hey everyone Dr J Cody and in this video I'm going to be breaking down some research that I was involved in uh This research was mostly done by Michael Daniels and it was done in the David broth and Catherine Lawrence research group at the University of Manchester now in the previous few videos I've sort of been building up to this paper I've been explaining the theoretical background behind this paper as well as some of the techniques that go into this paper and then the next few videos I'm really going to thoroughly break down this paper
so the title of the paper is fenimate NSAIDs inhibit the nlrp3 inflammasome and protect against Alzheimer's disease and rodent models if all of that is gibberish please go back and watch the previous videos because you should just from the title know where this is going so let's jump into it first I just want to quickly skim over some of the essential background for the paper how did we come up with this hypothesis and why did we essentially pursue this research in the first place so first up yes neural inflammation is happening during this form of
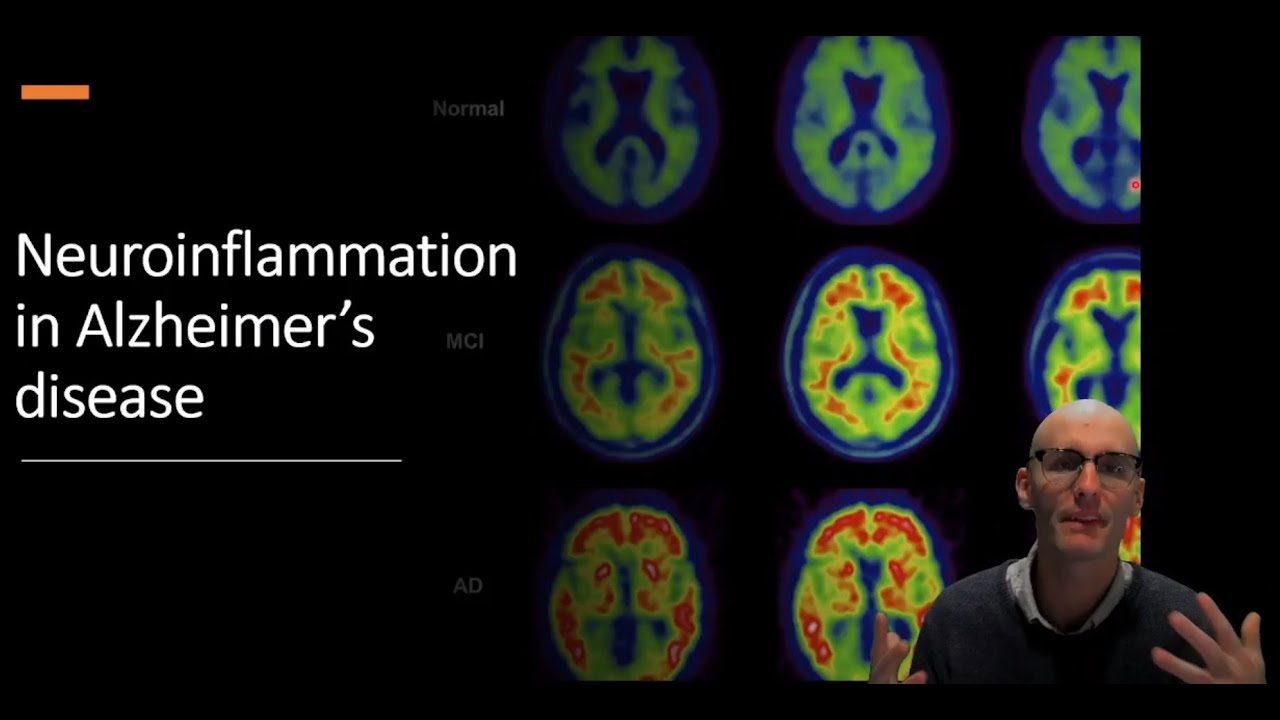
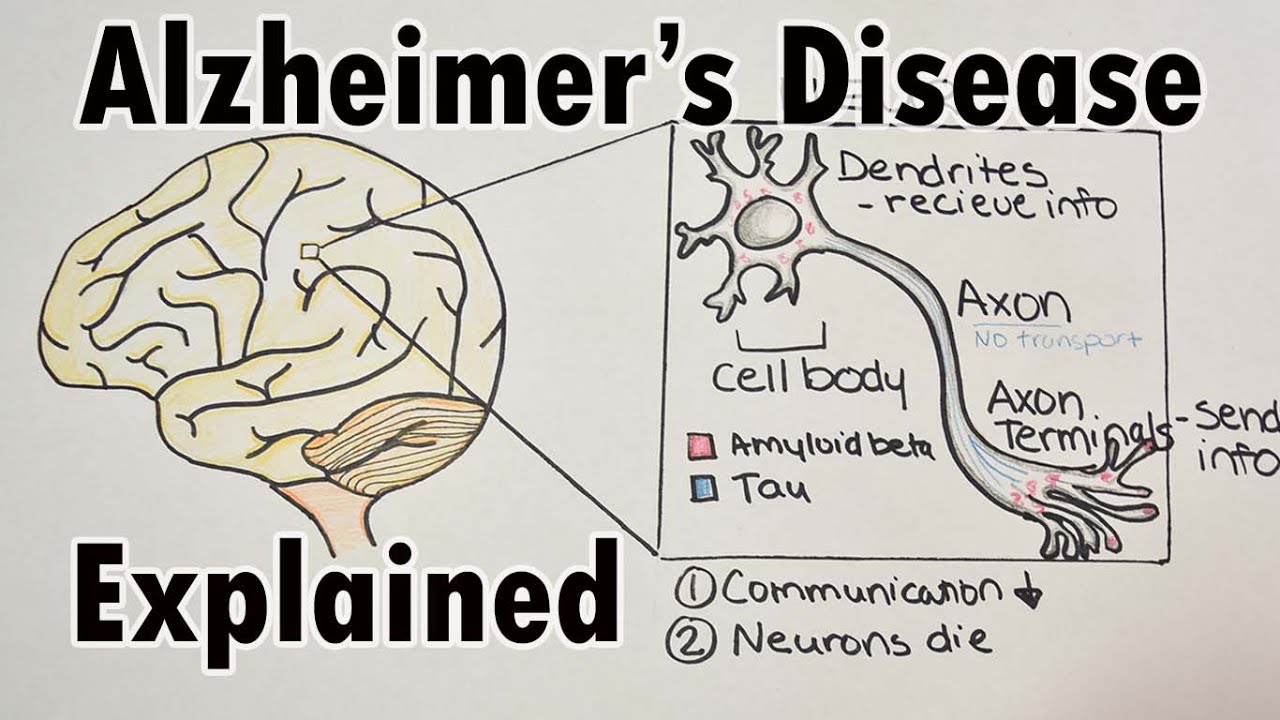
dementia known as Alzheimer's disease in which you get memory deficits followed by cognitive deficits language deficits intervention motor deficits and death now we can track neuroinflammation in the brain using pit Imaging which we put a radio label to tag into the bloodstream and it binds to a specific thing that we wanted to bind to and in this case we're binding it to activated microglare so here we can see in an Alzheimer's brain we've got activated microglia we've got inflammation whereas in a healthy control brain we do not have inflammation going on now this inflammation is
mostly clustered in little zones around the brain and an Alzheimer's disease is clustered around amyloid plaques so in green here we have the amyloid plaque and in red we have these activated inflamed microglare and yellow you can see little chunks of amyloid being eaten by the microglia now we know that this activates the microclear and causes inflammation but one of the weird questions is when it comes to sort of fibrilla or amyloid what receptor could it be working through because it's not very soluble and the answer is it's this uh receptor complex that sits in
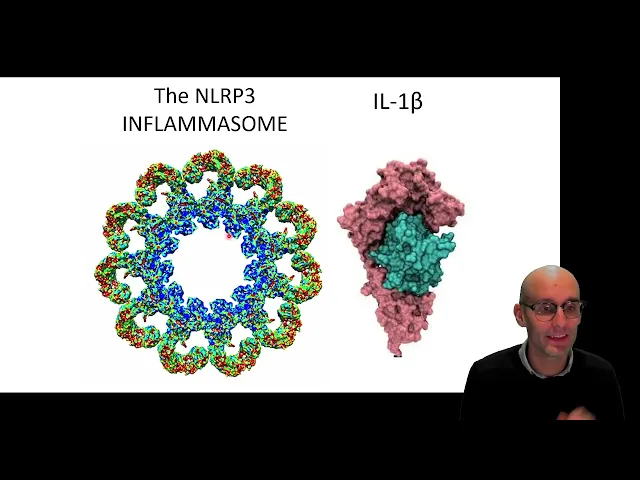
