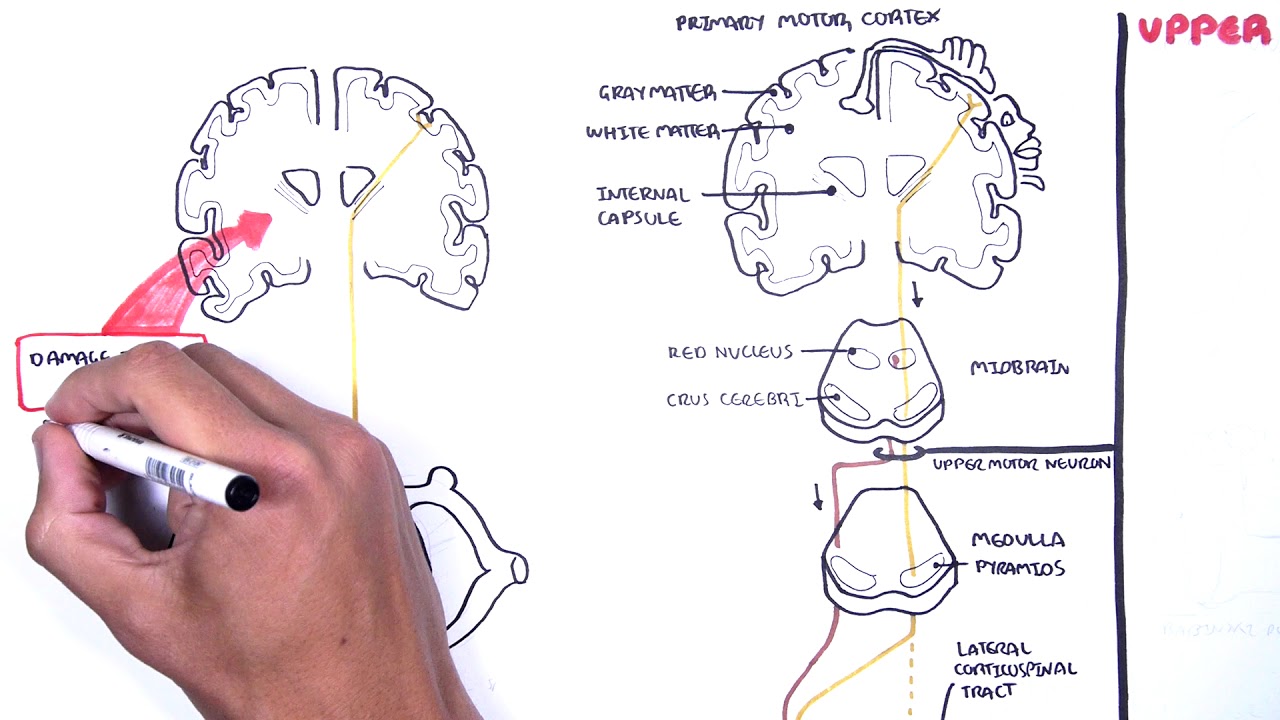
what is going on wonderful people it's meosis perfectionis where medicine makes perfect sense welcome back to my neurology playlist in previous videos we talked about neuroanatomy neurophysiology neuropharmacology and neuropathology we talked about diseases such as stroke ischemic and hemorrhagic we talked about the different types of shock including neurogenic shock we talked about the Cushing Triad of intracranial hypertension we talked about hydris brain herniation and idiopathic intracranial hypertension we talked about multiple sclerosis which is demalation of the central nervous system and gon B syndrome which is deyin of the peripheral nervous system we discussed myasthenia gravis and Lambert eaten myasthenic syndrome we talked about poliomyelitis vertigo and Min disease today we shall talk about one of the most horrible diseases ever Amit trophic lateral sclerosis which causes muscle paralysis and muscle wasting click the like button click the Subscribe button and let's get started am trophic lateral sclerosis has many names you can call it AIT trophic lateral sclerosis or abbreviated as ALS you can call it motor neuron disease or lar disease or shako disease but why do we call it each one of these names let's start by Amit trophic lateral sclerosis what does a mean a means no what does Mayu mean Mayu means muscle how about trophic it means growth oh so there is no muscle growth which is a nerdy way of saying muscle wasting why do we call it lateral because it affects these parts of the spinal cord as you see what are the names of these tracts these are the lateral cortical spinal tracts hence the lateral why sclerosis sclerosis means hardening as in atherosclerosis hardening of the vessels and ALS which is hardening of the muscles because these muscles are stiff they are # paralysis and that's why it's called amyotrophic lateral sclerosis why do you call it motor neuron disease because it's a disease that affects nerve cells causing motor deficits not sensory deficits why lugar's disease lugaric was a famous baseball player in America who suffered from ALS why do we call it shako disease named after the famous neurologist of the 19th century Jean Martin shako if I am your patient and you are my neurologist supposed to take care of me before I let you do anything I'm going to ask you one question what do you know about Je Mar Sho if your answer is Jean who I'm leaving your hospital I will decline treatment I would rather succumb to my own psychosomatic Neurosis then be treated by a schmuck who does not know who shako was half of the Neurology textbook is named after shako such as sho's artery which is the lenticulostriate artery please refer to my video on stroke to learn more and shako Joint which is a disease that happens to patients with diabetes shako disease is alss or a trophic lateral sclerosis sh Mari tooth disease shco V brand disease which is visual agnosia the infamous aneurysm of chco bushard aneurysm and for gastroenterologists there is shako Triad which we see in acute colangitis referred to my video on cystitis to learn more there is also the shako Triad of multiple sclerosis and shako Laden crystals which are microscopic crystals made of ashic proteins that we find in patients with asthma or parasitic pneumonia and that's why I was mad at my neurologist because I want my personal doctor to know what the french toast he talking about if you want to see more videos like this in the future please drop a brain Emoji in the comments I have two playlists on this channel dealing with neuro one is called neuroanatomy and the other is called neurology neurology has everything it has neuroanatomy neurophysiology neuropharmacology and neuropathology back to basic Basics we have central nervous system and peripheral nervous system the central nervous system is made of brain and spinal cord that's it the peripheral nervous system is made of cranial nerves and spinal nerves so by definition when I say nerve it is peripheral there is only one exception to this can you name a nerve that is part of the CNS rather than the pns please comment below so here's your nervous system we have central nervous system and peripheral nervous system central nervous system brain and spinal cord peripheral nervous system cranial nerves and spinal nerves how many cranial nerves do you have 12 pairs how