hey it's medicos is perfection elsewhere medicine makes perfect sense in the previous video we have talked about purine metabolism and they'll talk about how to manage gout in my previous video on gout diagnosis I've asked you to question 6 & 7 the previous five questions or in this Rheumatology playlist is it possible to encounter an acute polyarticular gout I've told you before that gout is nono articular when it's acute can it be possible to have a q2 polyarticular also it's aspirin good or bad for gout let's enter the first one is it possible to incur
an acute polyarticular yes it's rare but yes such as what you can see it in myeloproliferative neoplasms such as polycythemia vera essential thrombocytosis and if you have watched my hematology playlist after that you can see hyperuricemia and even gout with the myeloproliferative neoplasms or with lymphoproliferative such as the leukemias long-standing gout can lead to acute polyarticular gout post organ transplants hyperuricemia and gout and chronic kidney disease because your kidney cannot excrete uric acid uric acid will accumulate to toxic levels leading to a huge polyarticular gout this Rheumatology playlist has more than 50 videos de novo
purine synthesis is here purine degradation is here salvage system is here here and here let's talk about degradation you have innocent will become high pose Anton I presenting can become xanthine thanks to xanthine oxidase famous enzyme xanthine can become uric acid by the same enzyme xanthine oxidase uric acid will end up in the urine let's say we would like to inhibit xanthine oxidase to inhibit the formation of uric acid so that we can manage gout you can use allopurinol or feedback so stet they will inhibit xanthine oxidase and as you see here X o is
ending oxidase and sted means to stop because the inhibit the xanthine oxidase these two drugs will prevent the formation of uric acid now once you have uric acid we have other options we can increase the of uric acids in the kidney so that we can get rid of the uric acid very quickly and there is a drug called proven acid or you can use high dose aspirin low dose aspirin will inhibit the excretion of uric acid in the kidney due to increased serum uric acid level but there is a problem with probenecid what's that when
you excrete lots of uric acid in the kidney there is an increased risk of uric acid kidney stones that's why patients who take probenecid usually have to drink more than four liters of water per day and that's why patients hate it and not many patients are unproven isn't gout is a crystalline arthropathy which is inflammatory arthritis caused by division of microscopic crystals into joints and other tissue could be acute or chronic could be out if the crystals are monosodium urate but if the crystals are calcium pyrophosphate dihydrate crystals recall the pseudogout if the crystals are
hydroxyapatite crystals we call this hydroxyapatite arthropathy also known as pseudo pseudo gout gout is an inflammatory arthritis affects the first metatarsal phalangeal joint it could be acute it could be chronic it's asymmetrical usually mono articular peripheral and it's not an autoimmune disease gout is a crystalline inflammatory asymmetrical mono arthritis that involves small peripheral joints specially a big toe due to the position of microscopic crystals monosodium urate crystals and it's more common in males than females hyperuricemia is not the same thing as gout and we have talked about the slide in a previous video gout is
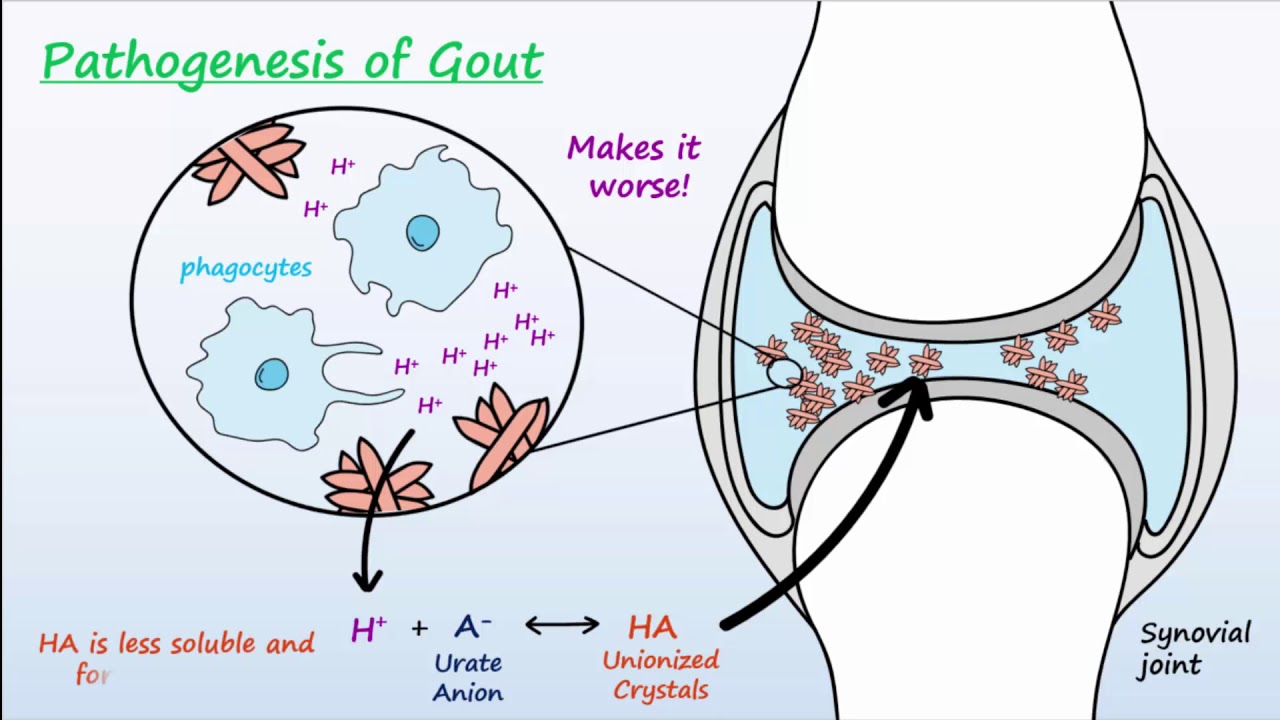
more common in middle-aged men associated with meat seafood and beer uncontrolled hypertension and diabetes are risk factors it's an inflammatory freakin arthritis what's the next step always aspired the joint why number one to rule out septic arthritis which is infection and number two is to diagnose the freaking out why should i like rule out septic arthritis because it's a freakin emergency and one of the management modalities for gout is to give intra-articular steroids or systemic steroids will suppress your immune system if this is an infection and you misdiagnosed it as gout and you gave patient
steroids good job doctor this is stupidity on steroids wink-wink risk factors of gout were discussed before please don't forget hypertension and meat fat seafood soft drinks fructose glucose etc uric acid is less common in women because estrogen is protective its Yuriko suruc it excrete uric acid in the kidney gelt could be primary or secondary what's the problem of primary it's an inborn error of metabolism so flesh such as Latian eye hand syndrome deficiency of h g PR taste enzyme we have talked about this in my previous video called purine metabolism it could be secondary which
