[Music] what is up guys Karma medic here and welcome back to another dose taking a history arguably the core of clinical practice and the most important skill that a doctor needs to learn in today's video I want to talk about some of the key points that I've learned throughout my time in medical school which have been really helpful for me when taking patient histories in the hopes that anyone watching who needs a little bit more structure or information will find them useful if you're new to the channel then hi my name is Nasser and I'm
now a final year medical student studying at Kings College London I think this video requires a bit of a disclaimer I am not a doctor I am a final year medical student and all of the content of this video is for information and education purposes only this is not medical advice this is not the perfect guide to taking a history or anything like that this video is a collection of things that I've been taught in my medical school and things that I've personally found useful when on the hospital during clinical placement now with that lovely
disclaimer out of the way let's get right into it so before starting the history there's generally two things that I try and keep in mind first of all I try to remember the context that I'm in so if I'm talking to a patient in the emergency department that's going to be very different to talking to someone in general practice or in the Cardiology Ward on top of that talking to someone who's just been admitted to hospital on day one might be very different to talking to a patient who's now on day five they might be
a bit more relaxed a bit more happy to talk to me as a medical student as compared to when they just walked into A&E complaining of something like pain this helps me stay a bit focused so that I can direct my questions and thinking towards why the patient is here to begin with the second thing is that being overly nice smiley happy genuine kind Etc when beginning a patient history I find goes such such such a long way even if the patient is quite grumpy to begin with and doesn't really want to talk to me
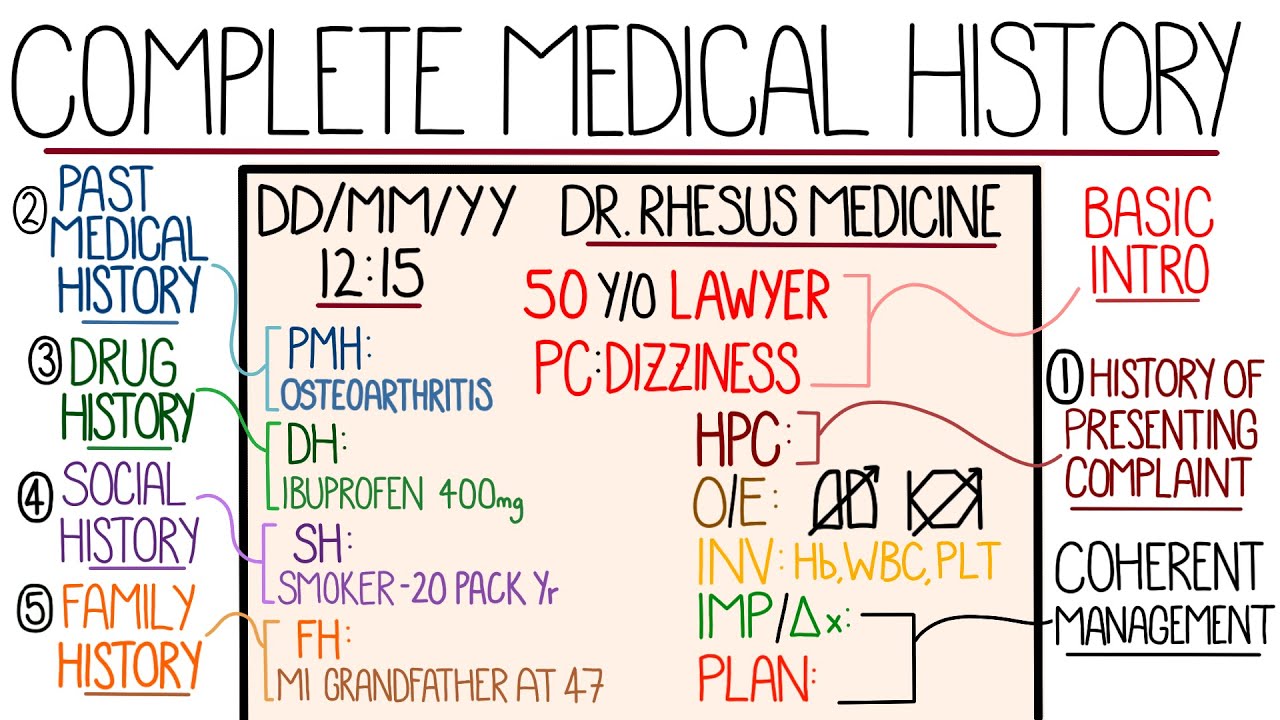
as a medical student I find that by the time I've introduced myself exchanged a couple of Friendly Smiles and asked them some questions about them I've already made great strides in connecting with the person in front of me and the history just becomes smooth sailing from there so moving on to the actual history the general outline of a history is as follows you have the presenting complaint history of presenting complaint systems review past medical history drug history family history social history Etc now this is subject to change based on the clinician the situation but definitely
