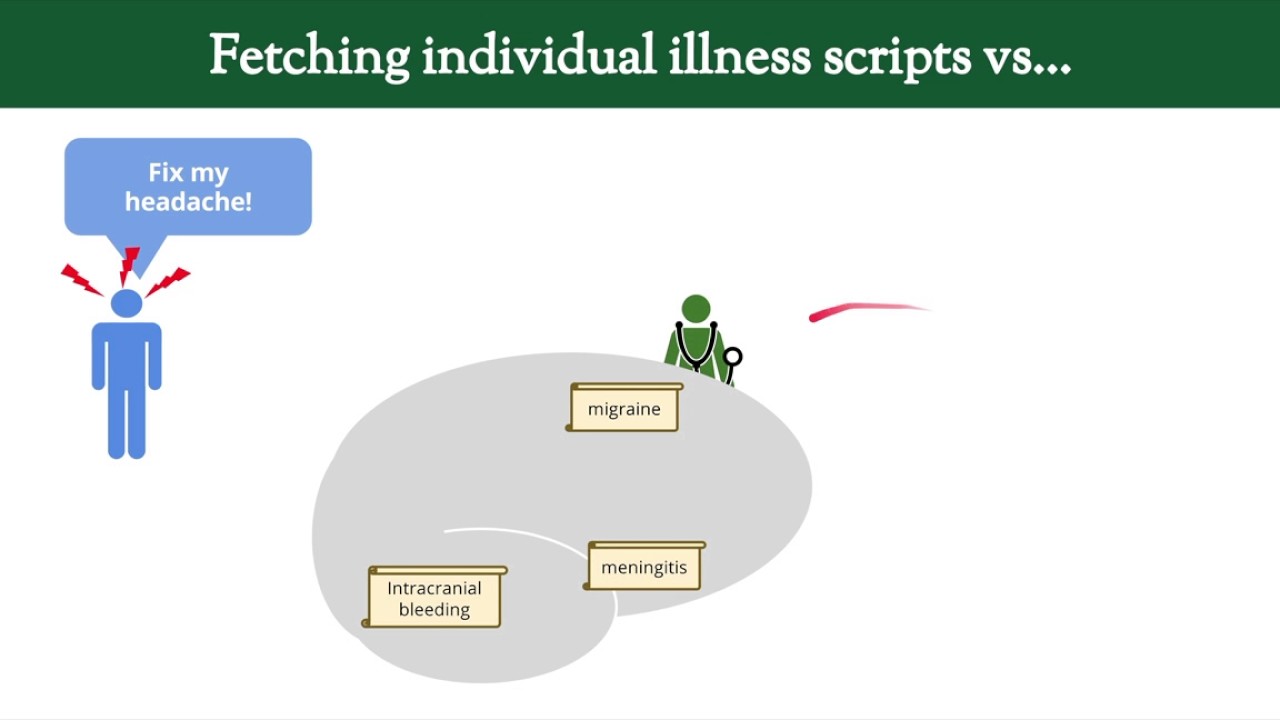
what is an illness script an illness script is an organized mental summary of the clinicians knowledge about a disease it is developed from a combination of reading and personal experience information is categorized such as by pathophysiology epidemiology symptom characteristics diagnostic tests and treatment the complexity of an illness script varies depending upon disease prevalence and clinician experience and the script is updated after each new encounter with the disease to compare diagnostic frameworks to illness scripts a diagnostic framework is structured knowledge centered around a common symptom physical sign or test abnormality whereas an illness script is structured
knowledge centered around a specific disease understand when I'm talking about let's look at an example or actually two examples as illness scripts can be particularly illustrative if used to compare similar diseases I'll compare the scripts for attention headaches and migraine headaches well first focus on tension headaches age of onset is typically 20 to 50 with a female predominance it is overall the most common cause of chronic headaches regarding the clinical presentation they are usually bilateral and symmetric mild to moderate and relative severity lasts anywhere from 30 minutes to 7 days and can be qualitatively described
by patients as a pressure tightness or band-like there are no associated symptoms the diagnosis is clinical meaning there is no specific diagnostic test to roll it in for treatment to abort or stop the headache and said or acetaminophen is used while there is usually no preventative treatment for migraine headaches the age of onset is typically 10 to 40 also with the female predominance and a strong genetic link they usually start as unilateral but can become bilateral the pain is relatively moderate to severe lasting for hours to 3 days and is most often described as throbbing
or pounding migraines are associated with prodrome xin auras and they have numerous distinct subtypes it's also a clinical diagnosis the board of treatments include NSAIDs triptans dopamine antagonists and air goats while preventative treatments include beta blockers antidepressants and anticonvulsants here's another example one taken from my video and approached the syncope I won't run through it line by line but feel free to pause it and look it over it demonstrates how the concept of an illness script is not necessarily only for specific diseases but it can also be applied to syndromes or categories of disease why
talk about illness scripts for many students creating charts that compare and contrast diseases like this it might feel like an obvious thing to do and does not necessarily require a specific name for the concept the most important reason is that cognitive psychologists hypothesize that scripts represent how people actually remember and process information let's take an example imagine the patient Sam a seven-year-old boy who presents to the pediatric clinic with an intermittent call for three months any physical exam notable only for mild bilateral wheezing how do we figure out what's wrong with him well if you