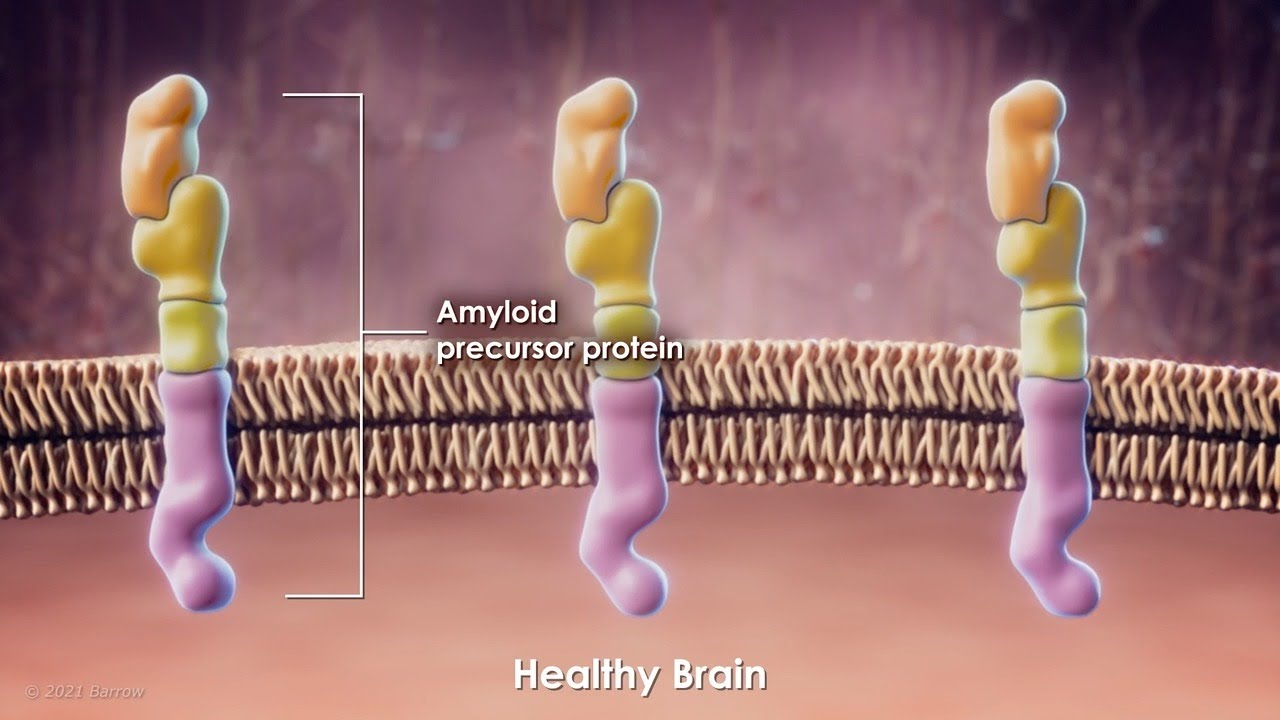
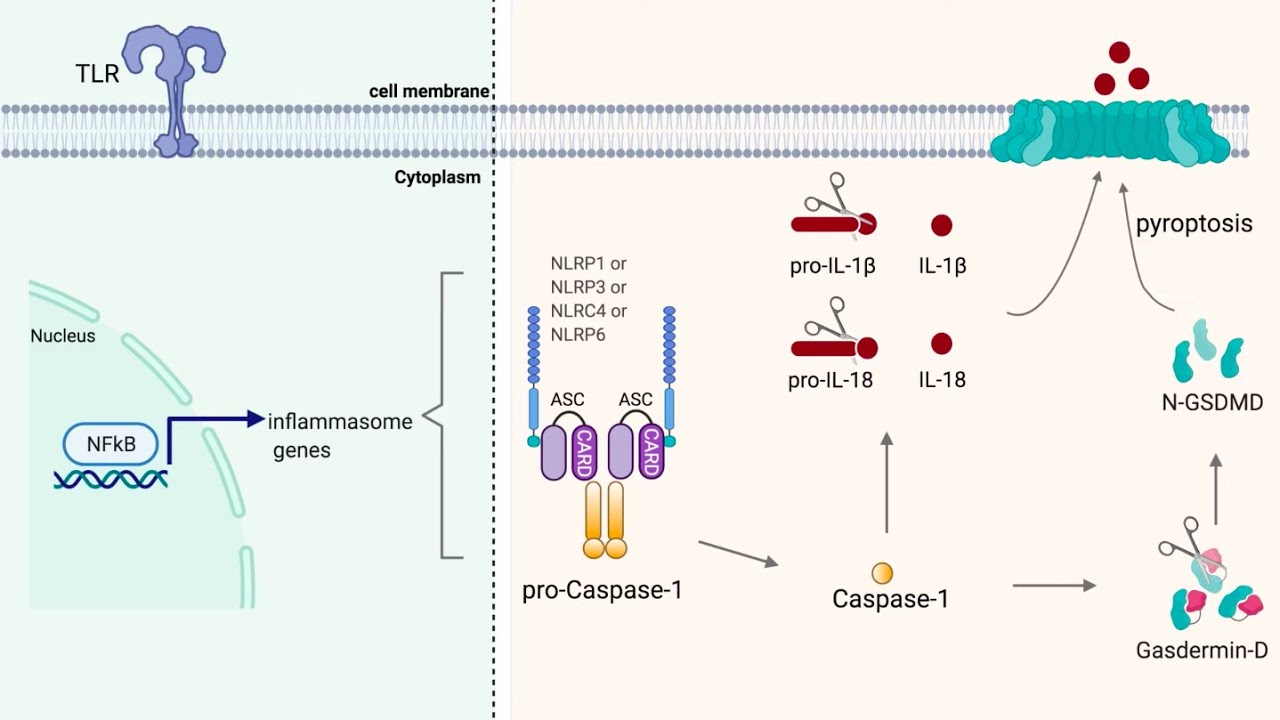
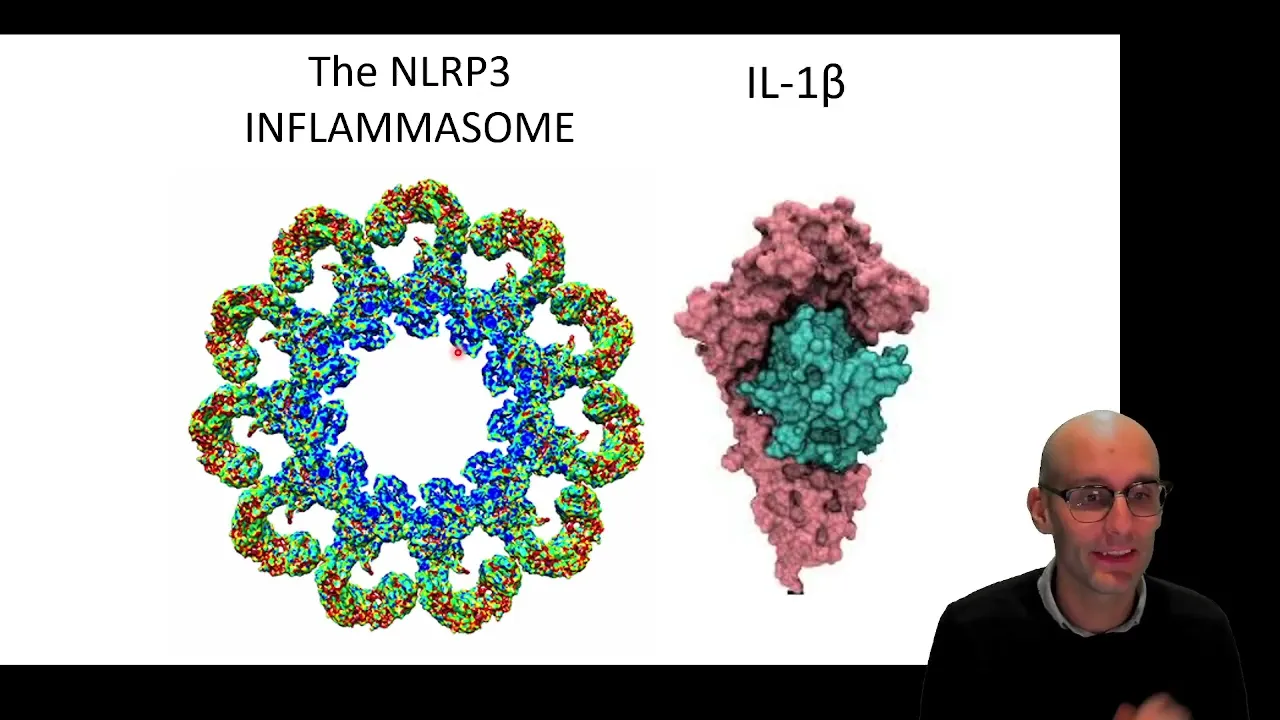
your cytosol called the enlar P3 inflammazone now here it is here it's absolutely beautiful and what nlrp3 does is it activates when there's a perturbation in the cytosolic fluid and it causes the release of mature active interleukin-1 beta here's in the local One beta nestled into the interlegal One beta receptor it's a very inflammatory cytokine now we know that this pathway is involved in Alzheimer's disease this is a very complicated image but I do do a step-by-step breakdown in a previous video but essentially here we can see amyloid which is various amyloid species which is
one of the quintessential markers of Alzheimer's disease where he monomers oligomers and februles they all contribute to this enlarp3 pathway we get activation of tlr4 and tlr6 receptors to cause the expression of pro-ir1 and the expression of nlrp3 then we get frustrated phagocytosis this is a lysis of the phagol lysosome which ultimately causes potassium and chloride efflux which activates the inflammasome the inflammasome then activates caspase-1 that Cleaves Pro interleukin-1 beta into the mature interleukin-1 beta which is then released and we end up with inflammation going on previous research which I've touched on is those signaling
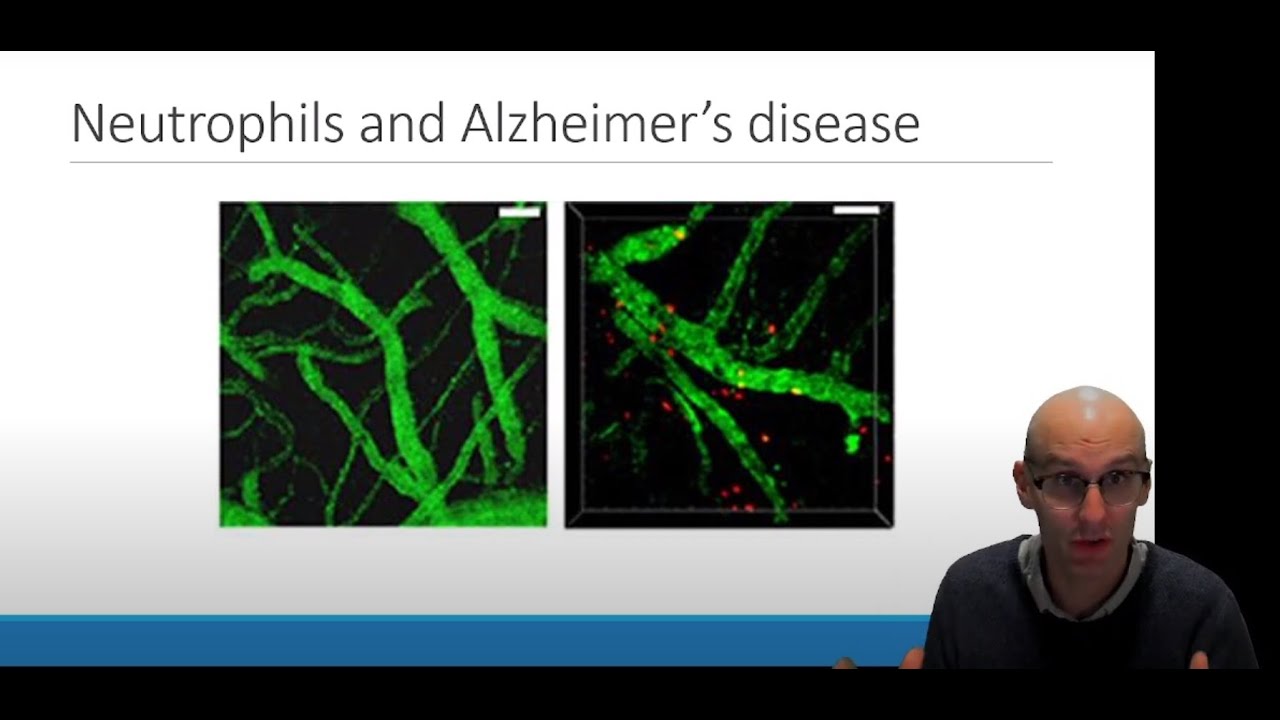
molecules intelligent One beta can lead to neutrophil infiltration activation causing production of toxic chemicals such as bleach in your brain which you can imagine if that's occurring for 20 years um between your 50s and 70s that's going to start to cause cognitive deficits through neuronal death okay so then there was this very similar paper by hinika um coming out of the golombok group uh we're very talented lab produced some huge papers um and in this paper they crossed an nlrp3 knock Mis a mouse with no inner rp3 receptors in them with an Alzheimer's Mouse and
after two generations you can end up with wild type mice in lrp3 knockout mice AP Alzheimer's mice and Alzheimer's mice within nlrp3 knockout they then looked at their memory using the Morris water maze so here we can see and I've explained this all previously which is why I'm zipping through it here we can see that wild temp mice can be trained to find a a location of a platform in a swimming pool so the dotted line is the trace of a mouse swimming in a pool and they can find where that platform is they can