many spinal nerves do you have 31 pairs I want you to master neurology like it's nobody's business and to do so you have to understand the lingo the language of neurologists what is inop this is pathology of the brain and by brain I could mean anything it could be the cam it could be the basil ganglia it could be the midbrain the pawns the medulla the cerebellum don't care all of this is incopy under incopy we have subtypes let's say that I have inflammation of the brain substance itself this is called analitis let's say that their inflammation is just in the cerebrum not the cerebellum not the brain stem not the basil ganglia just the cerebrum this is cerebritis a collection of pus in the brain is brain absis if it's in the cerebrum cerebral absis to be specific inflammation of the menes that cover the brain and the spinal cord is called menitis we're done with the brain let's talk about the spinal cord if the pathology is in the spinal cord itself it's called myopathy if it's inflammation it's militis if the pathology is in the nerve root as it exits the spinal cord it's radiculopathy but if the pathology is in the peripheral nerve it is peripheral neuropathy if the pathology is in the muscle it is myopathy if the pathology is in a channel such as a calcium channel or chloride Channel or potassium Channel it is a channelopathy and this is why senior Pathologists call me daddy if you wish to download these doozy colorful notes go to medicosis perfection. I help you learn understand and pass exams if you want me to personally tutor you reach out to me on my website I can tutor the medicine out of you quick review of the anatomy of the spinal cord if you've watched my neuro Anatomy playlist you will recall rule number one thou shall draw your Line in the Sand anterior is mostly motor posterior is mostly sensory and of course motor is eer but sensory is AER and because what's good for the goose is good for the gander the same concept applies to the spinal cord anterior is mostly motor posterior is mostly sensor for example this is the anterior horn cell it has motor functions but this is the posterior horn it has sensory functions again motor is eent so the this is the epher roote which is ventral root because we are in front of the line but the sensory is the efferent and its dorsal root as you see then we have a spinal nerve which is mixed it has motor and it has sensory fibers in it as you see the spinal cord has gray matter which has anterior horn lateral horn and posterior horn it also has white matter which has columns or Funiculi this is the posterior funiculus these are the lateral Funiculi and these are the anterior Funiculi this is the Soma and this is the axon of your neuron the Soma cannot be melinated it's always unmated and if the Soma is unmated therefore it has to be part of the gray matter such as this you find a bunch of SAS here A bunch of Somas there a bunch of Somas there similarly in the brain there is gray matter but it's on the outside so what's in the gray matter a bunch of SAS as you see this is a Soma and then the axon will be melinated and that's why the axon is part of the white matter in the brain speaking of axons some of them are melinated and they will be part of the white matter some of them are not melinated and they will be part of the gray matter so the white matter has one thing only mated axons the gray matter has two things it has unmated axons and it has Somas to understand what's going on in patients with AMI trophic lateral sclerosis or ALS we got to talk about the upper motor neuron and the low lower motor neuron and it goes like this suppose that you want to contract your left biceps in order to flex your left elbow the impulse has to start from the right side of the brain not the left where do I start in the primary motor cortex of the brain it's part of the pre Central gyus in front of the line in the sand in front of the Central sulcus and then these fibers will descend we're still on the right side of the brain we're going to pass through the posterior limb of the internal cap and then we are in the midbrain occupying the crust cerebra or the cereal peduncle then we're going to occupy the Basler part of the ponds basis pontis which is in the anterior half of the ponds and then we're going to go to the medary pyramids in the pyramids of the medila we're going to cross to the opposite side from