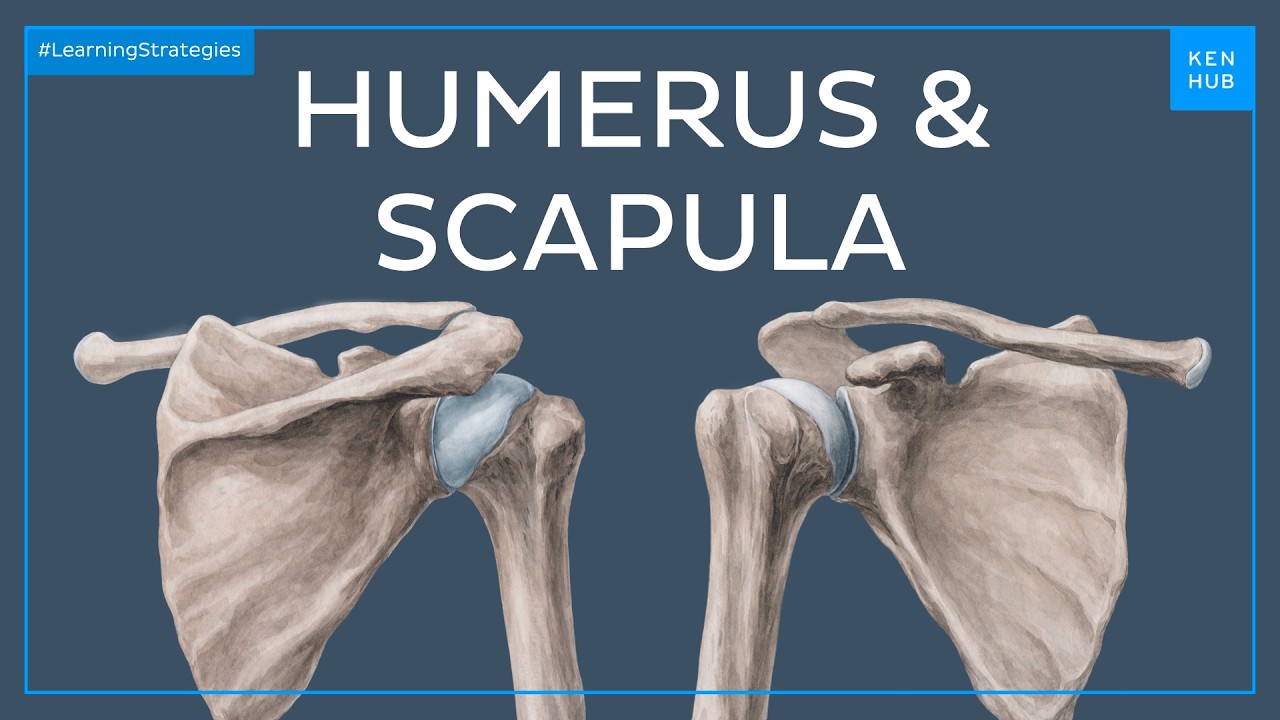
I will start by looking at a simple diagram which has the right shoulder joint seen from an anterior viewpoint as well as elements of the axial skeleton the axial skeleton elements that are seen here include the vertebral column and the ribs and I'm going to remove these as well as the clavicle we are and we are now left with these two bones that participate in the formation of the shoulder joint the first one of these is the scapula it is seen here as a large flat triangular bone and it articulates with the proximal end of
the humerus which is the single bone of the arm the scapula itself if you observe the scapula it has an inferior pointed end which is known as the inferior angle and from this inferior angle we see two borders that diverge away from each other one of those is on the medial side and is called the medial border of the scapula as being traced out here the other side is known as the lateral border of the scapula and it is traced out here in yellow these two borders as they go superiorly they diverge from each other
and they have some very important structures in the form of prominences that one can see the first one of these is known as the coracoid process and it is being labeled here the coracoid process is a projection of bone that is projecting laterally as well as anteriorly and it's shaped like the beak of a bird and hence the name coracoid there's a second projection which is much larger than the first known as the acromion process and it is seen here the acromion process is a rectangular piece of bone that is the highest point of the
