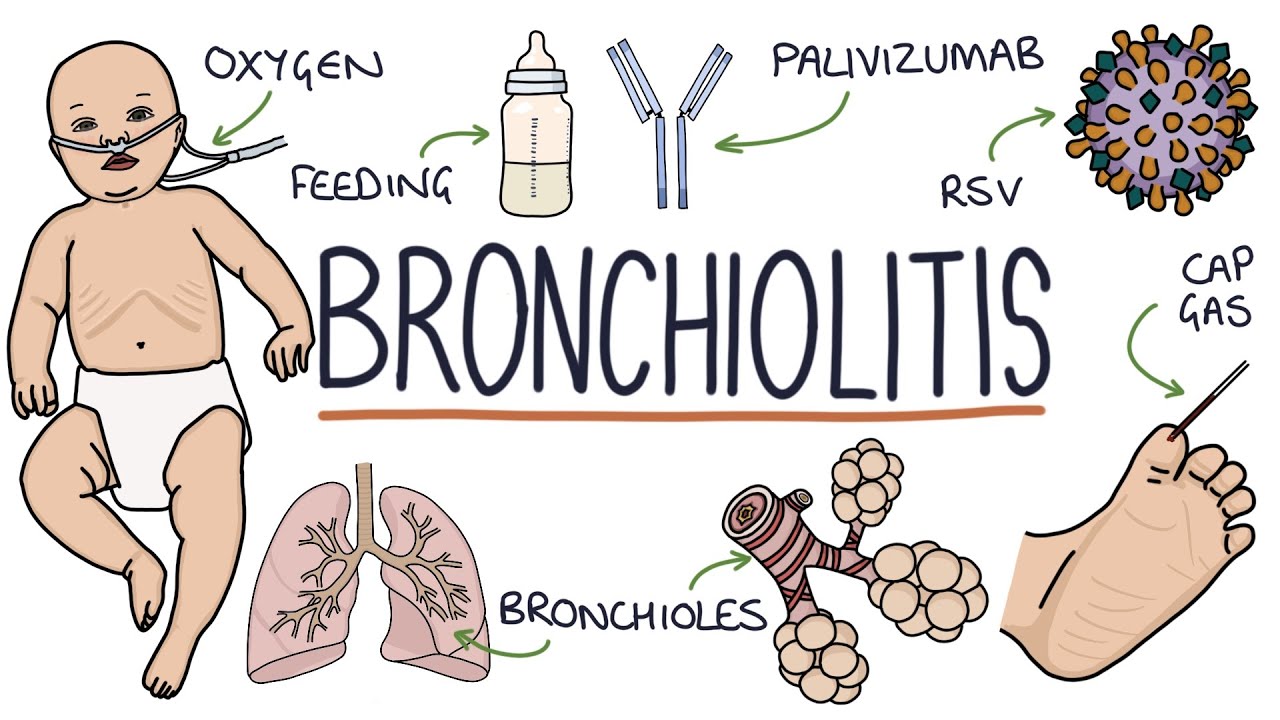
welcome to pete's doc talk tv i am dr mona amin a board-certified pediatrician and mom and it has been four months since i released a new episode here on pete's talk talk tv and it feels so good to be back i am talking all about bronchiolitis rsv what it is what are the symptoms and what to do about it this video is brought to you by the new mom survival guide an online digital e-course created by me to educate empower and create community for mothers as they embark on their journey for more information click the
link in the caption before we continue make sure you hit that subscribe button because that's how you stay up to date on all of the videos i will be releasing here on feedstock talk tv and here we go bronchiolitis is an infection that causes the small tubes of the lungs the bronchioles to get inflamed or swollen this makes it harder for babies to breathe it is more common in infants or younger children under two because of their smaller airways bronchiolitis is different than bronchitis bronchitis is something that we see in adults but children especially children
under two rarely or never get bronchitis bronchiolitis commonly gets referred to as rsv rsv is the respiratory syncytial virus it is one of the viruses that can cause bronchiolitis but in actuality bronchiolitis is a medical condition that can be caused by multiple viruses things like the flu things like rhinovirus things like enterovirus can all cause bronchiolitis it's just that rsv is one of the most common viruses that do cause this condition rsv is notorious for causing bronchiolitis because rsv causes a lot of congestion that congestion causes a lot of mucus which causes a lot of
inflammation that can affect the bronchioles leading to bronchiolitis rsv in adults can seem like a very bad cold with a lot of congestion and maybe a cough but in children especially infants and toddlers under two it can cause difficulty breathing and wheezing in some instances the younger of the child the more concerned we are going to be with rsv and bronchiolitis this has to do with their anatomy and the size of their airways if an adult gets rsv they're likely going to be okay because their airway including the bronchials are much larger but a baby
and a toddler can have a harder time clearing that mucus and subsequently can lead to the complications of bronchiolitis a typical rsv season runs from late fall to winter with a peak usually in february interestingly enough states like florida see their peak much earlier so their rsv season ends by november but because of the coven 19 pandemic we are seeing shifts in the season of rsv notably we were seeing a lot of cases in the summer all around the country when it is unseasonable for rsv to be so high so i wanted to create this
video so that you are aware of the symptoms when you need to seek medical attention and what you can do at home to manage the symptoms bronchiolitis is a pretty classic presentation it can start like a common cold that looks like a runny nose or stuffy nose with or without fever by day two or three the child is going to have shortness of breath difficulty breathing and their cough may seem to be getting worse think of it as a cold that has gone deeper into the chest it's not a bacterial process that likely needs antibiotics
but it's a virus that has caused so much congestion and subsequently inflammation that it's impacting the bronchioles or the small tubes of the lungs now remember signs of distress in your child may not always be rsv bronchiolitis but i wanted to go over what a child with bronchiolitis can look like on day two or three when you look at this video you can see the child's chest moving in and out this is not a normal breathing pattern you can see that they're sort of labored in their breathing tugging in and out you may also see
nasal flaring where the nostrils are flaring in and out this is much different than their normal breathing pattern watch your child's rib cage and if you're noticing the tugging that goes in and out if you watch here at the top of their sternum and you see tugging in and out or nasal flaring you would want to get your child evaluated to make sure a clinician can listen to their chest and see if they need any additional therapy other signs can be grunting with this difficulty breathing high pitched whistling sounds that almost sound like a wheeze