right to left for example this is called the motor decussation or the pamal decussation now I am on the left half of the body I'm going to descend here in the spinal cord occupying the lateral funiculus hence amyotrophic lateral sclerosis because this is the lateral corticospinal tract after this the neuron will end by synapsing here so that will be the end of the first neuron which is the upper motor neuron and this will be the beginning of the second neuron which is the lower motor neuron as you see here until we reach the biceps your left biceps to be specific this lower motor neuron fiber of the muscular cutaneous nerve is going to spit acetylcholine onto the biceps the biceps will accept that spit that neurotransmitter by means of its doozy receptor known as nicotinic subm this is nicotinic this is for muscle a skeletal muscle that is let's do it again you decided to contract your left biceps so the impulse has to start from the right half of the brain in the right primary motor cortex in the right precentral gyrus and these are the Somas the SAS cannot be melinated so we're talking gray matter here then these axon fibers are melinated so they are part of the white matter of the brain will occupy the posterior limb of the internal capsule and then the cross cerebri of the midbrain the basis pontis of the ponds or the Basler part of the ponds and then will occupy the pyramids of the medila we are going to cross in the vicinity of the Medela # peramal decussation because this is paramal tract why do you call it because it occupies the pyramids of the Medill recall that your Medill has pyramids and has olives the pyramids are for the paramal tract the olives are for the extra paramal tract to learn more please refer to my neuroanatomy playlist this doy upper motor neuron cell is going to cross to the opposite side from right to left as you see we cross in the Meda then we'll descend in the spinal cord occupying the lateral finicula of white matter with which is the lateral cortical spinal tract why do you call it cortico because I started in the cortex why do you call it spinal because I'm going to end in the spinal cord and why do you call it lateral because I'm here laterally and why is it attract because attract by definition is a collection of axons in the central nervous system remember that the brain and the spinal cord are part of the central nervous system the end of this upper motor neuron will be here at the anterior horn cell it will synapse with the lower m motor neuron at the anterior horn cell this is also known as the primary motor neuron the first one is upper motor neuron the second one is lower motor neuron the first one is a tract because it's part of the CNS the second one is a nerve because it's part of the pns so what's the problem in patients with amytrophic lateral sclerosis or laric disease the problem is that the upper motor neuron is destroyed hence the name Lal sclerosis and if that was not enough the lower motor neuron is also destroyed hence the name motor neuron disease what are the signs and symptoms of upper motor neuron Legion and what are the signs and symptoms of lower motor neuron leion upper motor neuron it's hyper hyper positive but lower motor neuron it's hypo hypo negative upper motor neuron hypertonia hyper reflexia positive ainy everything is up reflexes up they are heightened the tone up even the toes are Fanning up but in lower motor neuron it's hypo hypo negative everything is down the reflexes down the tone down and even the toes are curling down upper motor neuron lesion usually has pareses because of the spasticity this disease is known as latal sclerosis sclerosis from the stiffening lower m neuron lesion causes flaccid paralysis both cause muscle weakness in upper motor neuron there is no atrophy no fasiculations lower motor neuron there is atrophy and Fa ciculation So what's going to happen in patients with Amit trophic lateral sclerosis the answer is a mixture of all of these These are the diseases that cause muscle weakness why do I have muscle weakness we're not talking about General fatigue as in anemia but we're specifically talking about muscle weakness here are the possibilities the problem could be in the anterior horn cell of the spinal cord we see this in patients with potis spinal muscular atrophy and today's topic amrop Latos sclerosis if the problem is in the nerve