scapula or the highest point of the shoulder region and hence the name acromion acromion hi and it's a root word that is often used in other medical conditions as well medical structures like acromegaly which means height or somebody who is extra tall and and so a crow and acromion comes from the same root there's a third important structure that is seen in the superior lateral part of the scapula this is the glenoid cavity and it's point it's labeled here the glenoid cavity is a relatively shallow cavity but it articulates with the head of the humerus
to form a ball and socket joint the ball is formed by the head of the humerus the socket is formed by the glenoid cavity and in order to deepen this glenoid cavity there is a fibrocartilaginous ring known as the glenoid labrum that is sitting around the circumference of this glenoid cavity the clear oi cavity is somewhat deepened by very clean oil labrum and it adds an element of stability the design of the ball and socket joint the glenohumeral joint of the shoulder joint proper is for mobility and you will observe that the shoulder joint has
a very great range of movement but inherently it is also unstable because of the fact that it's designed for mobility rather than stability let's now proceed to our next slide and add back the clavicle that we had removed as well as the sternum and we can now look at the joints that we talked about so this is the clavicle here it's a long bone and is fairly unique in in many regards what is relevant here is that it's a long bone that sits horizontally rather than in this in its vertical orientation which many other long
bones are positioned in such as the humerus which is also a long bone and it sits in the anatomical position in a vertical alignment the glenohumeral joint which is the joint that we just described between the head of the humerus and the glenoid cavity is seen here and that gives us our orientation for the remainder of this slide if we focus on the medial end of the clavicle it articulates with the manubrium which is the superior part of the sternum and it forms another joint known as the sternoclavicular joint this is also a synovial joint