be trained over several days and Alzheimer's Mouse cannot remember the training that it's had for the previous five days so it cannot find that platform and it just swims around and around in circles however in Alzheimer's mouse with an inlrp3 knockout so they cannot induce that inflammatory response to the amyloid pathology that's going on in their brain they are protected from these memory deficits and they can remember where the platform is so all of this background this this concept that we now know that inflammation is going on and Alzheimer's disease it can predict how fast
your cognitive decline is it's mediated by the enolip3 receptor leads to the central hypothesis factors which influence nlrp3 activity and subsequent interleague 1 beta secretion will affect Alzheimer's disease progression now for about five years of my life I researched this from a couple of different angles one was can we inhibit nlrp3 as a therapeutic Target for Alzheimer's disease and are there environmental factors that can sensitize nlrp3 that accelerates Alzheimer's disease now this paper that I did with Michael Daniels and David Braff and Catherine Lawrence and a number of other collaborators really focused on this hypothesis
can we inhibit nlrp3 as a therapy for Alzheimer's disease and this is what I'm going to jump into over the next few videos so first up let's jump into this paper what do we do well what we actually did was is part of a little bit of a broader project we screened a whole bunch of existing drugs that are out there currently used in the clinic and in the pharmacy to see if any of them inhibit in a lrp3 um and so one of the advantages of this is that it means that we know the
safety profile we know if it can be given to 80 year olds nurse and effectively and you have a bit more of a streamlined Pathway to clinical relevance compared to trying to develop a brand new one and then finding out perhaps it's toxic for the liver if we try to develop a brand new one maybe we would get these unwanted side effects so we wanted to see if existing safe drugs could inhibit the unilrp3 inflammazone and we actually looked at a whole bunch of different classes like I can see tricyclic antidepressants there and here we
