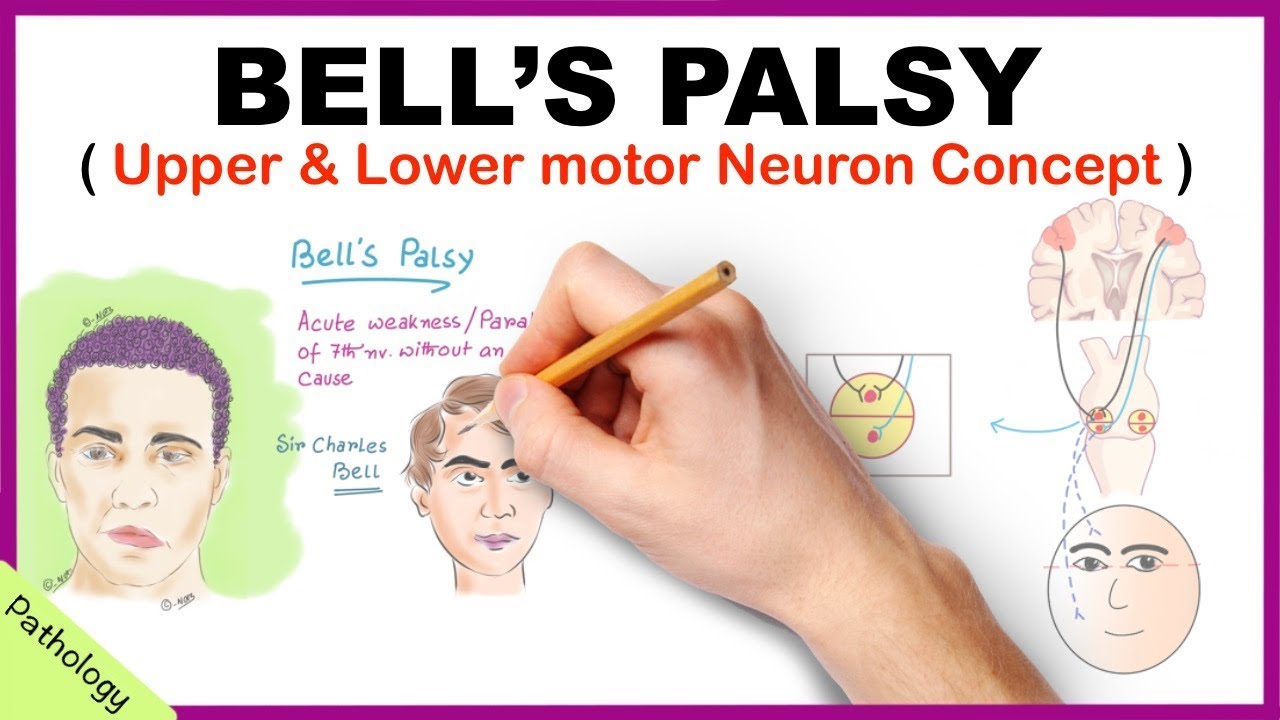
Bell palsy is a condition characterized by weakness or paralysis of the muscles on one side of the face that's caused by damage to cranial nerve seven which is the facial nerve now let's quickly review the anatomy and physiology of facial innervation the 12 pairs of cranial nerves are peripheral nerves also called lower motor neurons that emerge from the brain or brain stem the seventh cranial nerve is the facial nerve which emerges from the brain stem and then enters the temporal bone where it travels through the facial Canal the facial nerve then exits the skull through
a tiny hole called the stylomastoid foramen from there it branches off to innervate different facial muscles that control facial expression ipsilaterally so on the same side the facial nerve also innervates the lacrimal glands as well as the sublingual gland and submandibular salivary glands and the mucous membranes of the nose mouth and nasopharynx in addition the facial nerve also carries sensory information about taste from the anterior two-thirds of the tongue finally the facial nerve innervates the stapedius muscle in the ear which helps dampen loud noises if we look back the facial nerve receives information from a
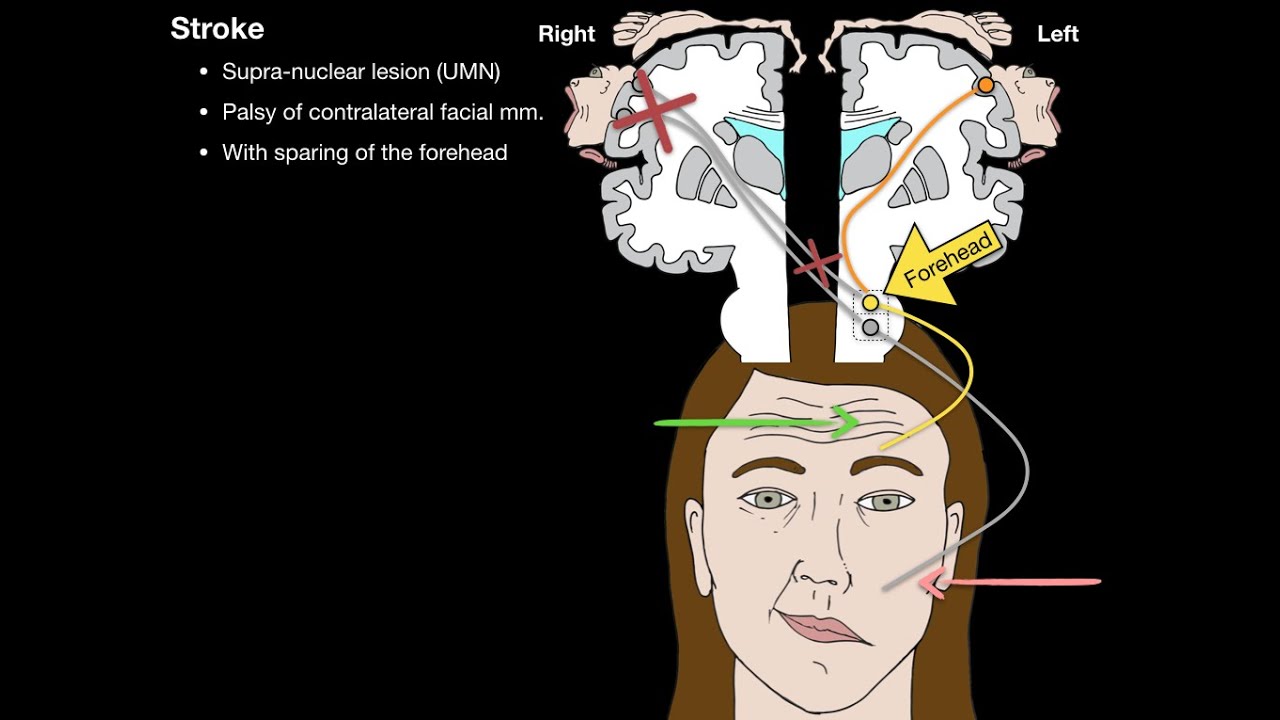
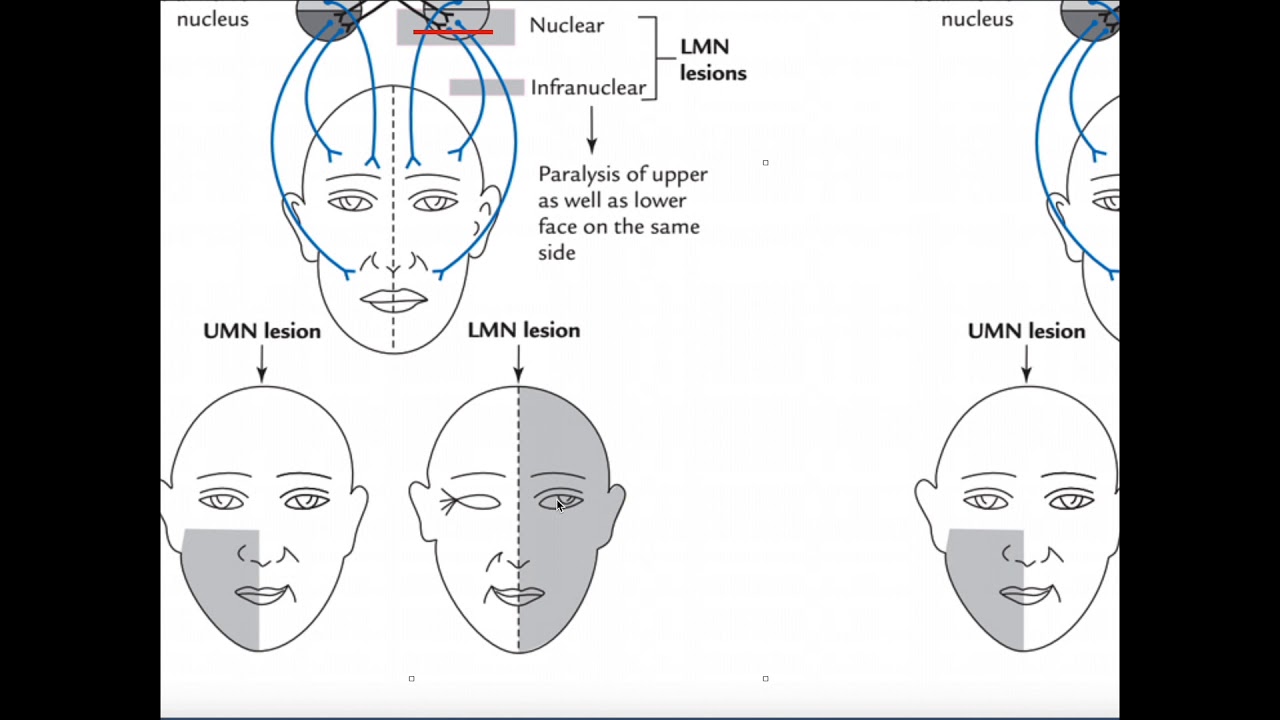
region of the brain called the motor cortex which has upper motor neurons that send information to the brain stem nuclei of the facial nerve and then the facial nerve gives rise to two lower motor neurons one to innervate the lower side of the face and one for the upper side now the lower motor neuron that innervates the upper side of the face receives information from both sides of the motor cortex so both from an upper motor neuron coming from the ipsilateral side as well as an upper motor neuron coming from the contralateral or opposite side
that crosses in the midline on the other hand the lower motor neuron that innervates the lower side of the face only receives information from the contralateral motor cortex so from an upper motor neuron that crosses in the midline now Bell palsy is caused by damage to the facial nerve although the precise cause of the damage is unknown risk factors include history of viral infections such as herpes simplex virus or HSV Epstein-Barr virus or EBV and varicella zoster virus or vzv as well as bacterial infections such as borrelia burgdorferry which causes Lyme disease other risk factors