like thinking a humeral joint but it is a very stable joint it's bounded by ligaments and capsule and it's in fact the only real articulation real joint between the entire upper limb and the axial skeleton the rest of the upper limb is attached to the axial skeleton and the axial structures by soft tissue sternoclavicular joint is truly the only bony articulation between the entire upper limb and the axial skeleton so it's a strong joint and has tremendous capacity for four load-bearing the lateral end of the clavicle is also in articulation with the bony structure that
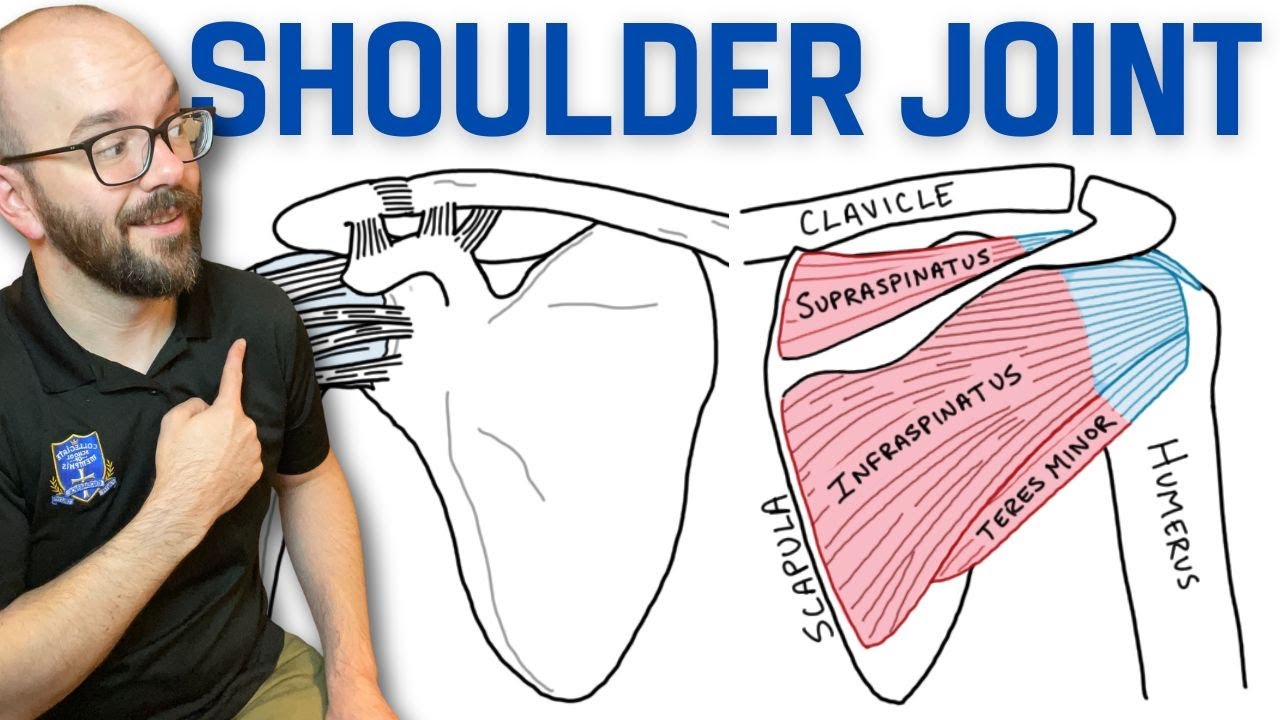
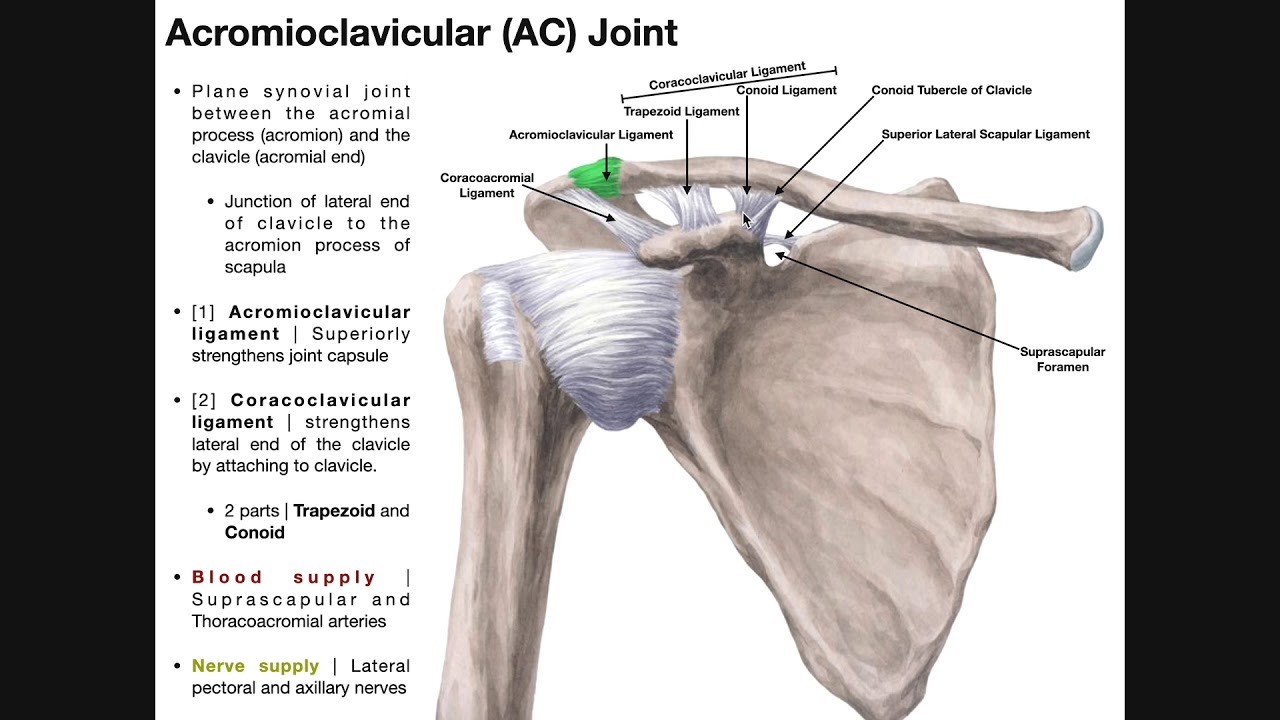
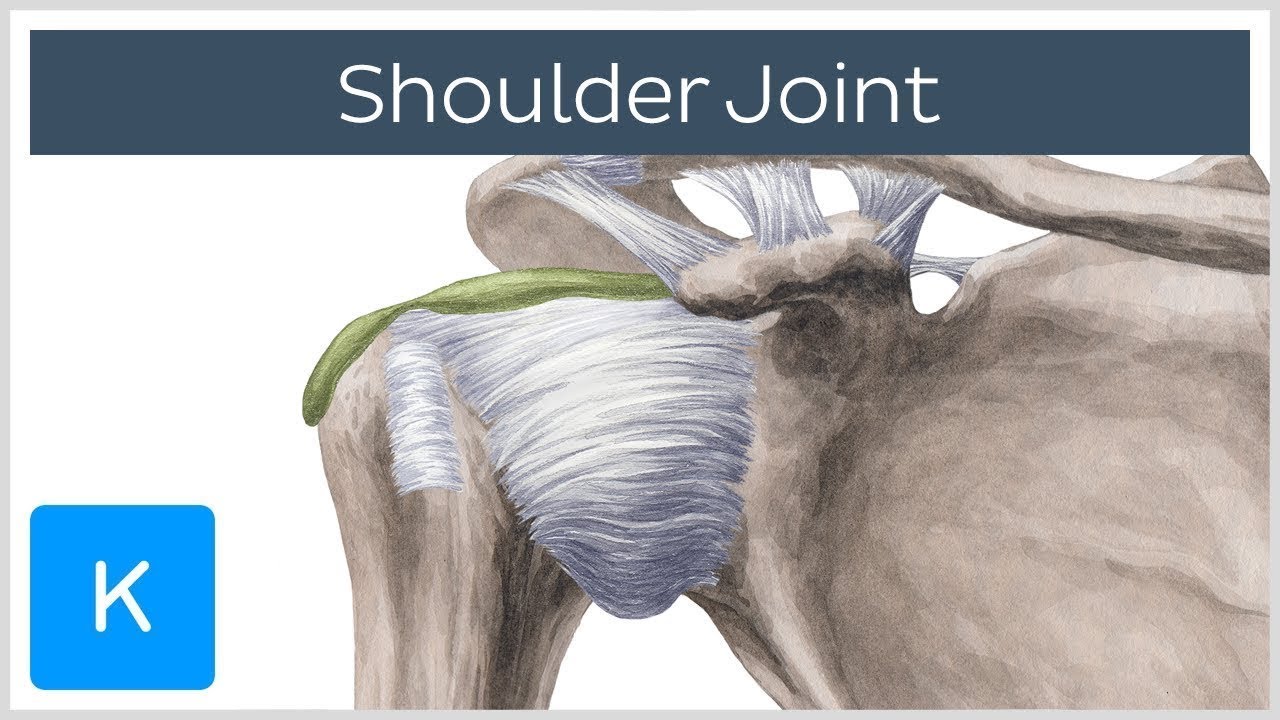
we just looked at the acromion process and forms the acromioclavicular joint this is a joint that is often dislocated in sports injury or other forceful trauma around the summit of the shoulder and the word that is often used for this is called shoulder separation this is very different from a true shoulder joint dislocation of the glenohumeral joint which is also a very common injury that is seen clinically in addition to these formal joints there are a couple of loosely called joints that are not truly joints but in clinical practice often the word joint is used
to describe these structures and one of those is just belief or inferior to the acromion known as the subacromial joint and note that we have put joint within course it's not really a joint it's the subacromial space and it has important structures in that in that space