root it is radiculopathy gon B syndrome does that if the problem is in the peripheral nerve this is peripheral neuropathy gomber syndrome also does this don't forget diabetes alcohol can also destroy peripheral nerves hypothyroidism ureia from renal failure and much more then we have diseases of the neuromuscular Junction these include myasthenia gravis and Lambert Ean myasthenic syndrome then we have the muscular distrophy including duen muscular distrophy and Becker's muscular distrophy metabolic myopathies are many a famous one is mardal disease which is a glycogen storage disease congenital myopathies are many and they include the inherited mitochondrial disorders does anyone remember the Ragged red fibers so what disease is this what's the name of the disease that destroys both lateral cortical spinal tracts in both lateral Funiculi of the white matter of the spinal cord and also destroys the enior horn cell on both sides the answer is this is AIT trophic lateral closis or lugaric disease it's an upper motor neuron lesion and a lower motor neuron lesion this is ALS it has upper motor neuron lesion on both sides and lower motor neuron lesion on both sides and that's why this disease can lead to quadri plasia here is everything you need to know about Als in one slide ALS or lar disease or motor neuron disease or shako disease is a neuro generative disease where there is degeneration of my nervous system upper and lower motor neurons it is also a neuromuscular disease because I have muscle weakness caused by a neurological problem it can happen in males and females it's relatively more common in males than females with a male to female ratio of 1. 8 to1 the typical patient is between 50 and 70 that's usually when the disease is done diagnosed for the first time there is a very important distinction in pathology that you need to be familiar with there are sporadic cases and the opposite which is familial cases what is the difference sporadic means it happened to me out of the blue the disease does not run in my family my father does not have it my uncle does not have it mother does not have it Grandma does not have it cousins do not have it no one in the family has it and I'm the first one to get it it just happened suddenly out of the blue it happens sporadically contrast that with familial diseases meaning a disease that runs in the family and the genetic mutation will be passed down the generations most patients with ALS have the sporadic form about 10% of cases have the familial form there are many mutations associated with this disease one famous mutation is the C9 o f72 what the french toast does that even mean this Enigma code means that the problem is on chromosome 9 that's where the genetic mutation is and it's an open reading frame 72 this explains a big chunk of cases there is another one which is the super oxide dismutate or S o1 this is an enzyme mutation and this is a very high yield fact for board exams to help my students remember that ALS is associated with s o mutation I have a terrible and inappropriate pneumonic viewer discretion is advisable are you ready okay my dear student do you think that ALS is a benign disease or a terrible disease of course it's a terrible disease I mean it's upper motor neuron lesion and lower motor neural lesion and it's horrible it's terrible that's right so it's as if that the patient was metaphorically sodomized by Fate next the prevalence of ALS is about five cases per 100,000 population signs and symptoms and physical exam findings of ALS we have upper motor neural Legion and lower motor neuron Legion because I have upper motor neuron leion we have hyper hyper positive hypertonia and clonus Hyper reflexia and positive babinsky and I have lower motor neural Legion hypotonia or aonia no tone hypo reflexia or a reflexion and negative Bensky upper motor neural lesion pareses the muscles are stiff lower motor neural leion flaccid paralysis the muscles are soft upper motor neural leion can lead to loss of fine motor dexterity lower motor neurol lesion can lead to fasiculations including tongue fasiculations but there are some intact findings in ALS the extraocular muscle movement is fine the bowel function is intact bladder function is intact and notice that ALS is a purely motor disease not a sensory disease so the sensations are intact can a male patient with ALS have erections and