for me as a medical student I find it very helpful to have this structure because it makes sure that I get through all the topics that I want to and that I don't forget any key information but patients are very different and I think it's important to be able to adapt and sort of go forwards and backwards be a bit more fluid with the structure if necessary but I don't always follow the structure patients can be very different and letting them lead the conversation and us being a bit more fluid with the different sections sometimes
makes for a much better history now on top of this structure something that I try not to forget something that Kings College London as a medical school has forever drilled into my brain is called ice so ice stands for ideas concerns and expectations and I actually find it really useful for honing in and finding out exactly what the problem is that the patient has come in with today if a patient has five different things that they want to discuss then asking them if there's anything in particular that's concerning them might help hone down and focus
the conversation asking about ideas and expectations also allows the patient to express their emotions and feelings which is something that can be easily forgotten if we're just going through the the structure trying to pick out all the important medical information so I do feel like it unlocks an extra level to the history and sometimes gives that really important information that you'd otherwise Miss I'll talk about eyes further in the video as we go along but for now let's start with approaching the patient so every patient history starts the exact same way starts with an introduction
patient safety and infection control this is commonly remembered with the acronym wiper which stands for washing hands introducing yourself patient details exposing the patient if necessary and reposition so washing your hands Obviously good for infection control but also to show the p that you're now clean if you move on to examine them after or during the history now introducing yourself of course is very important we generally give our name our grade and where we are for example hi good afternoon my name is Naser Karma and I'm one of the final year medical students here on
the respiratory Ward this very quickly and adequately explains who I am after that we move on to patient safety so you want to double check that the person who's in front of you is the actual patient who you are intending to talk to or take Bloods from or perform an examination on this is done by confirming two pieces of information commonly the patient's name and date of birth for for example could I start by confirming your name and age please asking for age instead of the date of birth helps you skip the mental math in
your head of trying to figure out how old someone born in 1957 is age gives you a lot of information to begin with and also gives you a lot of context for the presenting complaint of the patient a 15-year-old 45-year-old and a 65-year-old presenting with per vaginal bleeding has a very different set of differentials finally explain what it is that you're here to do and gain consent obviously this is very important you need verbal confirmation from the patient that they are happy to go ahead and talk to you so what I'll usually say after I've