have the insides but um yeah so we we we actually tested loads of drugs we used to just go to the drug cabinet on a Friday and and just start screening you know I was a Friday afternoon experiment would start to screen you know maybe a dozen drugs on a Friday and we would do this over several weeks just to see where we could go and what we actually found was some really interesting results around the inside so these are non-steroidal anti-inflammatories that inhibit Cox enzymes to inhibit the production of prostaglandins and so they're all
really anti-inflammatory it already just so happens that these guys are anti-inflammatory through the prostaglandin pathway however the prostaglandin pathway doesn't seem to be that important in Alzheimer's disease has already been several clinical trials on these drugs that inhibit prostaglandins and they've been shown to not affect Alzheimer's disease progression so do a couple of them though however that haven't really been thoroughly tested Alzheimer's disease do they also inhibit inlrp3 so essentially we know non-steroidal anti-inflammatories do this they inhibit the production of prostaglandins do they also inhibit the release of interleukin-1 beta the inflammatory cytokine that's what
we were doing so here's how we did the drug screen and these were done in 96 World plate so you could you could ts96 but normally um because to allow for standards and all this kind of stuff we would normally test 80 different drugs and we might actually do multiple doses so we might actually test 20 drugs at four different concentrations in a plate on a given an experiment maybe a little bit less if we wanted to do five different concentrations for example this is roughly how we did it we plated up macrophages so even
though these are microglia they have very similar enlar P3 responses and so it's a much easier and higher throughput to do experiment using macrophages and then go on and validate them in microgreen so we took macrophages we treated them with lipopolysaccharide LPS it's a bacterial toxin it activates the tlr4 receptor so we know we're going to induce the expression of pro into Luke and One beta and in a rp3 we then treated them with ATP so this is extracellular ADP ATP shouldn't be in the extracellular little space and so this is modeling a damage Associated