ejaculations the answer is yes because these are autonomic functions and not somatic motor functions remember that the autonomic spinal nerves leave through the lateral horn cells not the interior horn cells see medicine makes so much sense once you understand what the french toast you're talking about one of the skeletal muscles in your body is the diaphragm so it can be affected in ALS leading to respiratory paralysis and respiratory insufficiency this is a restrictive lung disease is it extrinsic restrictive or intrinsic restrictive it is extrinsic restrictive lung disease to learn about the difference please refer to my pulmonology playlist these patients can have bulbar symptoms and pseudo bulbar symptoms what is the bulb the bulb is the brain stem okay the the brain stem has the origin of most of your cranial nerves it's the third the fourth the fifth the 6th the sth the eighth the ninth the 10th the 11th and the 12th cranial nerves basically all of the cranial nerves except the first two cranial nerves three to 12 leave the brain stem and what do they do they reach muscles and skin of the face and the neck so head and neck basically so symptoms that can happen when I destroy my brain stem include dysarthria and dysphasia this arthria cannot talk or cannot articulate dysphasia cannot swallow I told my students that bulbar symptoms are the three DS diplopia dysarthria dysphasia but in ALS usually there is no diplopia because the extraocular muscles are usually intact next because ALS can affect the brain especially the cerebral cortex which has executive function ALS patients can have diminished executive functions next inappropriate laughter or inappropriate crying these are the sudu bulbar symptoms so if you find yourself laughing at my dead jokes maybe just maybe you need to get yourself checked for ALS how can we diagnose ALS clinically as you see signs and symptoms electromyography there was an old song by DrJohn Baron and it went like this Amit trophic lateral sclerosis EMG will clinch the diagnosis loss of both upper and lower motor neurons etc etc etc super oxide dismutate gene mutation just a trace in this case this song has disappeared from the surface of the internet for an unknown reason MRI not to diagnose ALS but to rule out other conditions such as tumors such as multiple sclerosis Etc pulmonary function test for the respiratory paralysis this is an extrinsic restrictive lung disease genetic test testing to find the gene mutations these mutations Could Happen sporadically or in a familiar fashion treatment for the respiratory paralysis you have the BiPAP and respiratory support and physical therapy severe progressed cases might need ventilatory support riosol is a glutamate antagonist that can help some patients with ALS another drug is edaravone which decreases the physical deterioration seen in ALS for the spasticity because of upper motor neuron lesion you can give backlin you can give clonazepam you can give tanine what's the mechanism of action of backlin what's the mechanism of action of kazaan and what's the mechanism of action of tadine if you know the answer to these questions please comment below for the sudo bulbar symptoms such as the inappropriate laughter there are anti-depressants that might help dextran quinine can also help quiz time here is a question for you what is the differential diagnosis for ALS if you know the answer please comment below don't forget to take a look at my neuroanatomy playlist if you want to learn about Strokes mardio infarctions cardiac arrhythmias ards acute limb esmia hypothermia hyperthermia drowning and toxidromes download my emergency medicine high yields course at medosa perfectional is.
com my courses come with videos notes and cases to learn about neurosurgery cardiothoracic surgery trauma surgery orthopedic surgery gastrointestinal surgery pre-operative care postoperative care and more download my surgery high yield course to learn about the anti-epileptics anti-depressants antis psychotics antiparkinsonian agents the opioid the anesthetics the stimulants and the sedatives and hypnotics download my neuropharmacology course at medicosis perfect. com if you value what I do help me make more videos by supporting the channel go to buy meac coffee.





![Amyotrophic Lateral Sclerosis [ALS] | Mechanism of Neuron Death](https://img.youtube.com/vi/dLHS8XzGO6g/maxresdefault.jpg)