had just watched my video on an approach to cough maybe he would recall this flow chart and work through it but probably not unless you repeatedly use the same flow chart over and over again our brains are just not good at using them from memory what you would do instead is compare Sam's presentation to your mental summaries of diseases that can cause a chronic cough diseases that you recalled from the conscious or unconscious use of the relevant diagnostic framework for example you might think about upper airway cough syndrome commonly referred to as post nasal drip
this is a common diagnosis but predominantly occurs in adults not 7 year olds has nasal discharge which Sam is not reporting and is associated with the physical exam findings that we don't see here next you could consider GERD or gastroesophageal reflux disease another common cause of chronic cough on that illness script you'll see that it's typically seen in adults but can also be seen in kids but it's associated with a sour taste in the mouth and it's worse at night and with lying down none of which Sam describes and isn't associated with wheezing so while
this script matches Sam's case a little better than the previous one it's still not great finally you could consider asthma as most typical onset is in children Chuck and it's associated with wheezing Chuck this script seems to fit the presentation much better in the interest of time this example of diagnostic reasoning was extremely simplified in real life we would be considering many other features of the presentation and comparing those to the rest of the scripts and we would be considering more than three scripts for a typical patient presentation experienced clinicians will do this during the
bedside encounter itself in which they will compare each response during the interview to their illness scripts update probabilities of diseases in real-time and then use those updated probabilities to inform what question they should ask next and what components to include in the physical exam this is predominantly done subconsciously now let's consider what is the most important information to keep on an illness script to answer this we'll need to revisit the concept of key features to remind you key features are individual elements of a presentation which are likely to help differentiate one possible diagnosis under consideration
from another imagine for example that we have a patient presenting with a symptom or exam finding that will represent with this star and this symptom or sign will guide the choice of diagnostic framework from which we will pull several possible diseases and the illness scripts for comparison these diseases are composed of sets of presentation features some of which overlap with others and since the diseases were all pulled from the diagnostic framework for whatever element is represented by the star the star must necessarily fall where all three sets in the Venn diagram intersect if we consider
that a key feature is something which by definition helps to distinguish diagnostic possibilities if we have a symptom sign or other elements of the presentation which fell here on the diagram which was present in all three diseases under consideration it would not be diagnostically helpful it would not be a key feature at all an element that fell into one of these locations would be modestly helpful since it would help to reduce the probability of one of the diseases but elements that fall here here or here only present in one of the diseases under consideration these
