today we're going to talk about the neuros pych cric aspects of traumatic brain injury with hopes that I can highlight that this is a very challenging clinical population with distinct Diagnostic and assessment dilemas at the end of this talk we're hoping that everyone can describe common neuros psychiatric disturbances after TBI review clinical and demographic risk factors and recognize psychosocial and pharmacological interventions that we often use to treat patients with these symptoms I'll touch briefly on the epidemiology and then we'll talk about some of the cohort studies we've done here at Hopkins to better conceptualize understanding
these patients we'll pivot over to talking about management and then we'll wrap up talking about where this field is headed in the future directions of TBI and Psychiatry so first we have to start off talking about why is it important what is TBI and what did we know about TBI what's been studied so far best place to start is always with the definition what is a traumatic brain injury so there are various classification systems the acrm vadod uh the CDC uh various classification systems that have different definitions of criteria that actually consider a diagnosis of
TBI but the most important point is that TBI is a clinical diagnosis there is a presence of symptomatology that has to be there in order for it to be considered a TBI it could be one of three of the following the first is loss of consciousness this is where we asked the patient did you black out second is loss of memory do you remember things before or after the accident third is altered mental state where you days disoriented confused as you heard today that happened after a car accident so you have to have at least
one of these three symptoms in order to be considered a TBI even though there's no standardized definition most people kind of rely on this it has to have some traumatically induced physiological disruption of the brain which means it's coming from the outside there has to be some trauma to the skull that happens causing these symptoms to occur now you may or may not have focal neurological deficits and your head Imaging may or may not be normal but again a head injury is not always a brain injury so the presence of these symptoms is really important
as we'll talk a lot about today TBI is a big public health problem huge about 3.6 million tbis occur in the us annually and about 3.2 to 5.3 million people suffer with some TBI related disability it's also a very expensive disease if you're looking at people who are discharged from the ICU people who are discharged from the ER with concussions people who are going to rehabs we're looking at anywhere from 60 to $221 million in direct and indirect costs and as we'll explore today at least 43% of patients have some kind of functional or Neuropsychiatric
sequele that happen afterwards it's important to understand the the mechanism of injury so when a patient comes to you with the TBI important to ask how they got that TBI so with a growing geriatric population we're seeing a lot of people who are suffering from Falls so Falls is typically usually what we see coming into the ER this is followed by motor vehicle accidents and assaults particularly here in Baltimore very commonly a reason that we see people coming in with injuries this group of quote other are people who are kind of now getting more media
attension people who are getting repeat concussions due to sports related injuries or blast injuries due to being in active combat why do we as psychiatrists need to know about TBI why is it important in the psychiatric Community to understand this well the answer to that is three-fold the first is there are distinct neuros psychiatric phenomena that we see that you don't normally see in idiopathic psychiatric disorders like major depression or bipolar disorder and because it's distinct Neuropsychiatric phenomena many of these patients are or refractory to treatment so you may not see a patient respond to
an SSRI like they normally would with major depression as they would if they had depression after TBI and finally as we'll talk about there is a distinct Nuance of emotional and behavioral discont control that is present in these patients that may or may not be comorbid with the mood disorder but makes treatment even more challenging when we see these patients if we think about the tvi like this devastating occurrence that occurs with the patient and the patient may or may not have had some kind of Neuropsychiatric problems before compounded together it creates a significant amount
of disability we see problems with social integration Workforce participation we see issues with occupational activities and overall ADLs and functioning if you think about Neuropsychiatric disturbances after TBI you can kind of put them into four big buckets there's the emotional piece there's the cognitive piece there's the behavioral piece but you also don't want to ignore physical problems because if someone got hit in the head very likely their body was injured as well but the most important thing to remember is how well a patient does after a TBI depends on what happened before the injury at