when they breathe out difficulty drinking remember that if they're having difficulty breathing they may have a hard time drinking because in order to drink comfortably you have to be breathing comfortably when i listen to the chest of a child with bronchiolitis it sounds like a washing machine i listen with my stethoscope and i can just hear mucus shrilling around it's something that we hear commonly that is also called ronkai you may also hear wheezing if we were to listen with the stethoscope your child may also have grunting sounds but remember grunting sounds alone are not
always a cause for concern but if it's grunting with difficulty breathing those ribs tugging in and out the sternum right here tugging in and out the nostrils flaring in and out you're going to want to get your child evaluated remember we as adults can get rsv we can get many of the viruses that can cause bronchiolitis but the difference is in children these viruses can cause more difficulty breathing because of the smaller airways symptoms can appear anywhere from two to eight days after initial exposure the duration of symptoms can vary child by child i want
you to watch out for that day two to three where we do see that difficulty breathing start to peak if you're noticing that difficulty breathing on day two or 3 or even to day 4 of illness you definitely want to seek medical attention rsv is spread by person-to-person contact or touching shared services similar to any respiratory virus that we see in our community you can return to school or daycare once your child is fever-free without any medicine that includes tylenol or motrin they are not needing any therapies such as albuterol such as saline which we'll
go over and they're back to their normal spirits this means eating drinking pretty much close to baseline how i describe it is that if your child is comfortable enough for you to be taking care of them then they can go be taken care of by someone else but they also have to be fever-free for 24 hours without any medicines to mask a fever typically rsv is diagnosed by clinical presentation that child who has congestion maybe a cough may be a fever and day two to three is now presenting with difficulty breathing at some hospitals or
urgent cares they will be able to swab your child they'll stick a little swab into their nose to say that hey this is actually rsv this is not necessary to make the diagnosis as a fyi a lot of this is done in hospitals for cohorting for example if your child is sick and needs to be admitted they will swap the child not because it's really going to change management but because we need to know in a hospital setting that this child has rsv so that when they are placed in certain rooms or certain parts of
the hospital that they can say that this child has rsv this child has rsv so that the staff is aware of what viruses are existing in which rooms but if your child's pediatrician in the outpatient office is not swapping them for rsv i don't want you to feel like they're not doing a full thorough workup the clinical picture can tell us a lot about what's happening and we often do not need that swap to tell us that clinically this looks like bronchiolitis could it be one of the other viruses that cause bronchiolitis besides rsv sure
but the management would stay the same if the child has any difficulty breathing if the child has any therapies that are needed so having the diagnosis really doesn't change our management because we're going to be taking care of it the same way if your child is sent home with bronchiolitis you're going to monitor their breathing difficulty their hydration you're going to monitor for persistent fever if anything changes or you are concerned seek medical attention please watch my videos on cough and cold symptoms and fever 101 for more information on how you can help with symptoms
things like saline in the nose things like baby vicks rub for children under two things like a humidifier can really help in terms of those congestion symptoms but with bronchiolitis we want to keep a close eye on their breathing and their hydration to make sure we don't need to add anything else for them but if your child is dehydrated which means that they're making less tears they're not making as much wet diapers they seem fragile or listless you're going to want to seek medical attention for that dehydration the other big thing is difficulty breathing which