introduced myself and confirmed the patient details is something along the lines of I've been asked by one of my seniors to have a conversation with you about what's brought you into the hospital and your past medical history would that be okay and only once they've agreed to have this conversation with me I can move on to asking them questions starting with the presenting complaint so the first part of the history is the presenting complaint or in the US I believe this is called the presenting illness so this is when you're trying to understand from the
patient the exact reason why they are in the emergency department general practice or hospital right now so for example a might say that they fell over or hurt their foot that they feel their heart is beating very fast they're having shortness of breath or they've noticed a new rash on their back this very specific singular thing is the presenting complaint a really great way of getting this information from the patient is by asking them an open-ended question and just letting them talk for as long as they need to before we ask another question we've been
taught by kings that this is like the golden rule of taking a history you ask one open-ended question and then let the patient talk for as long as they need to without interrupting so my go-to question is something along the lines of can you please tell me what's brought you in today or can you please tell me what's brought you into the hospital after this question the patient usually goes on to describe everything that's going on that might be one thing or three things but now I know what they are and I can go into
further detail about them in the history of presenting complaint so the history of presenting complaint or the history of presenting illness is about further exploring whatever the presenting complaint was so you take what the patient told you and you just dig dig dig and explore explore explore and find out everything that's going on surrounding that thing so for example when did this start is is it old or is it new how long does it last what medication have you tried already etc etc my classic go-to question over here is could you please tell me more
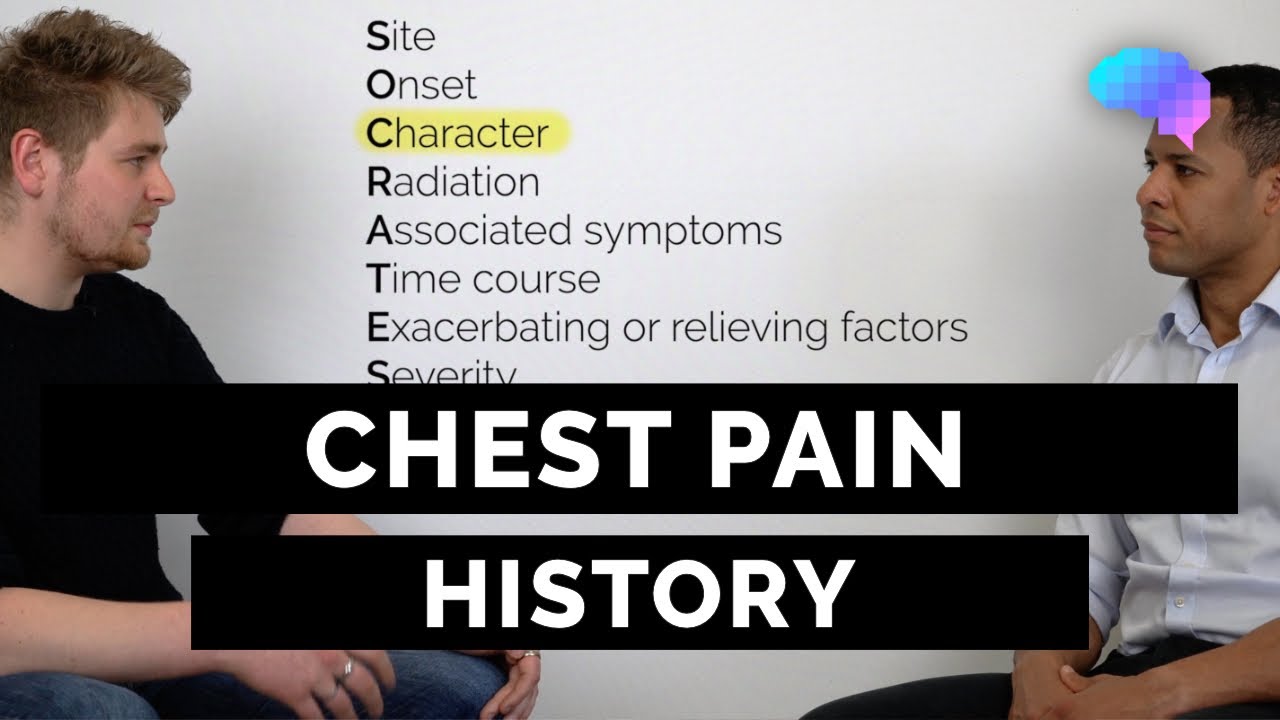
about that now there's some really good acronyms for some of the most common presentations and types of histories for example if someone is complaining of pain one of the common things used to explore that pain is an acronym called Socrates so Socrates stands for Sight onset character radiation Associated symptoms timing exacerbation or relieving factors and then scale or severity so this is kind of an easy way to remember all the different things that you need to ask when it comes to pain if it's a gical history we use the main outline of mosque which stands