the time of the injury and after the injury a lot of cohort studies and researchers in the field have try to conceptualize this connection between psychiatric disorders and traumatic brain injury but the problem is a lot of this is using a syndrome focused approach so this is a study that was done last year um by howlet at l in 2022 looking at overall axis one diagnosis and TBI in the trajectories over the past 5 years the top line is sort of all axis one diagnosis and then they break it down into mood disorders substance use
anxiety Etc you can see the blue line is mood disorders and more commonly this is what we see often in TBI mood disorders are the most prevalent after TBI and over time as you see with this trajectory things get better so from compared to one year at 5 years symptoms have pretty much or the syndromes have gotten better but this is not what we're seeing in clinic and this is today was a perfect example of that even several years after an injury we have patients saying I'm not getting better I'm actually getting worse so what
does that mean that leads us to the question of is there a noic issue going on is it not that we should be looking at syndromes but rather we should be looking at symptoms so the first is that there's a distinct phenomena of discont control that we see in these patients and when you look at discont control we can kind of break them down into three pieces the first being emotional so affective instability momentto moment shifts in mood and sort of being happy one minute angry the next minute pathological laughter and crying this is where
we see uncontrollable periods of laughter or crying in response to trivial stimuli an example of this is a patient of mine who started crying after she watched a gum commercial or irritability being on edge short and quick to anger behavioral problems are also something you want to think about so aggression or agitation we often see sometimes patients can be disinhibited blurting things out at the family table or becoming sexually inappropriate and then there's that third piece of cognition where we're often seeing patients struggling with slow processing speed with verbal learning issues difficulty initiating and completing
tasks so combined together this is sort of this phenomena of discont control that we really want to be thinking about when we're formulating these patients so this kind of prompted us to ask the question how can we study these patients better and what can we do to identify Neuropsychiatric correlates so let's talk now about some of the earlier studies we did these are some of the studies we did when I was starting off in my career with my wonderful Mentor Dr Ral and we asked the question could we look at these non-traditional symptom scales of
these Nuance symptoms in tbii and see if there is any correlation with mood disorders so what we did was we looked at over aggression pathological laughter and crying social functioning and then we looked at whether or not there was a correlation to scores on specific mood and anxiety scales so this is a group of patients that were first time TBI so no prior history of TBI that were admitted to the rehab units either at jhh or Kernan we lost about 39 to follow up and we ended up analyzing about 103 participants so the first point
is that the the timeline was as such they had to have blunt head trauma so no penetrating injuries no skull fractures and they admitted to the rehab so these are more chronic patients and we were we were basically doing these instruments at 3 6 and 12 months and what we found when we looked at sort of clinical variables is that the most common um gender or sex was 62.1 was male so majority of these patients were male that suffered the TBI the second was that the most common form of injury were motor vehicle accidents and
the third is that the most common severity of tbii was mild TBI now when we looked at new onet depression so these are patients who had no prior psychiatric history before but developed depressive symptoms after the TBI we found that there were higher prevalences of new onet depression in the first 3 months after injury but interestingly the presence of poor social functioning early on predicted the development of new onset depression even 12 months out we also then looked at different typ of aggression so the the overt aggression scale looks at verbal aggression physical aggression to
self others and objects what we found is that the most common type of aggression was verbal but interestingly if there was decreased social functioning early on and and the presence of new onet depression early on this was actually associated with verbal aggression later on at 12 months we looked at pathological laughter and crying using the pathological laughter and crying scale this is very highly validated in the stroke population and we also use it quite often in TBI when you parse out each symptom we found out across the board at each time Point pathological laughter was