is more common than primary secondary could be due to over production of uric acid or under excretion of uric acid under excretion is more common than overproduction over production sirs increased cell turnover eating lots of meat and beer alters under excretion nephropathy let poisoning and drugs such as diuretics loop and thiazide low dose aspirin high dose niacin pyrazine amide and chemotherapeutic agents since tumor lysis syndrome can lead to hyperuricemia and gout the drugs that are used to manage chronic gout are the same freakin drugs that will manage tumor lysis syndrome acute gout is the pain
usually very severe pain could be 10 out of 10 the big toe we call this food agra but quranic gout is the toe finer the pedigree the toe fie the out can lead to five different conditions you could be asymptomatic with high uric acid you could have acute or thrice this is very painful interr'd critical periods chronic to fascia Scout or uric acid in the properties these are kidney stones as you know uric acid kidney stones happen if your urine is acidic an acidic environment also uric acid kidney stones are radio loosened uric acid has
a you radio loosened has another you what do you mean by radiolucent you cannot see them on x-ray so how can i diagnose it renal ultrasound Bailey the diagnosis of Gao to us discussed before please don't forget arthrocentesis with joint fluid analysis and if the patient has gout you'll find all of this on arthrocentesis for arthrocentesis to be diagnostic you nearthe least one intracellular monosodium urate what do you mean dosa inside the freaky neutrals over more than or equal three extrasolar monosodium urate crystals in the joint gaudi crystals AKA monosodium urate crystals are negatively birefringence
crystals birefringence was discussed in a previous video it was a great lecture in physics gaudí crystals negative birefringence pseudogout positive birefringence grouchy crystals are needle shaped pseudogout a rhomboid shaped ipod uremia is not the same as gal just because you have hyperuricemia does not necessarily mean that you will suffer from a gout attack there is no correlation between serum or gas level an acute gouty arthritis oftentimes uragan acute attack serum uric acid may be normal or even low what does high plasma gas mean it means that you are at risk it does not confirm the
diagnosis now let's talk about treatment of gout we have treatment of the acute attack which is entirely different from treatment of the chronic attack treatment of acute exacerbation becomes 10 out of 10 doctor it's severe pains the worst pain of my life so their treatment is gonna be pain medications mostly cool chronic gout this is a patient whose chronic so the purpose of the treatment is to prevent future acute attack so this is prophylaxis and this aims at decreasing uric acid should oil decrease uric acid during the acute attack oh shut up if you decrease
uric acid during an acute attack you might worsen the attack you only decrease it when the patient has no pain because no pain no gain also even in chronic gout when you try to decrease uric acid don't decrease it too much too rapidly if you're that you can precipitate an acute gouty arthritis attack Sriman of gout baby you can treat the acute gouty attacks and this has nothing to do with the chronic chronic gout computer attacks non-steroidal anti-inflammatory drugs because goat isn't freaking inflammation steroids because gout is a freakin inflammation and colchicine gout we try
to decrease production of uric acid and increase excretion of uric acid remember that uric acid patients are either over producers or under X critters so you do the opposite to treat it I have a premium cardiac form ecology chorus on my website médicos is perfectionist calm has 50 videos and it has a great discount till the end of April treatment of gout acute and chronic acute nonsteroidals steroids and colchicine these are pain medications they are also anti-inflammatory some people are trying to use interleukin 1 inhibitors such as anakinra and kanaky nehemiah to treat gout we'll