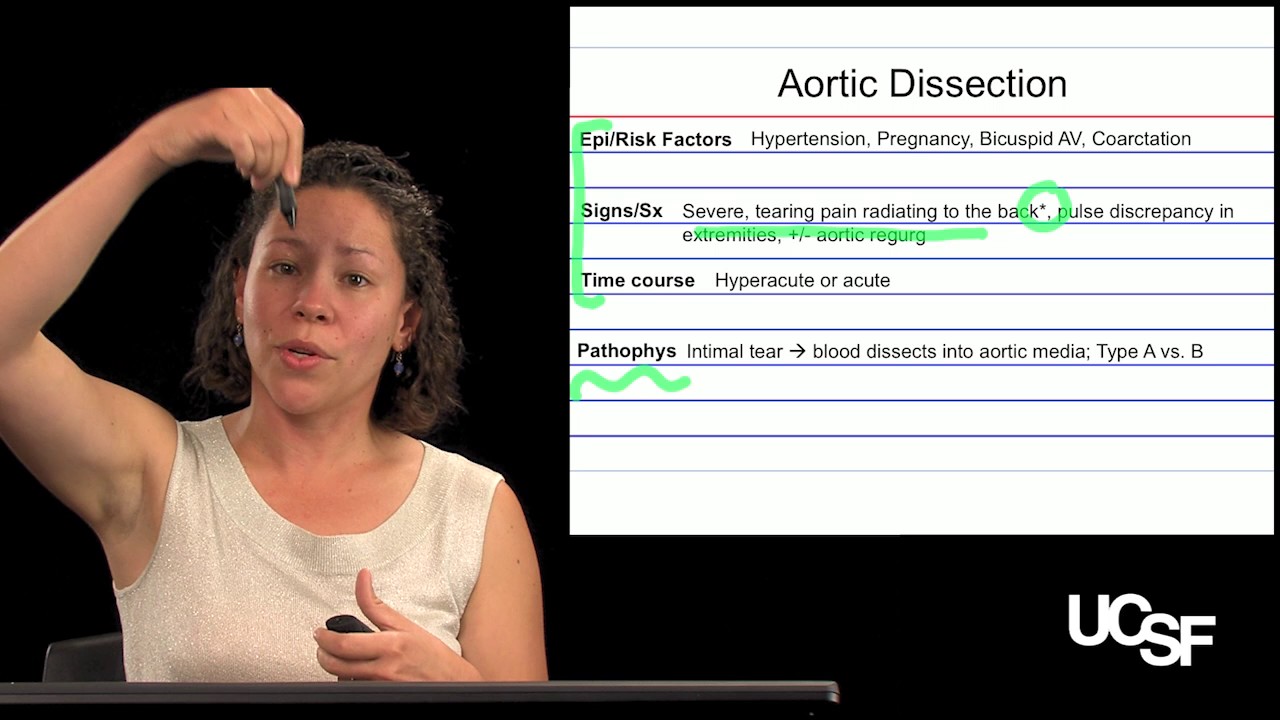
are the most helpful to see what I mean let's consider a specific example a patient presenting with acute chest pain and suppose for this patient for whatever reason we are considering as potential diagnosis acute coronary syndrome a word of dissection and pulmonary embolism all life-threatening conditions where would various potential elements of a presentation fall on the diagram what about hypotension well although the mechanism is different in each condition hypotension can be seen in all three so hypotension in this case is not a key feature and doesn't help here what about cardiovascular risk factors well they
are associated with ACS and aortic dissection but not with Pease so modestly helpful likewise if a patient has concurrent dyspnea that seen with ACS MPE but would be unusual in an aortic dissection so also modestly helpful but chest pain s exertional that's predominantly a feature of ACS chest pain it radiates to the back is particularly suggestive of a dissection among these three possibilities and chest pain that's pleuritic meaning worsens with deep inspiration is characteristic of a PE so while none of these last three findings are truly pathognomonic per se meaning a finding that's only seen
in a single condition they do strongly support one particular condition under consideration so in summary illness scripts are most helpful when they contain maximally distinguishing key features rather than just those that are shared by diseases with similar presentations there's another critically important piece of information that every illness script should contain a very general idea of how prevalent the disease is in different populations you don't need to remember specific numbers just ballpark estimates are usually sufficient so for example knowing that among all patients presenting to the ER with a new onset headache a migraine is many
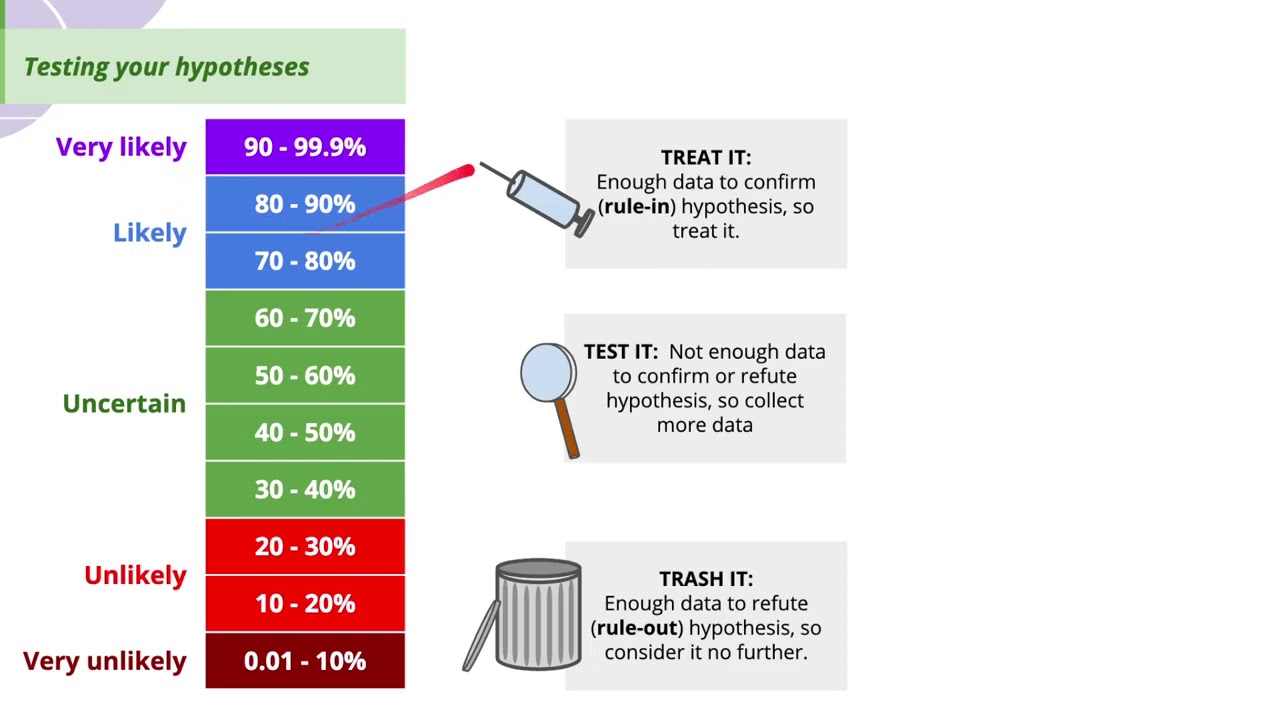
orders of magnitude more likely than a brain tumor or an abscess but among patients who are elderly with a new onset severe headache the prevalence of a tumor is not quite so different than that of migraines and among patients with significant immunocompromised and acute headache the prevalence of an abscess is not quite so different to understand why disease prevalences are so important in diagnostic reasoning consider an analogy that will probably be familiar to anyone who has taken a bio stats class when considering a probability of a disease in a person who undergoes a diagnostic test
the post-test odds is equal to the pretest odds times the likelihood ratio this general concept can be qualitatively applied to illness scripts the probability of a disease in the differential diagnosis depends upon the prevalence of the disease in the population to which the patient belongs and how well the patient's presentation matches the remainder of that diseases in the script in general when considering different diseases that can present with the same symptom there can be a greater variability in the prevalences of those diseases than in the variability in their manifestations what I mean by that can