much more common and the folks that were experiencing the most symptoms of pathological laughter and crying were those with mild TBI then if you look at across time points the pathological laughter and crying and you compare those that had it we call it plaque those who had plaque versus those that didn't those that ended up having plaque across time points had higher scores on the hamd as well as the clinical anxiety score SC so this association with plaque and mood disorders was quite evident in this particular cohort so what did we learn from this kand
study firstly males were injured more than females early mood symptoms were associated with aggression later on mood symptoms were also correlated or coexisting with pathological laughter and crying and the most common type of TBI severity was mild TBI so why is it what's so important about mild TBI you heard a little bit about it today and why is it so important to me in terms of my career and my um trajectory I've spent the last several years of my career really focusing on this patient population for several reasons the first is this is the most
common severity of TBI about 70 to 90% you've already seen from our study and in the literature very commonly if a patient has TBI it's likely going to be mild these symptoms are often overlooked by by doctors all the time patients are discharged from the ER and told to walk it off you'll get better and really they're dismissed and as a result they're very difficult to treat and their symptoms end up being very refractory there's also a variance in severity and Persistence of symptoms so some patients get better but many of them persist years later
and while you have that 7 to 10 day window of postconcussive symptoms that really should get better still 33% remain with some kind of functional impairment years later and my clinic is chalk full of these kinds of patients years later so we wanted to understand this a little bit more so this is a much larger study that was done between the years of 2014 and 2016 out of both Hopkins ER so the downtown uh ER as well as bayew and we the idea was this is a head injury Ser markers in response to trauma study
initially kind of um identified as a study looking at biomarkers of head injury but we screened about 4,450 patients and at the end of the day ended up enrolling 500 and when we use the vad OD criteria one of the other classification systems and applied it to this cohort as we expected majority of them had mild TBI 47 out of 500 had mild TBI so going back to the definition of TBI remember loss of consciousness altered mental status post-traumatic Amnesia very important what makes something considered mild is the duration of those symptoms so less than
24 hours of PTA and a AMS falls under the category of mild TBI less than 30 minutes of loc mild TBI now you can have normal Imaging findings or you can have a glass caloma scale of anywhere from 13 to 15 which is the normal 15 is a normal scale number so timeline a little bit more chronic than the earlier study I presented so this is within a six-month span so patients come into the ER blunt head trauma they're recruited within 24 hours and we follow them at 1 3 and uh 6 months while the
focus of the study was on biomarkers mostly I'm going to focus what I was interested on which is the post concussion phenomena as well as the psychiatric symptoms and functional outcomes so we did three scales the river meat which is a postconcussive scale that captures neurologic and psychiatric symptomatology the phq9 which you're all familiar with high sensitivity and specificity for detecting depressive symptoms and severity and then we looked at the goes this is called the Glascow outcome scale extended this is a this is basically a scale that looks at functional recovery going on a Continuum
of zero dead to eight full functional recovery we used this as a dichotomous variable and cut it off at seven and said anyone less than seven was incompletely recovered anyone at 8 was fully recovered so what did we find we took the cohort and we divided them into into subgroups in group membership based on severity of symptoms at the outset so those that had higher riverme scores AKA higher PCS or postconcussive symptoms right at the outset are the ones that got worse later on those that had mild minimal postconcussive symptoms at the outset got better
later on then we asked about predictive markers well we know that loc AMS are very important in the diagnosis of TBI and particularly mild TBI what do those clinical variables tell us about who's going to get better as the year progresses so we took all the participants that had mild TBI and we divided them into four distinct groups based on the presence of loss of consciousness and altered mental state so there was a group that had both l L and AMS those that just had loc those that just had AMS and those that had neither
and what we found just as we would expect is that the presence of loss of consciousness and altered mental status at the time of injury resulted in those that had the highest rates of depressive symptoms and postconcussive symptoms which is pretty predictable at the six-month Mark but these were also the people that were at the highest risk of incomplete functional recovery so what did headsmart tell us those with severe PCS early on do worse later those with mild or minimal PCS early on get better later presence of both loss of consciousness and altered mental status