include conditions like sarcoidosis diabetes mellitus or hypertension so these risk factors seem to trigger inflammation or damage to the lower motor neurons belonging to the facial nerve as a result information from both the contralateral and the ipsilateral motor cortex is lost for the upper face as well as information from the contralateral motor cortex for the lower face this results in the paralysis of all the muscles on the ipsilateral side of the affected nerve now the clinical manifestations of Bell palsy typically begin suddenly and tend to worsen over 48 hours these include mild weakness to total
facial paralysis on one side as well as a unilateral drooping of the eyelid and mouth and disappearance of the nasolabial fold which is the skin fold that runs from the side of the nose to the corner of the mouth clients often experience dryness of the affected eye or side of the mouth a loss of taste sensation on the anterior two-thirds of the tongue as well as some difficulty drinking and eating or difficulty with speech in addition clients often experience posterior auricular pain or pain behind the ear lastly some clients can also develop unilateral hyperacusis where
the ear on the affected side may have increased sensitivity to loud noises now it's important to distinguish Bell palsy from other causes of facial paralysis where the underlying problem is in the motor cortex before the upper motor neurons cross the midline this only causes paralysis of the lower half of the face on the contralateral side of the lesion since the upper half of the face is still receiving some information from the ipsilateral motor cortex the diagnosis of Bell palsy starts with a client's history and physical assessment followed by brain Imaging tests such as MRI or
