- Hello, I'm Vic Baum. I'm a medical officer in the Office of Blood Research and Review in the Center for Biologics Evaluation and Research, or CBER, at the FDA. And the next talk in this series is gonna be on investigational new drugs or INDs, and I should tell you up front, in the vernacular, so to speak, IND is used to refer to investigation of new drugs and investigational new drug applications.
So then, what's an investigational new drug? Well, investigational drug is a new drug or biologic, and for our purposes, I'll use drug to refer to either drugs or biologics in most cases. Anyway, it's a drug or a biologic that's used in a clinical investigation or a biologic that's used for in vitro diagnostic purposes.
So then, what's a drug? A drug is intended for the use, and this is a phrase that you come across a lot, it's intended for use in the diagnosis, cure, mitigation, treatment or prevention of disease intended to affect the structure or any function of the body or man. Now, you would think that would be obvious, but actually sometimes it's not, and there are discussions about whether a product is a drug or, say, a dietary supplement.
You need to know that this does not apply to the use of an approved product. In other words, FDA does not regulate the practice of medicine. And an appropriately licensed clinician can elect to use an approved drug that's out there for any purpose that they'd like, and the FDA is not part of that discussion.
So, why is an IND needed? In other words, why would a sponsor feel obligated to obtain one? Well, the bottom line is that only approved drugs can be distributed across state lines, you know, and interstate commerce, if you will, so that since investigational drugs are, by definition, not already approved, an IND allows the sponsor to ship the drug interstate for the purposes of conducting clinical investigation.
And finally, all investigational drugs need to carry this warning label, "Caution: New Drg. "Limited by Federal, or United States, law "to investigational use. " So, all clinical trials should be conducted in accordance with good clinical practice.
A good clinical practice is described in the Code of Federal Regulations, the CFR. As you can see here, a 21 CFR 312 is where INDs are discussed at some length and also in the International Council for Harmonisation Guidance that you can see there. And these are really essential readings to understand clinical trial design performance and data evaluation.
And what they do is provide a unified standard for designing, conducting, recording and reporting clinical trial results, and they not only provide a description of the content and format of IND applications but also for the investigator's brochure, if required. An investigator's brochure is something the sponsor has to distribute to investigators of multi-institutional studies. And what GCP does is it provides assurances to subjects, potential subjects, and to the public that the rights, safety, and well-being of trial subjects are protected, going back to the principles of the Declaration of Helsinki, and that clinical trial data are credible, because if the population at large isn't convinced of that, then they're not going to enroll in clinical trials.
So some of the principles of good clinical practice are that, of course, the anticipated or purported benefits have to justify the risks, and very importantly, the safety of individual subjects prevails over the interests of science and society. So, even if a clinical study sounds like (laughs) a really good idea and would be a benefit to society as a whole, if it presents excessive risk to individual subjects, it's inappropriate and shouldn't be done. Studies have to be supported with adequate clinical and nonclinical data and studies have to be described in a clear, detailed protocol, which is scientifically found.
Studies have to be conducted in compliance with a protocol that has prior institutional review board or independent ethics committee approval, and it has to be conducted by qualified individuals. Studies may only be initiated after obtaining informed consent. Data have to be protected by proper recording, handling and storage.
The studies must maintain patient confidentiality. Studies have to be done using investigational products manufactured, handled, and stored in accordance with GMP or good manufacturing practice. And procedures have to be systemized in advance to assure the quality of every aspect of the trial.
In other words, these can't be fill-in-the-blank protocols and made up as you go along. Here are what you need to know about IND applications. And these are outlined again in this section of the CFR.
First is applicability. In other words, when is an IND required? Those of you who have done clinical trials know that not all clinical studies require an IND, and we don't have time today to go into all the exceptions, but they are listed here.
It describes the phases of clinical investigations, and we'll get to that on the next slide. An IND must be in effect before a clinical investigation that requires IND can begin. This section also talks about the IND content and format as do additional FDA Guidances, but, you know, IND applications are highly choreographed, if you will, and we'll look at that on the next slide.
And this helps sponsors to know what to submit to FDA and helps FDA know where to look for information or specific information and to help us more readily determine completeness of the application. Now, nothing is etched in stone. So, even after an IND is active, sponsors can submit a new protocol, if it's sort of in a related area, or a revised protocol.
You know, during the conduct of a study, things come up, and there are sometimes revisions that need to be made, some of these minor, some of these major, and these are submitted to us, and we'll take a look. Sponsors need to submit, also they, or they may submit information amendments, which could be any information they want us to know, or it could be a response to questions we've asked them. They need to submit IND safety reports, annual reports, and they need to inform us in writing if they want to withdraw an IND for some reason.
So, this is an outline of IND application. There's a general introductory statement, a general investigational plan, an investigator's brochure, if it's a multi-institutional study, and a protocol or protocols, and all the associated information. They have to submit data on chemistry, manufacturing, and control or CMC, and we'll talk about this in a bit.