for menstruation obstetrics sex and contraception if it's an obstetric history we use GMC if it's a pediatric history we use bfgd there's all kinds of acronyms for different kinds of histories regardless of what the history is I always try to ask adopt which is d o PT it stands for duration onset progression and timing I always find it really helpful and I think it helps put the patients presenting complaint into a lot of perspective by the end end of the history of presenting complaint you should have a really detailed idea surrounding the events that brought
the patient into the hospital what happened before during and after is especially important for things like uh episodes of collapse for episodes of self harm by now you've probably started thinking about what direction you want to take this history in and how you want to narrow down to ask your more focus and specific questions this is a good time to ask those more specific questions that will help you include or exclude the most serious diagnoses so for example for someone with chest pain you want to make sure that you exclude something like a myocardial infarction
or a pulmonary embolism I generally find this also a good time to cover ice I tend to ask something along the lines of do you have any idea what might have brought this on or do you have any idea what might have caused this most of the time the patient will say I don't know which is obviously completely fine and reasonable but other times a patient will say something like I bought a dog around the time all this started happening or there was a really stressful event in my life or something like that after you've
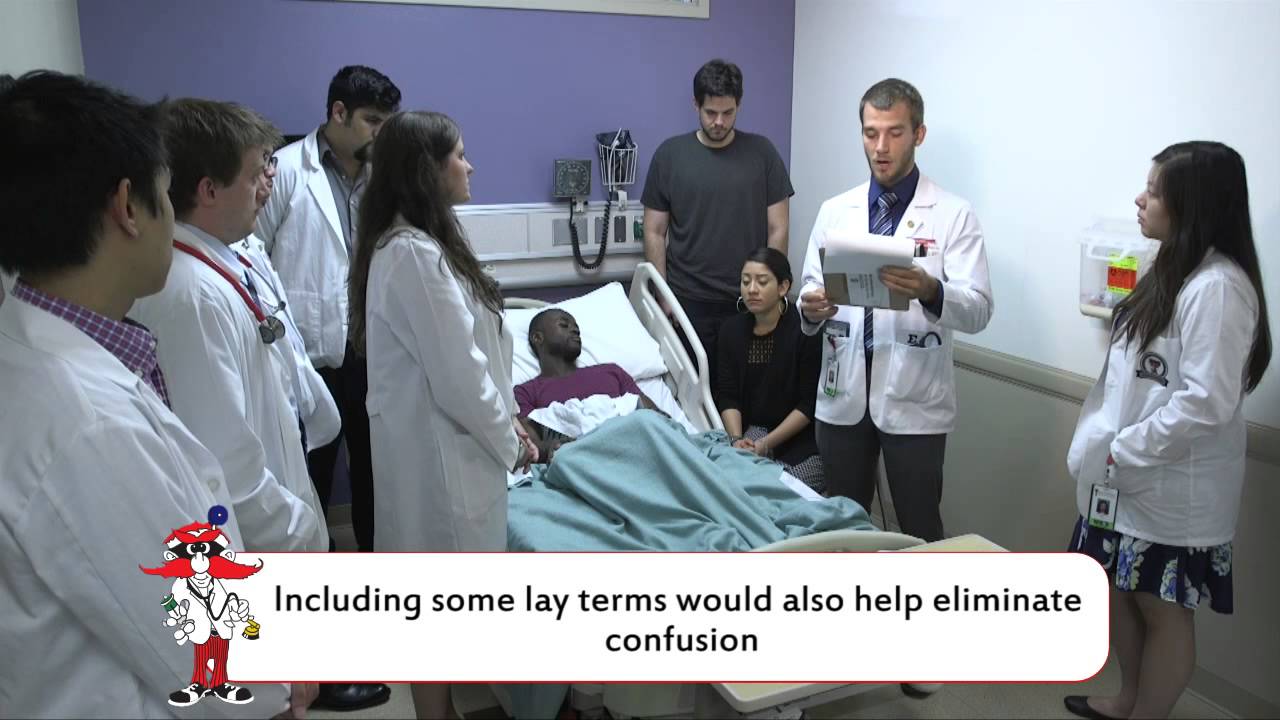
gotten most of the information from the history presenting complaint this is a good time to summarize back to the patient everything that you've heard from them this has two Main benefits the first is that the patient feels like they've actually been listened to and that you're taking their complaints seriously the second is that if you've misunderstood something from the patient or they've forgotten to tell you something in particular this is a good time to fill in those blanks and now we're ready to move on to the systems review this is so so so useful it's
actually something that I never used to do because I thought it would take up way too much time especially in the pressures of an OSI exam but I found a great way of doing it and I think it can be very helpful it helps me make sure that I don't miss anything and that I get every single detail and it helps remind the patient of something else that they might have forgotten to tell you so systems review is exactly what it sounds like it's when you ask a couple of questions for each of the systems
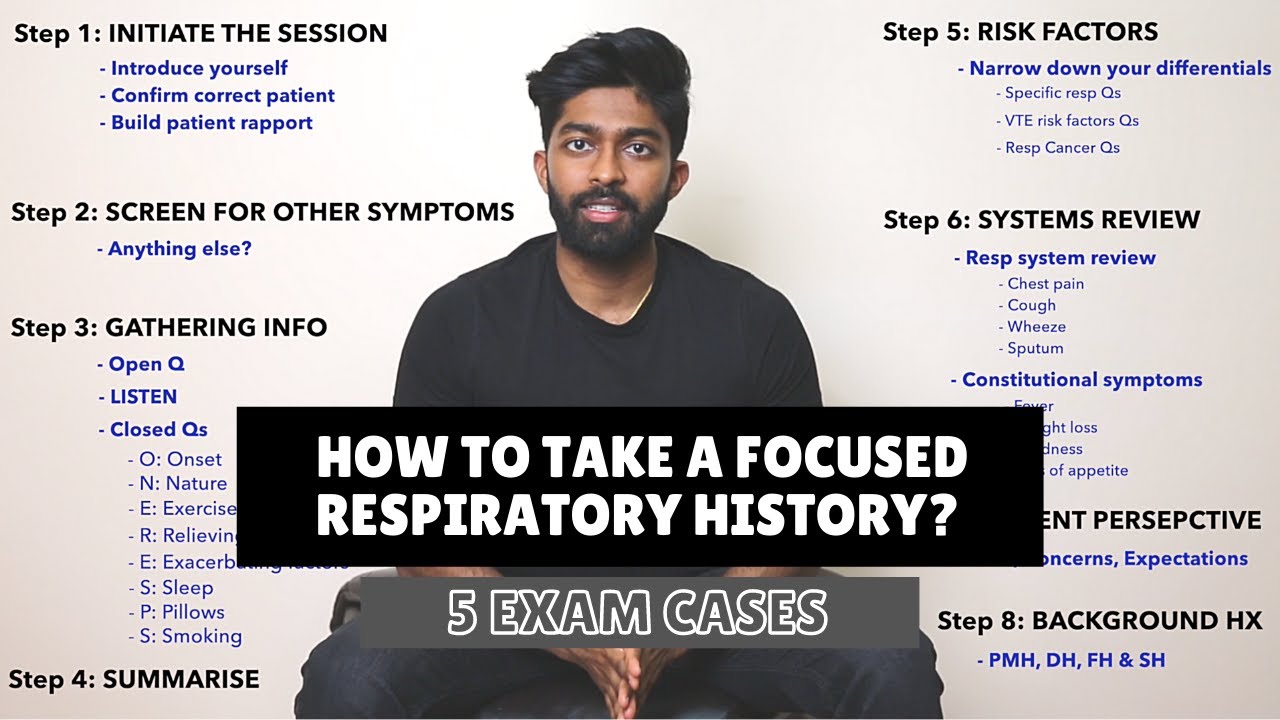