at the beginning of the time of injury means that there are going to be worse outcomes later so now we'll pivot over to talking briefly about management and how we manage and assess these patients because again it is Psychiatry it's just a little bit with there's some nuances that we look at so as with all psychiatric evaluations we want to be very complete and comprehensive you want to do a full fips history what's important with step one though is it's important to ask the family members what was this person like before their injury what was
their personality like what was their functioning like how were they able to interact with people prior to the injury what are they like now are they able to balance a checkbook can they make a grilled cheese sandwich these are things you really want to be asking then you want to do a brief neurological exam all my fellows and residents here are aware that I asked them to bring a tuning fork a Flex Hammer the stellin chart into the clinic because detecting neurological deficits even if it's 6 years out from the injury might explain some of
the phenomena and presentation that we're seeing now important to look at the problem solving F problem focused workups because we really want to figure out what's going on if it's not just Psychiatric so if a patients coming in with sleep disturbance very common after TBI to have obstructive sleep apnea not Central you want to do a full sleep study and you want to make sure that you're not missing this as part of the issue before you start prescribing medications you want to do ancillary studies to help establish the diagnosis so psychosis after TBI very rare
but true story a patient came in having psychotic symptoms that weren't getting better after antis psychotic use come to find out an EEG was never done and they were having post traumatic seizure so these seizure these psychotic episodes were happening in an interial pattern multi-prong formulation really important it's very easy to chalk up people that have a TBI to saying this is a brain disease that's what's going on but we want to take a step back and use the perspective as model to really apply it to the patient and look at it from a holistic
framework multi-disciplinary treatment is really important TBI does not exist in a bubble it's not just Psychiatry but it's all other Specialties and it's important to connect and coordinate and collaborate care and finally consultations and referrals are really important so I'll do a work up for example I'll order a pituitary panel because pituitary hormones are often disrupted after TBI if something comes back back abnormally I'll refer out and send people to neuroendocrine or neuropsychology for cognitive testing it is really important to apply the perspective model to these patients like I said before it's easy for clinicians
to chalk up patients with TBI as they have a brain disease but if we take a step back and go back to the concept of what they have who they are what they do and what they've encountered it's really really helpful for us to characterize and deliver treatment that's specific to that patient so yeah they have a brain injury they've got neuronal injury they've got which has resulted in neuroanatomical and neurophysiologic changes but what about their premorbid vulnerabilities if their personality vulnerabilities sort of lended them to dealing with this particular incident in a different way
that's important for us to know this can sometimes be explained by patients overexaggerating or minimizing their symptoms what about what they do we've talked about impulsivity and disinhibition this can really lead to a lot of problems in the home so substance use domestic violence can often be things that we're thinking about or the lack of behavior a motivation an apathy not doing things can really impair patients in getting to their doctors and actually engaging in treatment and finally demoralization is something we're seeing all the time these are patients that are really struggling with I don't
know who I am anymore after my brain injury and that's where we are sort of tasked with the duty of basically rescripting and working with them to kind of rewrite the narrative as a TBI neuropsychiatrist I would say I spend majority of my time coordinating collaborating care with other Physicians and in other Specialties if it's pm&r neuropsychology neurology Audiology you name it pain management it is truly a multidisiplinary intervention but even within Psychiatry there are different modes that we can use anger management mindfulness occupational therapy social skills groups that we have psycho education so not
only is it interdis disciplinary or multi-disciplinary it's also multi it's also multimodal within Psychiatry when we look at pharmacologic interventions um that we use to treat these patients there are actually not a lot of treatment trials that have been done unfortunately uh one of our former fellows Barry n Paretti and myself wrote a very large systematic review looking at pharmacologic interventions to treat depression after TBI and really there are not that many studies out there but across the board typically ssris are the first line ceraline and calram have the most evidence methylphenidate in one trial