CT scan in order to rule out a stroke or brain tumor regarding treatment for Bell palsy most cases resolve on their own within six months but some clients May benefit from anti-inflammatory medications like corticosteroids which can help reduce the nerve inflammation and speed up the recovery in some cases physiotherapy can be used after recovery to promote facial muscle control fortunately only a few clients develop permanent facial weakness or paralysis okay let's look at the nursing care you'll be providing for a client with Bell palsy the priority goals of care include managing symptoms and preventing complications
Begin by assessing if your client is experiencing pain and administer the prescribed analgesics and apply a warm moist compress to the affected side to provide some additional comfort and promote circulation then administer the prescribed corticosteroids next assess their eyes and administer artificial tears or ointment to keep the cornea from drying out lastly collaborate with the physical or occupational therapist who may recommend and fit a facial sling for your client to help Provide support improve lip alignment and help with eating finally Provide support for your client regarding their temporary change in physical appearance and encourage them
to express their feelings and anxieties refer them to counseling as needed all right let's move on to client and family teaching Begin by explaining how the disorder affects their facial nerve resulting in the symptoms they are experiencing reassure them that in most cases the condition is self-limiting and that their symptoms should resolve gradually over several months lastly emphasize the importance of keeping all scheduled treatment and follow-up appointments so their progress can be monitored next discuss the importance of protecting their eyes instruct them on the proper use of moisturizing eye medications during the day and explain
that wearing protective eyewear like goggles or sunglasses will help protect their eye from dirt and dust since they may not be able to Blink to protect their eye also let them know that they can close their affected eye manually several times each day to simulate blinking demonstrate how to apply ointment at night to gently tape the affected eyelid shut and then apply a patch at night to protect their eye during sleep instruct them to contact their health care provider right away if they experience any symptoms of corneal abrasion including itching pain irritation and light sensitivity