molecular pen ATP and then we would give it either an hour or four hours depending on the stimulant sometimes two hours we would measure the interleukin-1 beta coming off and so in this way we could screen a lot of drags it's not really in an Alzheimer's relevant there's not really Alzheimer's specific this model but we're just looking for some generic innerp3 activators and seeing if we can inhibit the enlar P3 inflamazone so then we could test a large number of drugs now ATP binds to this receptacle p2x7 on the surface of these macrophages which opens
up a pore which allows potassium reflex so you can see the potassium leaving and this as we can see over here potassium reflux is a major trigger of venal rp3 um Activation so if we activate a receptor called p2x7 with ATP we will cause potassium efflux now you can see that this is a fantastic thing for an immune cell to be able to do if this is a macrophage and this is a regular tissue cell and let's say this tissue cell gets infected with a virus and this is a lysis virus So eventually the cell
fills up with viral particles and explodes it's now going to release its ATP at very high concentrations now ATP is not normally outside the cell so now the ATP is going to be instead of being inside the cell it's outside the cell and it can act as a damage Associated molecular pen triggering interleukin-1 Beta release from this macrophage right beside it using its p2x7 receptors so it's a very clever technique excellent way to do a drug screen and so this is from figure one in their paper here we've got uh silicoxide these are all non-steroidal
anti-inflammatories here's ibuprofen here's diclovenac his flu phonemic acid mycophenemic acid and methanamic acid and they're all given at different concentrations and we've got io1 Beta release and it's expressed as a percentage of control or a percentage of zero drug um being applied and so basically if it ever drops reasonably below this 100 dotted line that means we've got some level of inhibition so you can see the Covenant does some inhibition but really these are the stars flu panamic acid michelofenamic acid and mefenamic acid are all exceptional ad inhibiting the phenyl rp3 we were very excited
at the 50 micro molar Mark we would have liked it at lower concentrations but 50 micro molar is actually clinically relevant um it gets up to around about 75 micro molar in the blood after you take these drugs okay so um next you can look at the chemical structures and see that Meatloaf phonemic has a diclofenac and flu phonemic acid all have similar structures they have these two rings here joined by a nitrogen molecule and ibuprofen that structurally dissimilated had no effect on annual rp3 very cool so suggesting that there's something unique going on in