um and in monotherapy was found to be very uh beneficial for PTSD a lot of veterans have been studied in culine has been found to be efficacious if we're looking at apathy inattention executive function problems often times the goto are stimulants or if they don't have a seure disorder amantadine there's robust evidence for these two agents in severe TPI specifically memory deficits are actually being studied in larger trials now but really colon esterase inhibitors especially donil can be very effective it is a little takes a little adjusting to when you have to prescribe donil to
an 18-year-old who has you know cognitive deficits after concussions from sports but it does happen and they are effective lots of times on the conso service and the inpatient Services we are getting called on agitation very commonly particularly with severe TBI and we have a curriculum actually on how to manage agitation in these patients that we're developing because we're finding that non psychiatrists really struggle with this as well um but for the most most part mood stabilizers have Mo a lot of efficacy so valproic acid at doses of 12200 1250 and above or oxcarbazepine and
doses around 1,200 are very useful to manage acute agitation you also want to rule out that this is not a postconcussive or post traumatic confusional state or a delirium and then if this is more of a chronic thing you can use mood stabilizers postconcussive symptoms really don't have a treatment at this juncture lots of times what's happening is people are targeting specific neurological symptoms so headaches with Gabapentin or neuropathic pain as well as tricyclic anti-depressants and finally insomnia a really difficult to treat symptom after TBI you want to start off with doing a full workup
doing the full sleep study cbti for insomnia is very helpful before jumping to other agents that you would use pharmacologically but remelon and trazodone have been found to be very helpful in these particular patients other interventions obviously Psychotherapy so as mentioned before I'm often encountering situations where patients are like I I'm not the same person that I was before so I do come from the approach of we may not be able to get you back to who you were before how you were before the injury we certainly can get you better than you are now
and kind of giving them that hope that they can get better than what they're presenting with today we also want to rescript the narrative and help guide them in that aspect of all of the studies that have been done in specific types of psychotherapy modalities cognitive behavioral therapy has been the most efficacious one thing with cbts you have to be very mindful that you want to deliver a modified CBT to these patients because there is that cognitive sort of deficit piece that you want to be thinking about cognitive Rehabilitation is also very helpful so this
is where I tell patients I'm going to be sending you to the brain gym this is where neuropsychology will give patients specific exercises and tools to kind of help them remember things and help them understand more you know how to keep track of their lives and organize themselves and then of course we do substance use counseling supportive therapy behavioral activation therapy there's some supplements that are kind of up and coming now they're looking at managing postconcussive symptoms nothing's really been groundbreaking so far but people are looking at various sort of off-label supplemental use for postconcussive
symptoms uh pm&r does a lot of physical things to help with brain fog like aerobic exercise there's a lot of aspects of vestibular therapy that help patients that have the postconcussive phenomena that continue and then we also think about sort of physical therapy getting their bodies rehabilitated from a pH physical standpoint and physical perspective so where are we headed with this particular field and what's the future of TBI so the first is we really need integrated care sites so patients come and see me for pharmacologic management then they're going across the hall to see the
therapist but then they're going downtown to see the neurologist and the Audiology and pain management and it's very fragmented so having a One-Stop shop where patients can really be seen by all providers is really really beneficial the second piece is the psychosocial rehab programs most clinics have prps but our patients often times can't tolerate groups they're often blurting things out and becoming disruptive and they get kicked out of PRP which is really not helpful for them this was the impetus for us to raise the and create the hopes program that Dr Rouse started which is
really targeted just for patients with brain injury to help them regulate within groups early screening is really important so now that we've seen that loc AMS is a high predictor for poor outcomes prior history of psychiatric illness or high risk for depressive symptoms early you want to catch this personally I'm interested in neuroimaging screening so my current narad award is looking at patients that are coming out of the ER with firsttime mild TBI and looking at functional neuroimaging changes are there resting state fmri changes that happen in the acute period that might predict depressive symptoms
