Thrombolytic (or fibrinolytic) agents are medications used to dissolve unwanted blood clots to restore blood flow. Unlike anticoagulants, which prevent the formation of blood clots, thrombolytics break them down. These drugs are often used in emergency situations where the clots must be dissolved quickly to reestablish perfusion to vital organs, such as during a heart attack, stroke, or pulmonary embolism.
Thrombolytic therapy may also be used when anticoagulants fail to prevent blood clotting. Coagulation is a physiological process that is critical for the control of bleeding. Blood loss is stopped by formation of blood clots that seal the breaks in blood vessels.
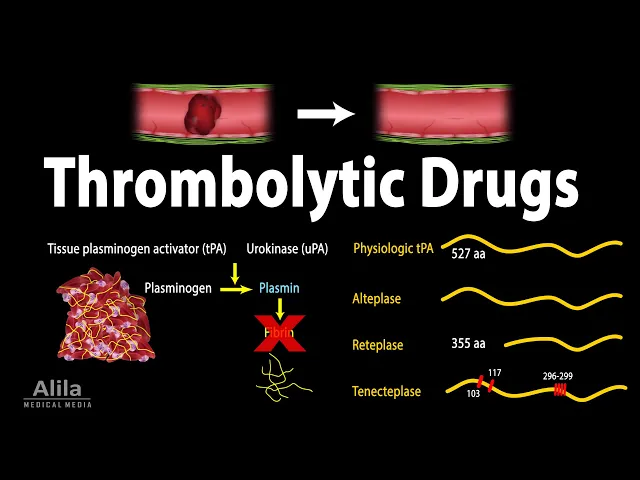
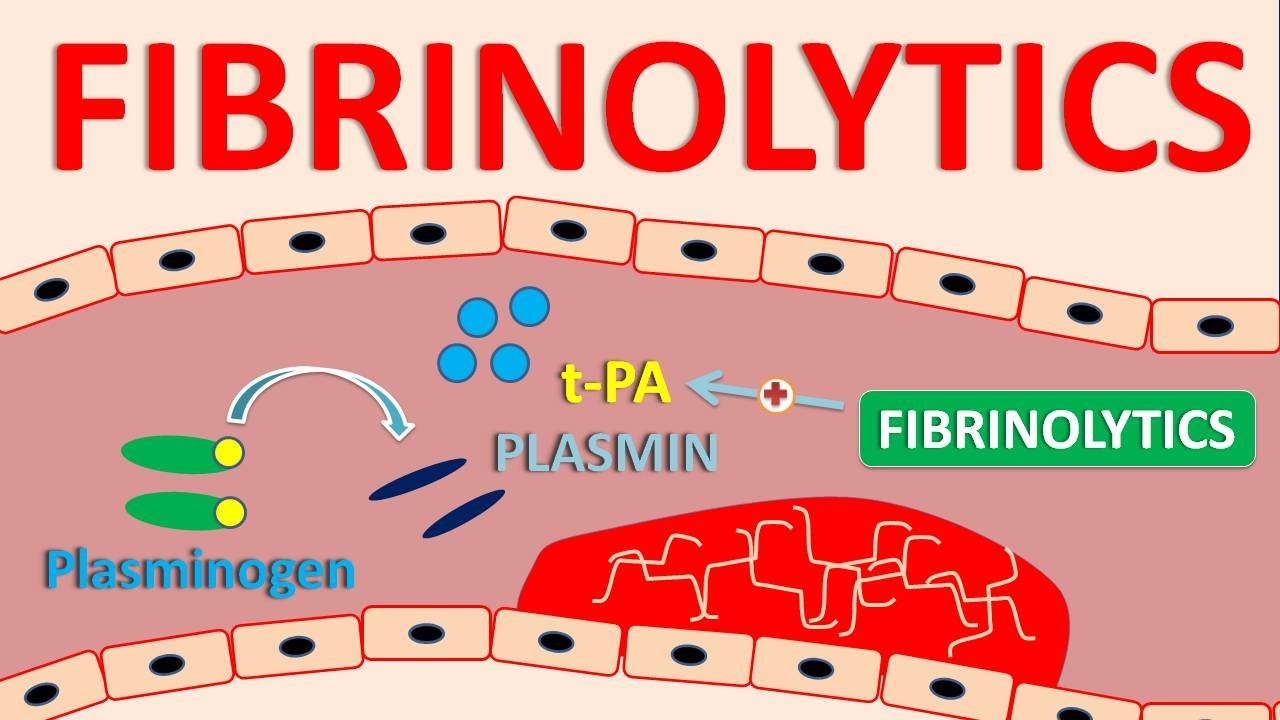
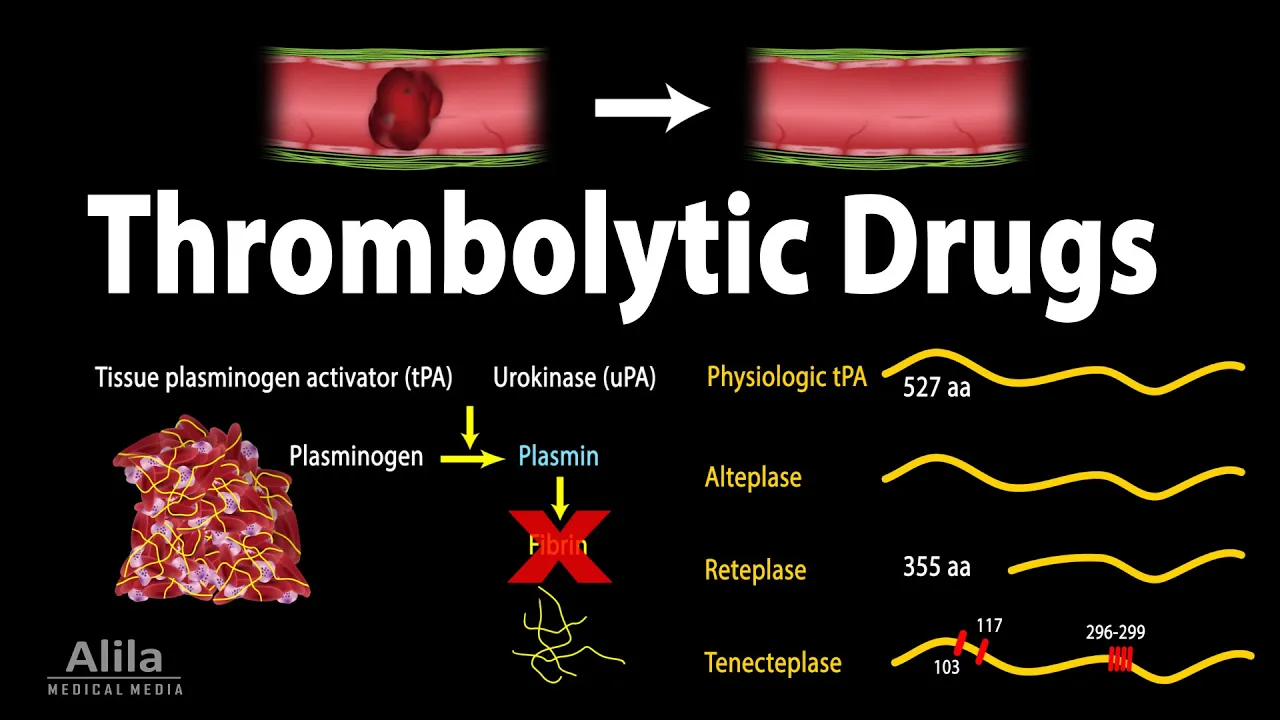
A clot is essentially a platelet plug reinforced with strands of the protein fibrin - the final product of the coagulation cascade. However, once the vessels are repaired and bleeding stops, blood clots must be dissolved to restore blood flow. In this process, called fibrinolysis, tissue plasminogen activator (tPA), and urokinase (uPA), convert plasminogen to plasmin; plasmin then cleaves fibrin and dissolves the clot.
Thrombolytic drugs are based on these plasminogen activators - they work by converting plasminogen to plasmin. There are 2 types of plasminogen activators: fibrin-specific and non–fibrin-specific: - Fibrin-specific agents require fibrin to function. They selectively act on fibrin-bound plasminogen within blood clots and have little or no effect on circulating plasminogen.
- Non–fibrin-specific agents, on the other hand, also act on circulating plasminogen to produce plasmin. Because plasmin can also cleave fibrinogen - the circulating precursor of fibrin, these agents are associated with a higher risk of systemic bleeding. Thrombolytic therapy can be administered intravenously, for a systemic delivery; or via a catheter to the site of blood clots, for a more localized action.