be summarized in a classic clinical reasoning rule of thumb an atypical presentation of a common disease is usually more likely than a typical presentation of a rare disease it's very common for early learners in medicine to make the mistake of approaching a patient as if all diseases that they've ever learned about in school presents with equal frequency a phenomenon formerly known as base rate neglect for example I might take a student to see a patient presenting with hemoptysis and after seeing the patient I'll ask the students what might be causing the patient's symptom and the
first diagnosis the student suggests is anti GBM disease in autoimmune condition with an incidence of 2 per million people per year and I'll be like okay sure I suppose it might be but it's probably not simple bronchitis lung cancer bronchiectasis and necrotizing pneumonia are all much much more likely a common metaphor is embodied in related but more colorful clinical reasoning rule of thumb when you hear hoofbeats think of horses not zebras since a nearby horse is a much more common explanation for hoofbeats assuming of course that you aren't in sub-saharan Africa however the flip side
is that it's common for later learners and even seasoned clinicians to overcompensate for this and make the mistake of not sufficiently considering rare diagnosis there so called zebras a clinician will never diagnose a zebra if they don't consider it a possibility an obvious phenomenon which contributes to the under diagnosis of many rare diseases overall in illness script is only as good as the information in it when compared to novices illness scripts of experts acknowledge when the classic textbook description of a disease does not match its most common presentation for example most patients with cardiac tamponade
and they present without hypotension unlike what's often described in textbooks scripts of experts include atypical but well described variants of the disease for example an acute MI presenting as dyspnea or abdominal symptoms without chest pain in women diabetics and the elderly and they include a qualitative predictive value for commonly associated symptoms science and test abnormalities like knowing an s3 is a much better positive predictive value than negative predictive value in suspected heart failure the key takeaway points in illness script is an organized mental summary of a clinicians knowledge about a disease based on reading and
experience and update it with each relevant clinical encounter the most helpful key features in a presentation are those which occur in only one illness script under consideration the probability of a disease in a patient's differential diagnosis is dependent upon both its prevalence in the population and how well the patient's presentation matches the rest of the illness script for the disease and illness scripts of experts are distinguished from those of novices by acknowledging differences between text book and real-world presentations incorporation of atypical variants and inclusion of predictive values for commonly observed symptoms science and test abnormalities
[Music] you