see if it works chronic gout decreased production or increase how do I decrease production diet and lifestyle modification decrease your intake of meat beer seafood try to lose weight try to manage your bad hypertension increase excretion how do I do it we use you rate lowering therapy I love it so she has xanthine oxidase inhibitors allopurinol and Phivolcs so stat xanthine oxidase inhibitor Yuriko suruc agents which will excrete uric acid in the urine and your case that's an enzyme uric ace it's an enzyme that will destroy uric acid and degraded and you have two options
respira case and take galata case who named these things treatment of acute gout let's focus on acute i spects because of spain an inflammation non-steroidal such as indomethacin or silicon said this is a non-selective cox inhibitor this is a selective cox-2 inhibitors i have talked about the difference between cox-1 and cox-2 in a great video in my bleeding and coagulation playlist indomethacin if you have multiple joints and Silcox of also if you have multiple joints and history of peptic ulcer disease because this is soft and smooth on your stomach because it's only - not coxswain
steroidal first you will add the freaking infection that's why we do the are throw flipping synthesis prednisone or methyl pernessa know your options should I give them into articular or systemic you can do either colchicine if the patient has multiple joints please use low dose colchicine if your professor is an old dinosaur who has not opened textbook sense man walked in moon he is used to giving hide those cultures he even intravenous colchicine no more colchicine can be really toxic speaking of toxic here are the adverse effects of colchicine nausea vomiting in myopathy bone marrow
suppression especially in chronic kidney disease and usually patients with gout have chronic kidney disease that's why they have kept or you say that all patients are not all gout patients but some of them okay contraindications do not use colchicine with drugs that inhibit cyclic roam p450 three a four especially in chronic kidney disease because this will increase the toxicity of colchicine and you can end up with neutropenia and infections stream of chronic gout either decreased production or you increase excretion treatment of chronic gout general rules decrease production will this work sometimes but most of the
time at best it will decrease uric acid by one milligram for this liter only this is not good also if my doctor rolled up on me and said hey medical says you should not eat seafood I will use my l3 and l4 segment to initiate a knee-jerk reaction to kick him in the pudendal nerve it ain't gonna happen baby and that's why adherence with this regimen is easier said than done increased excretion do not start these drugs until the acute attack subsides otherwise you might make it worse regarding decreased production patients should decrease intake of
processed simple sugar such as raw sugar brown sugar corn syrup fructose glucose and sucrose patients should instead of this consume complex not simple but complex carbohydrates such as fruits vegetables and nuts which are close to the pudendal nerve if you know what I'm saying here are some tips for chronic management of gout you should not start it during an acute attack you should wait until the patient has no pain the goal is the decrease in serum uric acid level below 6 if the patient has severe gaped how do I note severe your toe fie there
are severe symptoms decrease it the uric acid less than 5 milligrams per deciliter in the serum so your rate law drugs what's the goal to decrease your gas at less than six and this is below the saturation point for uric acid this is sophisticated stuff indications when should I use urate lowering therapy of the business to fiery stones or urine you rate more than 1100 milligrams per deciliter or if the patient has recurrent attacks which is defined as more than one attack per year what are the options Anton oxidase inhibitors Eureka Surak agents and gearcase
xanthine oxidase inhibitors are the most commonly used nowadays but these and we can use them in over producers or under X creatures allopurinol baby very cheap very effective xanthine oxidase inhibitor is the mechanism of action the clinical uses are chronic gout hyperuricemia tumor lysis syndrome myeloproliferative neoplasms because they can have gout in hyperuricemia so it affects nausea vomiting diarrhea ah happens with many drugs rash hypersensitivity reactions this is a big deal such as Steven Johnson syndrome toxic epidermal necrolysis and dress syndrome drug-related you seen Ophelia with systemic symptoms in Steven Johnson syndrome and toxic epidermal