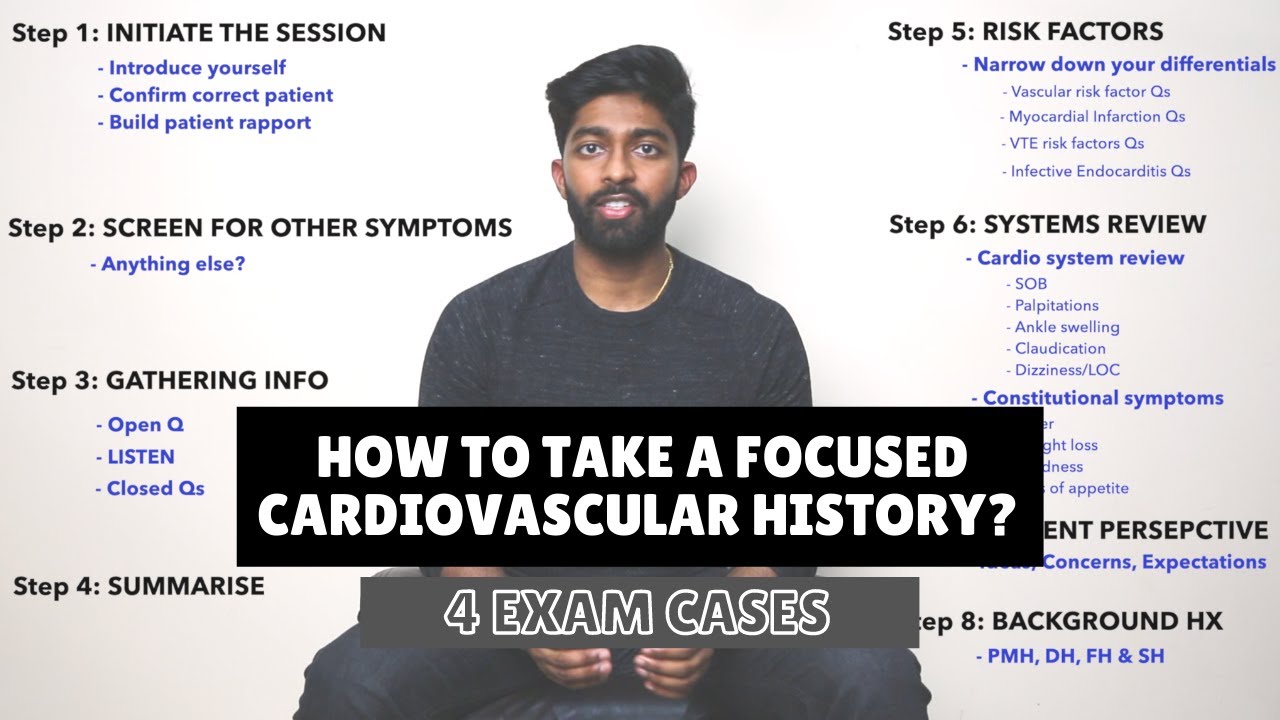
of the body just to kind of peek in and check on each of the systems to make sure that they're okay now as you become more confident you can ask specific questions that focus on the specific body systems that you think are relevant based off of the presenting complaint and history of presenting complaint but I'm definitely not at that point yet and I like to ask questions from each of the body systems to make sure I don't miss anything I'll put a picture of all the possible questions you could ask somewhere up over here you'll
never have enough time time to ask the mo so you want to pick and choose the most important ones for the history that you're taking so here's how I do a systems review I say to the patient that I'm going to ask a couple of questions back to back bear with me it might seem like a lot but it's just to make sure that I don't miss anything and once they say okay I can begin so for example have you had any headaches recently any changes to your vision have you had a sore throat runny
nose or difficulty swallowing have you had any chest pain have you felt like your heart is beating very quickly any shortness of breath or cough any nausea or vomiting any tummy Pain any changes in your bow habit are your Waterworks working normally any rashes or joint pain and then finally and very importantly the Constitutional symptoms so any fevers night sweats or unexplained weight loss and that's it it takes something like 30 seconds to 45 seconds and covers a ton of information if I missed anything during my investigation in the history presenting complaint then it's most
likely going to show up here now moving on to the Past medical history this is extremely important sometimes the problem that the patient is presenting with now can be a complication of an existing condition or an event in their past medical history so getting every bit of information here is key one thing that I found is that some patients don't consider things like asthma high blood pressure diabetes as part of their past medical history probably because it's something that's very chronic that they've been living with for a long time and so they don't see it
as a condition or illness that they have so it's something that I always screen for and make sure to ask specifically you can usually get all the relevant information from the patient by asking them something along the lines of do you have any long-term health conditions or any illnesses that you see your GP for another important thing to ask is whether the patient has ever had any surgery been admitted to the hospital or had any visits to A&E some people find the pneumonic Jam threads helpful but personally I don't use it if you're interested the