such as the rotator cuff and synovial cavity is like the like a bursa and it's often the seat for chronic shoulder pain and so it's an important anatomical structure that we need to be able to identify from a functional standpoint the blade of the scapula forms an articulation or
a joint again loosely defined known as the scapula thoracic joint where the blade of the scapula rotates around the rib cage itself and this provides for a fairly significant amount of movement of the shoulder joint itself so if you think about the shoulder joint the glue the humeral joint is the ball and socket joint which is this the stroller joint proper but these other joints around the glenohumeral joint particularly the scapular thoracic joint participates in the movements of the shoulder joint and about one third of total movement occurs at these additional joints only about 2/3
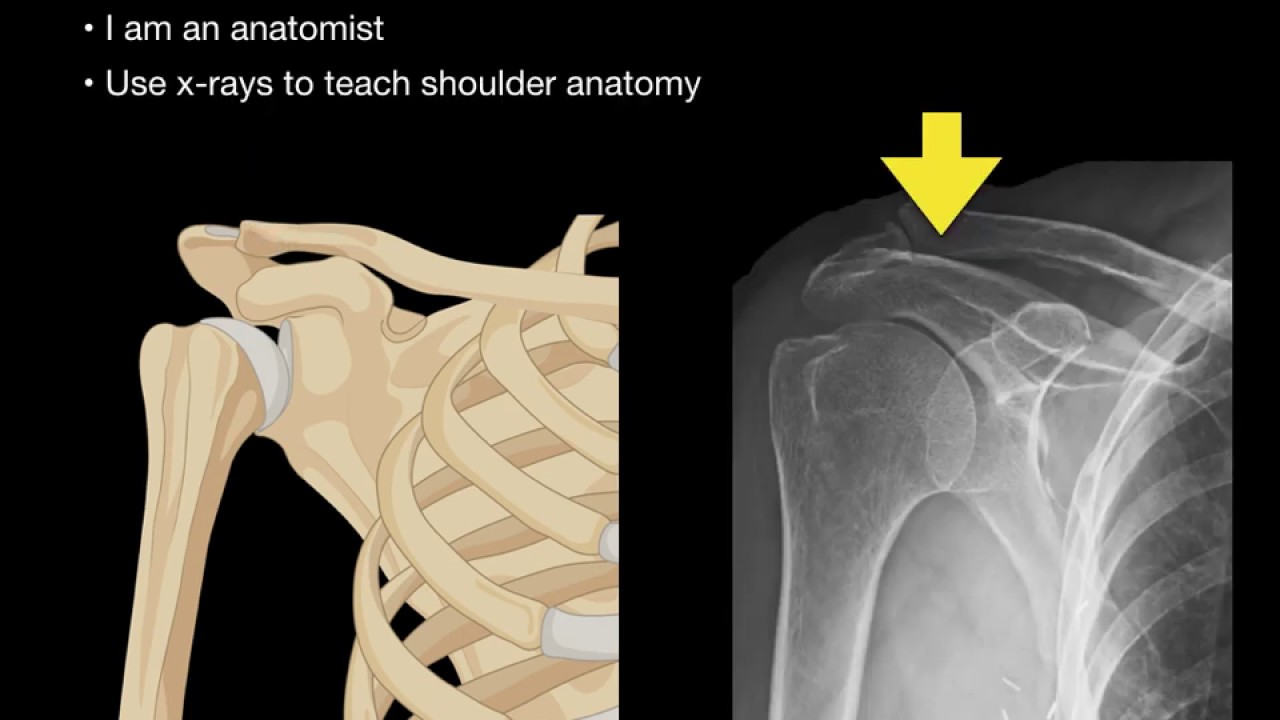
occurs at the little humeral joint so let's look at a simple ap or natural posterior view x-ray of the right shoulder area and we can identify certain structures in this film the first one is the sound head of the humerus and I'm going to outline it like this so this is the head of the humerus and it articulates with the glenoid cavity which is shaded in here so this is the glenoid cavity and this forms that ball and socket joint or the glenohumeral joint or shoulder joint proper there are other structures that are also visible
the first one of those is the long bone that we have looked at earlier the clavicle and I'm going to outline that bone here in its entire course so this is the clavicle and note that its lateral end is articulating with the acromion process as we just looked at in our line diagram and I've outlined it here and so this is the acromion process and that forms the acromioclavicular joint there's one other structure that we can see the coracoid process which is outlined here in red and this is that bony beak like projection from the
scapula just below or beneath or inferior to the clavicle so these are some of the structures that we can see in a simple plane film of the shoulder joint and this is an ant or post year or AP view if we look at another x-ray same view same right side shoulder joint it looks a little different and so let's trace out some of the structures that we've already looked at and identified in the previous diagrams and so we have the scapula here the head of the humerus we can see the hemispherical head of the humerus
outlined here and the glenoid cavity is shaded over here and you will instantly note that unlike the previous x-ray where the head of the humerus and the glenoid cavity where articulating with each other congruently in this case the head of the humerus in the joint cavity appear to be away from each other in fact they are overlapping each other the glenoid labrum is in this location but it is not visible because it is fibrocartilaginous but it is at the margin of the glenoid and we can estimate that this would be the location of the glenoid
labrum this is an x-ray of a dislocation of the glenohumeral joint and classically described as an anterior or more accurately an antral inferior dislocation whenever we talk about dislocations of joints the traditional way in which they are described is the dislocation of the distal fragment in relationship to the proximal fragment so the head of the humerus which is the distal fragment if this joint is anterior and inferior to the glenoid cavity and hence this will be called an Antero inferior dislocation [Music] you