later on so early screening with neural novel neuroimaging interventions is also really helpful early interventions is key could we talk to our ER colleagues and say hey this guy has a concussive episode he might be someone that's going to do worse could we give them resources on his way out of the ER or her way out of the ER neuros stimulation rtms and ddcs we actually did a study at Hopkins a few years back but generally the effect sizes are pretty it's a mixed bag part of the problem might be because neuros stimulation is being
delivered to the frontal areas in a non-specific ma manner so the dorsal lateral prefrontal cortex is huge so targeting specific areas particularly with neuro navigation and fmri guided neuron navigation might be helpful in making making more efficacious um interventions with neuros stimulation and finally treatment trials for those who are not doing well with pharmacologic agents like traditional ssris what does ketamine look like in these patients what does v otine look like and these are conversations that we're having right now sort of with other institutions as well so in summary the presentation of traumatic brain injury
doesn't always fit the DSM model and these check boxes that we typically see there 's a unique phenomena of symptoms that's often surrounded by this idea of discont control emotional and behavioral there's nothing mild about a mild TBI which you heard today firsthand and there's a lot of things that are involved in multidisciplinary management of these patients both within spe amongst other Specialties and multimodal within Psychiatry and there's a lot that we have to learn a long way we have to go to understand pathophysiology and connections to Psy Psychiatry within TBI I'd like to take
this moment to acknowledge my mentors um and all my colleagues Dr lusto beol and ra have been integral in my career in TBI Psychiatry I'd also like to thank my colleagues who have done a lot of the research that I presented today with and my other mentors Dr Smith and Dr Chisum who have also been integral in my career development and I'll leave you with this final point which is the next time you interview a patient with TBI always remember that there is a complicated battery of symptoms that often revolve around emotional discont control and
behavioral discont control and the more often we're doing this as clinicians we're better able to ask research questions better able to find treatments and do better for our patients and with that I thank [Applause] you was a great hello hello hello oh there we go now W that was a great talk wow great content and magnificent delivery um let me ask start with a question for you Dr Roy the U the emotional liability piece can you talk about the targeting treatment for that particular piece of the equation how do you treat emotional relability yeah so
um that's been explored somewhat in some treatment trials early on a lot of the ssris particularly caline and Citalopram had been used to kind of treat sort of the fluctuations in mood but there is a lot of evidence now that mood stabilizers particularly um valproic acid and even loten might help with that in terms of a treatment standpoint um also frustration tolerance you know from therapy learning about when to figure out where your battery is and where your gauge is from a behavioral stand standpoint great thanks Dr tooski do we have any information TBI location
and of sympoms yeah so you want to repeat the question Zoom audience oh sorry yes sorry so the question is about do we have any information about the location of the TBI and um how that affects treatment particularly and the symptoms that that come about so um we didn't have too much time for to go into the neuro Anatomy which is my one of my favorite Parts about this I this topic so if you think about the brain which is this jelly-like substance and this hard en casement called the skull no matter where the injury
happens because of these frontal temporal bony prominences there's this shearing that can happen so the most vulnerable areas of the brain are the frontal temporal areas in particular the orbital frontal cortex is responsible for sort of that break the go noo so that's where we see a lot of this kind of disinhibition impulsivity and agitation the V medial prefrontal cortex that's typically where we see problems with apathy and then the dorsal lateral prefrontal cortex is really where we have problems with um executive function I don't know if that answers the question so really the frontal
temporal areas is where it's important now if you see someone that has a brain bleed in any of those areas you can kind of expect those symptoms to develop thanks Dr gilbertt yeah so the two scales that were used was the social functioning exam this is where patients are the the patients perception of how they are functioning so this is where they think they are not doing well in their job not doing well in school they think they're a poor spouse and the second was the social ties checklist the connection are you eating lunch with