acronym stands for jaundice anemia myocardial infarction tuberculosis hypertension romatic fever epilepsy asthma and COPD diabetes and stroke drug history so this one tends to be quite simple you simply ask for all the medications that the patient is currently taking whether that's prescription drugs or overthe counter drugs sometimes it's also important to ask whether any medications have recently been stopped or any new medications have been started even though medicines and drugs are amazing and help cure a whole wide range of conditions almost all of them even the ones that you might think are really benign that
a lot of people take will also come with side effects for example things like anti-hypertensives antiglycemic statins these are medicines that a lot of people take and are considered to be fairly common but they all have their side effects so having a list of all this medication is really important also something worth asking is do you take your medications regularly as prescribed there's no point in us having it in our systems that the patient is taking X wied medication if they don't actually take it when they're at home one resource that has helped me immensely
in Remembering pretty much everything that I need to know regarding medication is sketchy medical sketchy medical is this visual Learning Resource that helps you remember drugs their mechanism of action their side effects Etc through these beautifully weird drawn out pictures personally whenever I'm asked about a medication on a ward round or something like that I will literally picture out that image from sketchy medical and go to the part of the drawing that helps me answer the question it's a great resource you should honestly check it out if you don't know about it already last thing
in the drug history and something you never ever ever ever ever want to forget is to ask if the patient is allergic to anything whether that's medication or non-medication this has to be written down in the notes somewhere so family history is exactly what it sounds like I tend to ask something like do you have any illnesses or conditions that run in the family something else you could say is can you tell me about the health of your family again over here I feel like being specific about things like asthma diabetes and hypertension is sometimes
needed I found that patients don't tend to bring these up unless specifically ask a patient's family history can put into perspective their presenting complaint especially if it's a condition that has a strong genetic component a family history of heart disease diabetes liver or kidney disease Etc now especially with older patients it's likely that their parents or siblings may have already passed away and so it's important to be sensitive when asking these questions and trying to elicit this information one important thing to ask if a family member has died from a specific disease is that what