Pharmacology and toxicology data, I'll have a slide on this. Previous human experience with the drug, if there is anyone, if there is any rather, and any additional information that they'd like us to know. In general, for all phases of clinical trials, the most important goal is to assure the safety and rights of subjects, but in addition, for phase two and three trials, they help assure the quality of the scientific evaluation of drugs.
It's adequate to permit an evaluation of the drug's effectiveness and safety and eventually lead to approval or licensure. What are phase one studies? Phase one studies are generally limited to a relatively small number of subjects, let's say less than 50, typically involve healthy volunteers.
They have a primary focus on safety and tolerability and a secondary focus on demonstrating preliminary evidence of activity and maybe some evidence for dose escalation. Phase two trials, generally up to a few hundred subjects, and enroll patients who now have the disease or condition to be treated. They have a primary focus on safety and tolerability and a secondary focus on demonstrating activity of the product.
Again, some evidence for dose escalation, to determine what dose or dose range will be used in the phase three trial, now preliminary evidence of efficacy and these trials need to be registered at ClinicalTrials. gov. Phase three studies are now the pivotal safety and efficacy studies that form the basis for a marketing application, a BLA for biologics or NDA for drugs.
The size is dependent on the disease of population and study design. For a rare disease, it may be not more than a handful or two, but for let's say cardiovascular trials there may be several thousand subjects. The primary goal here is to confirm clinical benefit and also to expand the safety knowledge base and overall to evaluate the benefit risk relationship for the product to provide adequate data for labeling, and again, these must be registered with ClinicalTrials.
gov. There are also phase four studies, which are post-marketing, so these actually aren't part of an IND but phase four studies may be requested or required by FDA and address issues of safety or pediatric product development. So if we, the FDA, have significant concerns about a trial, we can impose a clinical hold, which can be temporary if sponsors adequately respond to our concerns, so a clinical hold can be imposed on the grounds of unreasonable or significant risks to subjects if investigators aren't qualified, if the investigator's brochure is misleading, erroneous or incomplete, if the IND doesn't contain sufficient information to assess risks to subjects, or if the study is for life-threatening diseases that affects both genders and for some reason the trial excludes one gender or the other.
So for phases two and three, any of the conditions applicable to phase one studies apply. And, in addition, if the trial is clearly deficient in design to meet its state of objectives, and we will look at protocols very seriously to assess this because if the trial is not gonna be able to meet its objectives, then it's exposing subjects to needless risk. What about manufacturing or CMC information?
Well, they need to tell us about raw materials. The sponsor needs to describe the entire production process from beginning to end. They need to characterize the product so we know what it is.
They need to inform us of process validation, testing, and products need to be manufactured again in compliance with current good manufacturing practice. What about pharmacology and toxicology considerations? Well, sponsors need to tell us about the clinical evaluation or the planned clinical evaluation for toxicology.
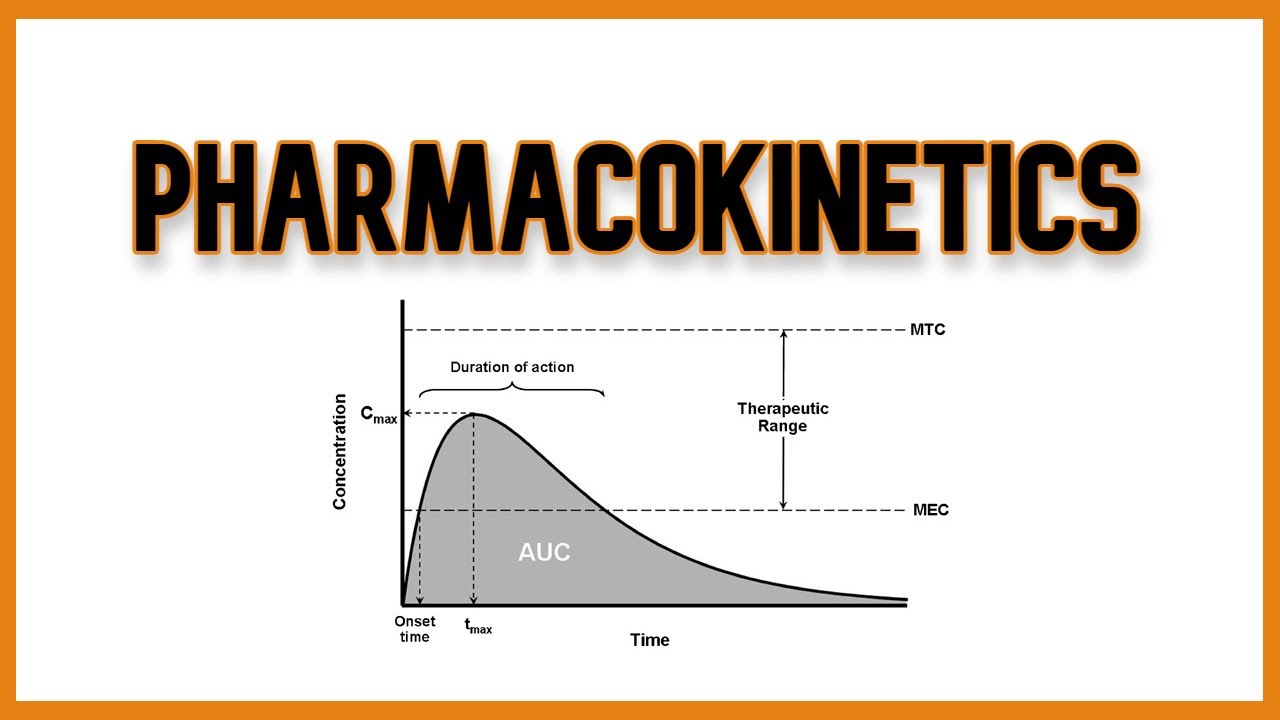
They need to tell us why they selected the animal models, if they did, and why those are relevant. And in some cases, in fact, there are no relevant animal models. They need to provide pharmacokinetic data they've generated in animals, immunogenicity data, genotoxicity data, medical device biocompatibility, and medical device chemical characterization.