someone once a week do you have a pet do you see your family members for at least an hour a week so the social functioning from our studies really was encompassing a patient's perception of their functioning as well as social connectedness great thanks other questions yes Dr kog thank you so the question was about in my current narsad study and were we collecting data about prior TBI so the whole focus of this study that we're doing out of the ER is to look at almost to consider TBI as a mechanism of disease so we're only
enrolling people who had no prior history of TBI so this is first time mild TBI and then we're looking at functional neuroimaging but it's a great point to look at repetitive concussions as well because that's obviously it's a it's a cumulative effect but our study only looks just at first time let me just add that um good point good point Dr margas typical clinical encounter any number of types of clinics someone adult 30 years ago when I was a kid playing sports they said maybe I had a I was in an accident I had a
headache for a while afterwards and that's that's a very so the question is about if someone had a remote many years ago history of TBI how do we sort of take that into consideration when thinking about other disorders so I think that just goes for me goes back to taking the fips and looking at the chronology so you run the risk of patients kind of attributing their symptoms maybe to a TBI which might happen but I always that's where I really like to pinpoint the collateral because if a family member can tell you what they
were like right after that injury and if it was really a negligent thing that Happ you know it was just a negligible experience and it was just you know a brief tap on the head or something like that then you know that it's likely not playing a role now but I usually like to get the chronology much more specified and what I do is I get the details of that injury and exactly what happened because if it typically if it was really that much of a devastating event you will hear a lot about it when
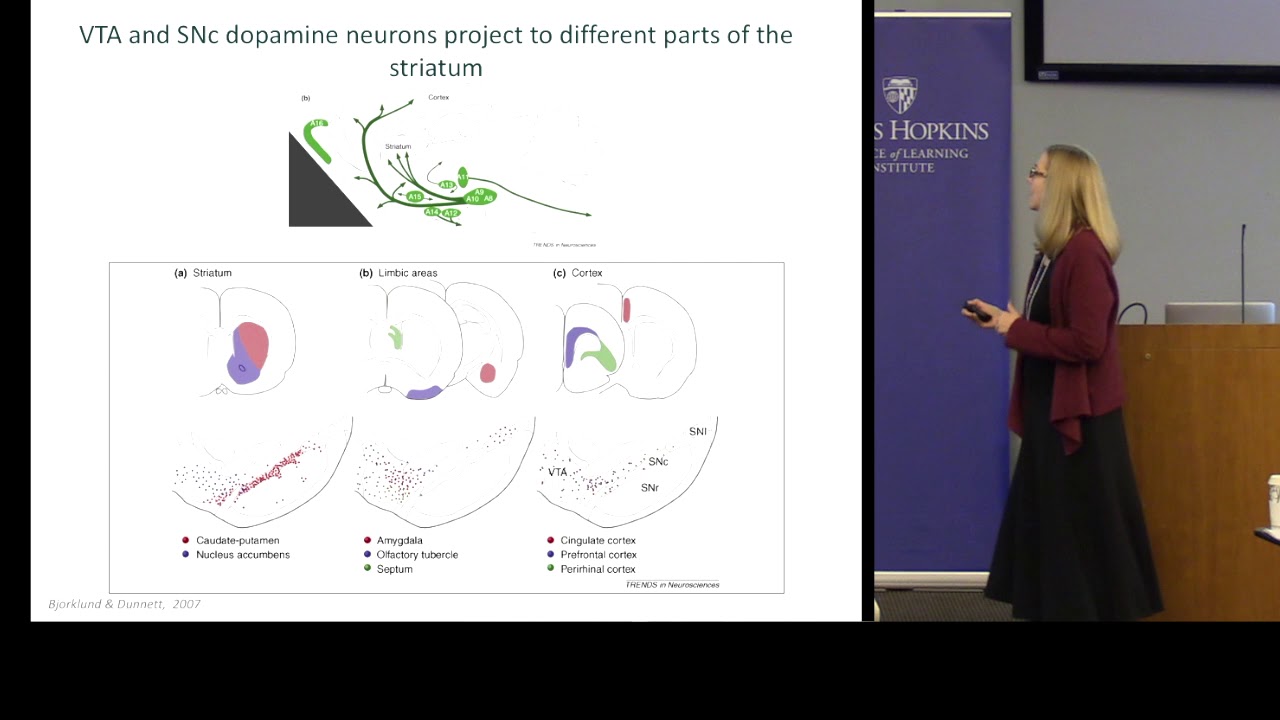
they're talking about that particular thing but if they're kind of bringing it up sort of in hindsight the importance might not be as much uh have as much weight I think other questions yes go ahead second thank you question absolutely so the question is about the role of the cerebellum and you know how much importance we put into that in in formulating so the cerebellum is actually a very very important especially in neuros Psychiatry we're talking a lot about it now especially because of the proje projections to the frontal areas of the brain and its
responsibility for attention and coordination and motor function is really important um I I a lot of the times with the Imaging that we get of our patients much of the focus is really on the cortical structures and subcortical structures and we're kind of looking at that but I think this points back to the idea of when we do our brief neurological exam and getting a history if we know that there was some cerebellar dysfunction there early on that that may also be contributing to the mood libility and a lot of the instability that we see
with affect that's happening and so um but I think also um when we send our patients over to pm&r they're able to do a lot of the cervical vestibular interventions that can sort of address some of these symptoms as well great thanks other folks let me ask you another question der the U you mentioned the uh a study looking at serum markers yeah uh I I presume we would have heard that there have been positive findings and something like that are there any physical tests that can tell us much about uh about whether a person's
had a serious TBA the issue is that a lot of the serum markers like for example bdnf um was one of the big ones that was looked at they're very nonspecifics for the CNS so um in terms of that particular study nothing really did would pan out because you know you have to Target it specifically to areas now there are specific proteins when we are talking about for example CTE like td3 uh tdp43 and other types of proteins that we might be wanting to look at for long-term outcomes but I think right now we're just
continuing to explore other peripheral markers and and I guess mild TBI I think you said is defined as in part by the absence of Imaging findings right typically so typically Imaging findings are normal now there is a subset that do have brain bleeds that can be considered complicated mild TBI and that's a whole other uh discussion but um generally speaking most classification systems consider the structural Imaging to be normal structural Imaging so so I guess General mild TBI is like is like all of our psychiatric illnesses in that the diagn diagnosis is is entirely syr
there's nothing there's no physical basis for Di a clinical diagnosis based on symptoms yeah anyone else okay with that I will thank you for a really wonderful Grand rounds thanks thank you thank you