Alteplase is the first agent produced by recombinant technology and is identical to the physiologic tPA. It’s often the top choice for treatment of strokes, pulmonary embolism and cardiovascular events. Alteplase is not antigenic and may be re-administered as necessary.
Reteplase is a second-generation recombinant product, and is a shorter version of the physiologic tPA. This modification reduces its binding affinity for fibrin, enabling the drug to diffuse more easily through the clot. The result is a faster thrombolysis action and a lower bleeding risk.
Reteplase also has a longer half-life, which allows a more convenient bolus administration. Tenecteplase is another version of alteplase, with several amino acid substitutions. These changes lead to a higher fibrin specificity, hence lower bleeding risk, and a longer half-life, which allows a single-bolus administration.
Urokinase is a physiologic agent secreted by the kidneys. It can be purified from human urine, or produced from in vitro cell culture. Urokinase is a non–fibrin-specific agent and is most often used to treat peripheral vascular clots and occluded catheters.
Streptokinase, the first discovered thrombolytic, is produced by beta-hemolytic streptococci. It is an indirect plasminogen activator that must complex with plasminogen to become active. Streptokinase is non–fibrin-specific and is therefore associated with more bleeding complications.
In addition, because it’s a product of streptococcal bacteria, streptokinase is highly antigenic (hence cannot be re-administered safely) and often causes allergic reactions. Finally, there is anistreplase, which is a complex of streptokinase and plasminogen. It has some advantages over streptokinase but produces similar side effects.