vision loss or a feeling like there's something gritty in their eyes stress the importance of keeping their follow-up appointments with their ophthalmologist to monitor their Eye Health also be sure to teach your client about strategies for managing pain and discomfort recommend they apply moist heat to the affected area to promote circulation as needed and take their prescribed analgesics and corticosteroids as directed also review changes they'll need to make while eating teach them to chew on the non-affected side of their mouth to prevent food trapping and advise them to choose soft foods that are easy to
chew emphasize the importance of maintaining good oral hygiene after every meal to prevent cavities periodontal disease and perotitis remind them to maintain their scheduled dental cleanings every six months to monitor for any problems with their oral health finally as they recover encourage them to seek support from friends family or from a support group all right as a quick recap Bell palsy is a condition where temporary weakness or paralysis of the muscles on one side of the face occurs because of damage to cranial nerve seven the facial nerve risk factors include a history of viral or
bacterial infections or conditions like diabetes mellitus and hypertension that can trigger inflammation or damage to the lower motor neurons of the facial nerve signs and symptoms usually occur suddenly and worsen over 48 hours and include weakness or facial paralysis on one side and unilateral drooping of the eyelid and mouth and disappearance of the nasolabial fold clients also often have dryness of the eye or mouth on the affected side difficulty talking and eating and loss of taste diagnosis involves history and physical assessment followed by brain Imaging to rule out a stroke or brain tumor treatment includes
corticosteroid medications to reduce nerve inflammation as well as physiotherapy after recovery to promote facial muscle control priority goals of care include managing symptoms and preventing complications client and family teaching focuses on management of symptoms at home helping current and future clinicians Focus learn retain and Thrive learn more