this effect must be separate from the Cox enzymes and the prostaglandins because ibuprofen also inhibits the Cox enzymes the mechanism of action how these drugs are working can't be Cox dependent which is very very interesting okay now there are a lot of Pathways to activate the inflamasome I've just got a few of them here so reactive oxygen species and phagol lysosomal rupture and there's a few receptors on the cell that can all lead to enoliv3 inflammozyme Activation so an important question is we know that inhibits ATP which goes to the p2x7 we know that these
drugs inhibit this pathway but perhaps they're just inhibiting the p2x7 receptor so why don't we look at a different pathway just to check to make sure that it's an inflammasome inhibitor and not the p2x7 receptor inhibitor so that's what we do and we actually look at crystals that look just like this and so that's the next experiment that we jumped into and for this we use these things called urate crystals now this is actually a segment of tissue from someone with gout and in gout perhaps their kidneys aren't working very well perhaps they have a
high nitrogen diet and they get too much uric acid building up in their blood and the uric acid starts to to crystallize it's a little like if you put too much sugar in water eventually the the sugar will start to crystallize at the bottom of the dish essentially there's a maximum concentration before you start to get crystallization and these crystals look extra cool because they do funky things under polarized light so this is the tissue is viewed under polarized light so you can see yellow and blue crystals and these are uric acid crystals these are
all immune cells they look a bit funny because they are they're polarized light but you can definitely see the multi lobes of the neutrophils you can even see some monocytes that may have tried to phagocytose from uric acid crystals so we're going to do the same model we're going to take the macrophages give them LPS and then we're going to give them urate crystals to see if that will activate the inflammazone I mean we know it'll activate the inflamazon we'll see if we can inhibit it with our drugs so again we've got 100 release which