In other words, what happens if, for example, you take this drug and put it in a plastic syringe or plastic storage bag? Well, clinical considerations, the sponsor needs to include a statement of the objectives and purpose of the study. In other words, why are they doing it?
Does it have a good basis in science that you need to give us an estimate of how many patients or subjects they're going to enroll, inclusion and exclusion criteria, the dosing plan. In other words, how much are they gonna give? How are they gonna give it?
And for how long are they gonna give it? They need to provide a plan for patient monitoring for both efficacy and safety. They need to provide stopping rules and dose adjustment rules for phases two and three studies, in particular.
They need to report to us adverse events. They need to provide a plan for pediatric development, and they need to discuss the demographic subgroups that they'll be studying. So what are the responsibilities of sponsor?
Well, first of all, what's a sponsor? A sponsor is the entity, well, actually takes responsibility for and initiates a clinical investigation. Now, that can be an individual or more likely, but not necessarily, a pharmaceutical company, a government agency, academic institution or, in fact, any other organization.
If it's an individual, they then become sponsor investigators and resume this, the responsibilities, of both sponsors and investigators. So sponsors need to select investigators and clinical sites. They need to provide the investigator's brochure to all the principal investigators or PIs.
They need to notify and submit all information to the regulatory authorities, like FDA, so that investigators communicate with sponsors, but it's the sponsors that communicate with the FDA. They need to promptly inform PIs and the FDA of any significant new adverse effects or risks that become apparent. They need to assure adequate monitoring.
I mentioned they're the ones who interact with FDA. They need to act if they become aware of potential investigator non-compliance. Now, that's rare, but it does happen.
They need to notify us and the investigators of premature termination or suspension of the trial, and they need to submit final study reports to FDA. They need to keep PIs informed of any new observations. They need to, again, inform us and PIs of adverse events.
They're responsible for quality assurance and quality control and developing standard operating procedures. They're responsible for trial and data management, but they may elect to allocate these duties and functions to and contract with a contract research organization. Now, you know, it may be that a new or a small sponsor may not have the in-house expertise to actually conduct a clinical phase three, certainly, clinical trial.
Sponsor is responsible for auditing and for producing and distributing the investigational product. Again, phases two and three require registration on ClinicalTrials. gov, and any sponsors need to include this form certifying that they have.
Again, they need to monitor studies to verify that rights and well-being of human subjects are protected, that data that are reported are accurate, complete and verifiable from primary source material and are in compliance with the protocol GCP and all appropriate regulations, and sponsors have to select monitors who actually go out and do this and train them appropriately. Well, what about investigator? What's an investigator?
Well, that's the individual who actually conducts a clinical investigation. In other words, under who's immediate direction the drug is administered or dispensed. Now, if there are multiple investigators at one site, the PI is the responsible leader of the team.
Anyone else is a sub-investigator. And their responsibilities include actually conducting the clinical trial at their site, adhering to the investigational plan, in other words, the protocol, and all applicable regulations. They're responsible for human subject protection, assurance of IRB review, obtaining informed consent, submitting case histories to the sponsor.
They're responsible for records retention for at least two years. They have to control and dispose of investigational products appropriately, and they have to report progress reports, safety reports, final report, and financial disclosure report to the sponsor. Finally, may sponsors charge subjects for participation in clinical trials?
And the answer is yes, they may, but these may only be for direct costs. So if they wanna charge subjects, for most situations, the sponsor will develop and submit an explanation of why charging is necessary and what they're charging for. FDA will review that and either agree with the sponsor's plan or reject the sponsor's plan, or modify it.
We may say, "Well, gee, you know, "charging for that looks good, "but charging for that doesn't look good. " And importantly, sponsors may not charge for the normal costs of doing business. In other words, they may only charge for direct costs only.
They may not charge for things like, you know, paying their phone bill and keeping the lights on. Finally, IND studies may not interfere with efforts to develop the drug for marketing approval. In other words, a sponsor couldn't develop a large IND enrolling many subjects and charge them a substantial amount, you know, and then say, "Well, wait a minute, "I'm generating all this income from the IND.
" Why would I now go through the bother and the large cost of developing, you know, a marketing application, a BLA or an NDA? I'll just say, "We are. " And they can't do that.
So with that, I thank you for your attention, and have a good day.