age they passed away someone passing away from cancer at the age of 40 or 50 is going to be very different than someone in their '90s I think over time you'll develop your own way of sensitively asking for this type of information but generally just showing empathy and compassion wherever you can goes a really long way and finally social history the all important social history common questions asked in this section are if the patient smokes and if so how much if the patient drinks and if so how much and also if the patient uses any
recreational drugs now before that last question it's important to sign poost a lot of people can get offended if you ask them about the use of recreational drugs so something I like to say is a bit of a strange question but but it's something that we ask all of our patients do you use any recreational drugs also in the social history if you've forgotten to ask previously please don't forget to ask about allergies other important things to ask here are about the patient's occupation and what their living situation is like at home so for example
who do they live with at home how many floors are there in the house are there stairs Etc if you're speaking to a child or adolescent then the acronym heads can be very useful this stands for home education activity or employment drugs and then sex social life and suicide if you're talking to an elderly patient something that's good to ask is about their ADLs or activities of daily life so are they able to go to the shops and get groceries for themselves are they able to cook and clean after themselves Etc and then lastly this
is also a good time to screen for mood so something you can ask is how have things been at home recently how would you describe your mood something along those lines so one final bonus tip this is something that I used to use a lot especially when I first started taking histories if I ever feel like I'm really stuck and I feel like I haven't managed to find out exactly what's going on I used to say something along the lines of the following okay Mr Smith you've given me quite a lot to think about today
is there anything you think might have caused this or anything that's concerning you in particular this usually helped solve all of my issues and on top of that it helped cover ideas and concerns from Ice just generally if you're feeling stuck honestly going through ice is very helpful and that's it please bear in mind that this video is sort of an amalgamation of what I've been taught at my medical school and what I've learned things that I found particularly helpful throughout the years this is by no means the golden rule book to taking a patient
history and I'm sure that there's better ways to do all of the sections speaking of which if you've got any tips tips or tricks or something helpful that you'd like to share please do leave them in a comment down below I'll be reading through them and incorporating them into my history taking thanks so much for watching I hope you find this video useful and I will catch you in the next one peace