is no drug here's flip phonemic acid which only has 20 percent sort of reduced by 80 the amount of ir1 beta coming out and here we have ibuprofen which has done nothing that's not statistically significant so now we can show that yes it's actually inhibiting multiple different activation Pathways for in lrp3 so yes it inhibits particulates now this strongly points to it being an inflammasome inhibitor rather than just inhibiting specific receptors that do eventually lead to inflammasome Activation so awesome now we know that fluvonamic acid and these other NSAIDs are inhibiting the inflammazone why do
they inhibit all inflamazomes so there are actually multiple inflammozymes I think it's up to 11 now um and here's just a few of the examples here so here's our boy here the inner rp3 inflamasome and it's got all these uh activators here uric acid Alum is a thing that we put in vaccines which does a very similar thing to uric acid and ATP and poor forming toxins they all activate the nlrp3 but there's aim2 now aim two directly binds to DNA but their DNA has to be in the cytosol you should never have DNA in
your cytosol so it's a sign that you've got probably a viral infection that has a DNA genome and so this has been designed to bind to the DNA and activate in response to cytosolic DNA and over here we've got nlrc4 now this responds to flagellin the famous spiral corkscrew-like tail on bacteria so you can see that this one's largely a bacterial inflamazon this one's largely a viral inflammasome and a lot of these are sterile damage so uric acid ATP and Alamo or sterile damage but poor format some bacteria do produce poor forming toxins and so
it is also involved in some bacterial infections so do our insades or a non-steroidal anti-inflammatories also and hit the other inflamasomes or is it selective for the nlrp3 so once again we take macrophages we activate them with LPS and then we either give them flagellum or we give them DNA to see if that if that activates inflamasomes and can we inhibit the il-1 release in response to those stimuli so here we have flagellum now it's going to get into the cytosol so we have to actually transfect it which sounds weird but basically we put it