necrolysis the patient can have fever blisters vesicles and bull a rash diffuse erythema which is ill-defined contrast that with every syphilis which is very well demarcated the rash can also lead to extensive necrosis as well as acute kidney injury which was previously known as acute kidney failure but since we live in the era of snowflakes and people don't like failure and everyone is a winner we changed the name into injury instead of failure in order not to hurt your feelings I think I'm a stupid idiot with ever purine overdose has to be adjusted for GFR
okay drug drug interactions normally by the way is a thigh brain and six milk after purine one is a prodrug to the other are metabolized using Benteen oxidase now imagine that you gave our peer know which is a xanthine oxidase inhibitor no one is gonna degrade Asaph - or six more kept appearing so if you give allopurinol plus ssi print or LPR on +6 mcafee purine and now there is no xanthine oxidase this will increase the toxicity of azo fibrin and six mercaptan these are chemo therapeutic agents side effects include Milo suppression what is the
solution decrease the dose of is a thigh friend or six more captive hearing if you decide to give them with LP or no by about seventy percent free box usted I have good news and bad news good news there is no need to adjust the dose based on the GFR kill bad news it's more expensive than LP Renault xanthine oxidase inhibitor is the mechanism action medical uses include chronic gout hyperuricemia tumor lysis syndrome and mother professor neoplasms nausea from degrees and a high percentage reaction by the way if a patient has a history of an
LP r''l induced hypersensitive reaction you should not give feedback so sad because usually they will get the same reaction with few extra stairs again the same drug drug interaction applies because Phivolcs are said you know it inhibits the xanthine oxidase your rate lowering drugs Anton oxidase inhibitors Yuriko suruc agents and your case let me tell you about your case what's uric ace ace is an enzyme it's an enzyme that degrades uric acid some birds have it some other organisms have it but humans do not have it and that's why we can give humans uric a
such as respiration piggle OT case they will damage and degrade they recast it into some trash these are degradation products soluble and towing and if you remember in brie ology this can make sense this is close to the kidney we use res very case for tumor lysis syndrome few doctors use it for gout piccolo decades is definitely used for gout and of course tumor listen why do we go to pick a lot a case because it's a pegylated recombinant in the middlee in your case i love it side-effect hemolysis in patients with g6pd deficiency therefore
before you prescribe big logic haze please check the g6pd level first and of course you know we always check the level of this enzyme during quranic period not during the acute hemolytic attack it will be falsely elevated and you know if a patient is fine there is no g6pd deficiency oh shut up also watch my video on g6pd deficiency because it was epic I'm an Egyptian guy so I know what I'm talking about Yuriko Zurich agents / Boehner said work inhibits you are 81 which is you're a transporter one this will lead to increase kidney
clearance of uric acid and the side effects Eirik acid kidney sauce because you're increasing the secretion of uric acid in the urine so patients usually have to drink more than one gallon of water today contraindications do not give probenecid if the patient has a history of kidney stones low GFR high creatinine Toph I or if they are over producers because this is not the problem these are not under excrete or these are over producers now is aspirin good or bad for I tell you that remember that a rapid increase or decrease in serum uric acid
level can precipitate the acute attacks take it nice and easy doctor so is esperan girl bad or depends low dose aspirin is anti platelets it's actually bad for gout high dose is the anti-inflammatory and since gout is a freakin inflammatory arthritis high dose aspirin can be good because it's a Yuriko suruc at high dose it inhibits uric acid secretion at a low dose thank you so much for watching don't forget subscribe hit the bell and click on the join button you can support me here or here get my cardiac forum ecology course at medical suspicion
a less calm thank you so much for watching as always be safe stay happy and study hard this is medicos perfect snails where medicine makes perfect sense