i mentioned was those retractions that you see in the rib cage retractions that you see here and nasal flaring that you may see in the nose the other reason we want to see the child is fever persistence or just overall inconsolability despite meds so even if your child is acting okay in terms of how they're breathing and their hydration is okay if they are seeming very inconsolable with that fever motrin or tylenol depending on their age is not helping we want to see your child to make sure they don't have an ear infection to make
sure that we listen to their chest to make sure no other intervention is needed for the well-being of your child if your child is dehydrated you may need to go to the emergency room there they may give your child iv fluids iv fluids is when they set up an iv and give fluids through that line to hydrate your child in some cases they need that to perk them up so they can breathe more comfortably in other situations if your child is having severe difficulty breathing looking dehydrated your child may be admitted for observation to make
sure that their breathing status improves and to make sure that their hydration status improves if your child is having difficulty breathing you can go to the er or your child's clinician's office however if your child is very listless and having very low energy your best bet would be to go to the emergency room because they will evaluate if your child needs iv fluids and if they need any support for oxygen or any support for their breathing your child's clinician's office if they're open can guide you there may be chances that you go to the office
they look at you and then they have to send you to the er this is obviously for the best interest of your child so you can always call your nursing line and see what the best step is based on your child's symptoms if you need to go to the office or if you need to go to the er but how i say it is if you're looking at your child and they seem very labored in their breathing they're not drinking anything they're just very uncomfortable it may be beneficial to go to the er to see
what the evaluation is and you may be admitted or you may just be able to go home with certain medicines or interventions if your child is mildly labored meaning that they're comfortable but you see some tugging in their chest they're hydrated their oxygen saturations are normal their fever is there but it's controllable with medicines and their comfort is there your child's clinician may just recommend nasal suctioning which helps alleviate that mucus from the nose they may recommend a humidifier these are things that we would do for any child with a coffin cold with close observation
of their breathing difficulty and their level of hydration in more moderate to severe cases of difficulty breathing the management will depend on the child's work of breathing how fast they're breathing and also their oxygen status in a child who's not really working hard to breathe but has a lower oxygen they may just recommend oxygen via something called a nasal cannula this is something that goes into the nose and helps deliver oxygen to support their lungs in cases where the child is having a lot of difficulty breathing there may be other interventions these are things in
the hospital like something called a cpap machine and in very severe cases it may be something called intubation intubation is where a breathing tube is placed to support the child while they recover remember bronchiolitis is usually caused by a viral process rsv is a virus so there's no antibiotic that is needed but we need to support the child so their body can heal itself so things like intubation things like oxygen these are things to support the child so that their body can heal from this virus and that you all can go home in some cases
some doctors still do prescribe steroids it is not usually recommended to prescribe steroids in bronchiolitis the guidelines have now changed that really is supportive care its hydration iv fluids its oxygen support and breathing support if needed some doctors still do prescribed steroids and this may just be a case-by-case basis based on the symptoms some clinicians still do prescribe albuterol albuterol is typically used for asthmatics and rsv is different than asthma but sometimes we do see that the albuterol treatments can help so it's really up to your child's clinician to discuss with you what are the