in a little fat ball that will then fuse with the membrane and then you end up with flagellin in the cytosol and you can see that we get io1 Beta release um and it's not blocked by flip phonemic acid methanamic acid or ibuprofen and we did it again with DNA because that will activate the aim2 receptor and it was not blocked again by our drugs so in other words our drugs work on in lrp3 but they do not work on inelastic four which is stimulated by flagellin or aim2 which is stimulated by DNA now you
might notice here we do have this group here called yvad which has inhibited io1 Beta release in all of these and that's because that's a caspase-1 inhibitor so if we know that in lrp3 pathway the inflammasomes activate the caspase which activates the interleukin-1 beta because all all three of these inflammosomes activate caspase one if we block headspace one it should actually block all forms of il-1 Beta release right so we had this yv drug and that's to confirm that we could inhibit the ir1 beta so this is just a positive control there but very cool
stuff now we know that we've got a selective nlrp3 inhibitor now that's actually good you might go hang on isn't that bad no but if we want to give this drug to treat Alzheimer's disease we don't want it to block The receptors that are designed to detect bacteria or viral DNA we only want to block the receptor that detects the amyloid and that's because we don't want to open up our patients to infection and indeed there have been drugs that block the ir1 signaling molecule from doing its signaling and it did amazing things that reduced
cancer death by 50 and reduced osteoarthritis and gout by 80 and it reduced cardiovascular events by 50 because they are caused by cholesterol crystals and inflammation partly caused by those things which is all amazing but unfortunately we got a massive rise in in fiction because by inhibiting ir1 you're actually inhibiting this pathway flagellin causing il-1b to release or viral infections cytosolic DNA causing ir1 Beta release so by inhibiting io1 Beta or caspase 1 you're opening your patient up to massive infection risk but you're much less so you are still a bad but you're much less
so if you're just inhibiting nlrp3 so this was actually super exciting and awesome news to have our drugs only inhibit the enoliv3 and flammazone so that is all figure one from a four-figure paper and there are actually supplementary figures that I'm not going to go into but that is uh figure one done and in the next video I'm going to cover forget 2.