options based on your child's symptoms and what's going on in the office another possibility is something called nebulized saline saline can be administered through a nebulizer machine and can in many ways help break up that mucus this is also another treatment that your child's clinician may recommend overall the supportive care is what we need we need to make sure that your child is staying hydrated we need to make sure that their breathing is comfortable so many times in bronchiolitis if your child is being sent home from the clinician's office they may recommend coming every day
or every other day to follow up your child's clinical status if you go to the hospital and your child needs admission rest assured the reason for this admission is to monitor all the things i mentioned how's your child breathing do they need any other support do they need anything for iv fluids or hydration sometimes being in the hospital can be the best thing for your child so that they can recover i know as a mom that it can be very scary when your child is admitted to a hospital but sometimes it can be the best
place for their body to heal over 50 000 children get admitted to the hospital with bronchiolitis every year last year 2020 was a little lower because of the pandemic and the precautions that we had but know that it is common and outcomes are good in terms of what we're monitoring and what we have to do but sometimes your child has to be in the best place possible and that may be the hospital the best prevention for rsv and bronchiolitis and all of the other viruses that can cause this are the same things we would do
for any respiratory virus things like hand washing things like covering our nose and our mouth when we sneeze and washing our hands things like limiting visitors especially to our newborns and our premature babies if you must have visitors you can have them wear a mask or assure that no one is under the weather i know everyone wants to see newborn babies but if they're not feeling well if they're under the weather they should hold off on that visitation if that visitation needs to happen because it's you or your partner or someone who's taking care of
your baby mask them remember masks help prevent against the spread of respiratory illnesses including rsv for older siblings that may be in child care they can still go to child care you can weigh the benefit and risk with that situation with your child's clinician but if they do go a habit that you can get into is having them kiss baby's feet focus on showing affection to the feet versus getting into the face this can help protect the baby's mucous membranes from getting infected with rsv or other viruses that may be circulating right now another tip
is to avoid utensils if sick i know this can be really hard when we are with our children but this is a simple way that we can avoid germs spreading in our home currently there are no vaccines against rsv but science is awesome and there are currently trials to create a rsv vaccine for children although there is not a vaccine for some high risk infants there is something called synergists which is humanized monoclonal antibody that can help reduce a high risk infant's risk of getting rsv and getting complications from rsv this therapy is recommended in
up to five months during rsv season for high risk infants eligible children include premature infants especially those born at less than 29 weeks gestation infants with chronic lung disease of prematurity infants with certain types of hemodynamically significant congenital heart disease infants and young children with certain immunodeficiency states and infants with pulmonary abnormalities or neurological and neuromuscular conditions that impair their ability to clear secretions from their upper airway remember rsv is one of the many viruses that cause bronchiolitis but we do end up calling it the same thing remember that other viruses can cause bronchiolitis and
always remember what to look out for that difficulty breathing the dehydration all of the things that we would want you to look out for for every virus the best way that we can prevent the spread of rsv is hand hygiene the same things that we're doing in this pandemic but really remembering to always protect our youngest children bronchiolitis affects children usually under two years of age more so because their size of their airways so when we are taking precautions we want to do the best we can to reduce the risk with the understanding that we
do the best that we can thank you for joining me today if you found this video helpful make sure you comment below share it on social media and ask any questions if you have them and i'll see you next week