[Music] hello everyone today I'll be discussing the physical findings of sosis the learning objectives are to identify the common physical findings to explain the basic pathophysiological mechanisms which cause these findings and last to consider test characteristics such as positive and negative likelihood ratios when estimating the probability of curosis in a patient with one or more aention findings the physical findings of curosis can be categorized based upon which of the three major pathophysiological derangements are primarily responsible for them these derangements are first portal hypertension in which increased resistance to flow through the portal Venus system leads
to high pressure within the portal vein second abnormal hemodynamics which manifests as several abnormalities of the vital signs and third a decreased number of functioning hites hepatocytes have a large number of different functions so this category can be further divided into decreased protein synthesis decreased conjugation of B Rubin decreased detoxification of blood and an abnormal balance of the sex hormones let's take a look at one category at a time first is portal hypertension the most avert problem this causes is aites which is collection of fluid in the peronal space leading to Progressive abdominal distension I'm
going to take a small digression to discuss aites in more detail aites is particularly important because it can be very uncomfortable can restrict movement of the diaphragm and thus impair breathing and the acidic fluid can become infected in a condition called spontaneous bacterial peritonitis there are many ideologies of aites with sosis being the most common in the US to understand why sosis causes aites we need to look at something called the Starling equation the Starling equation predicts how quickly and in which direction fluid moves between two compartments based upon the hydrostatic and oncotic pressures of
each as well as the permeability of the membrane separating them in sorosis the relevant values of the capillary hydrostatic pressure which in this case is approximately the portal vein pressure and the capillary oncotic pressure which is primarily determined by serum albumin concentration in sosis the combination of high portal vein pressure and the low serum albumin results in a net movement of fluid from the portal Venus system into the interstitial space around those capillaries which eventually leads back into the peronal space a CES actually has its own set of physical findings independent of the presence or
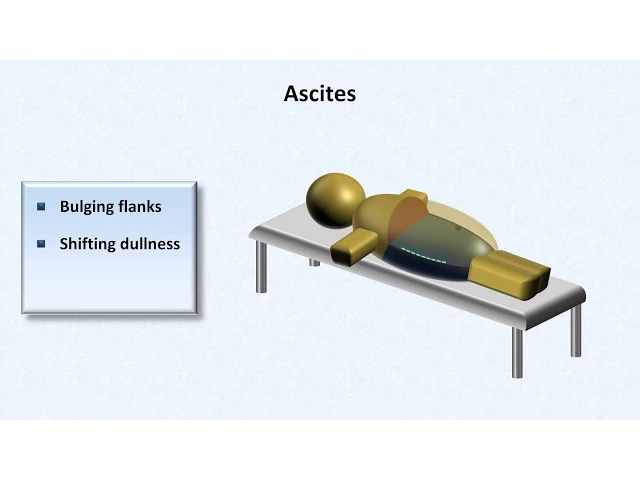
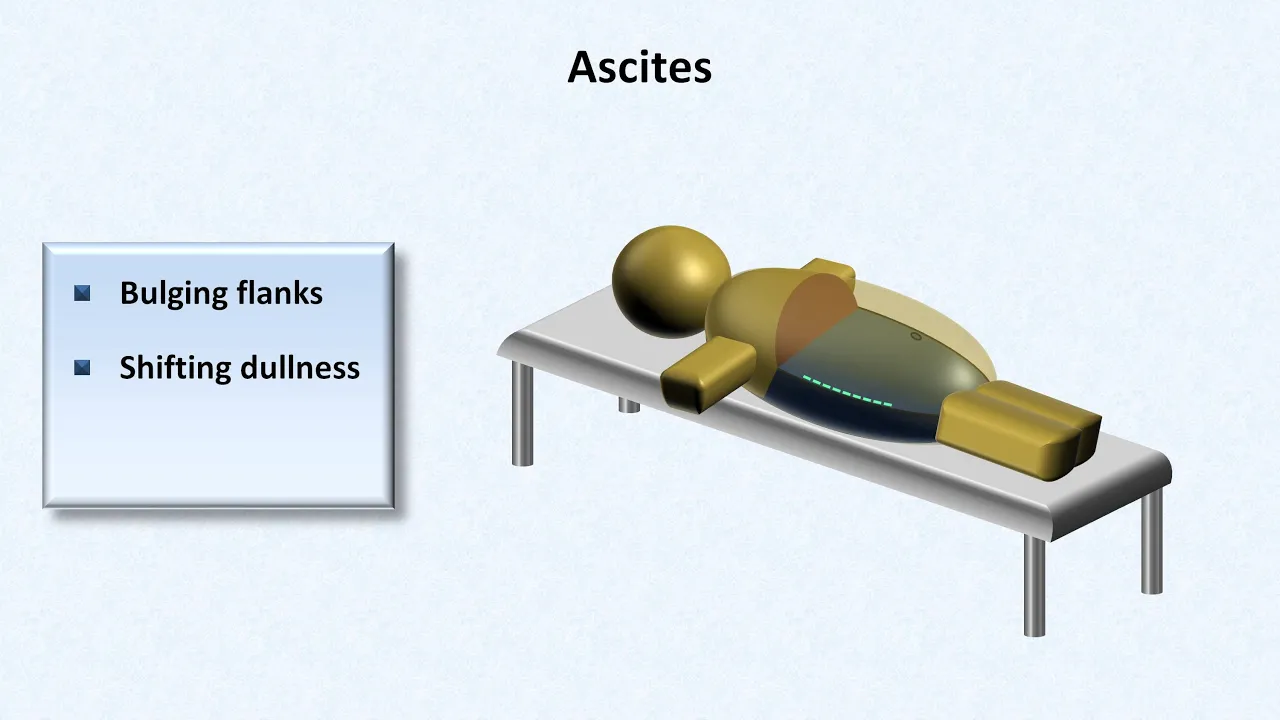
absence of curosis first is an abnormal Contour to the abdomen often referred to as bulging flanks as seen here from Contour alone it may be impossible to distinguish cites from massive bowel distension but it's usually distinguishable from obesity in obesity the adapost tissue is deposited circumferentially around the body the anterior and posterior sides receive roughly the same amount of excess tissue in AES however the pertino cavity only extends posteriorly so far thus the apparent distension only extends so far as well this is difficult to appreciate in the supine patient but it's much easier to see
from the side when the patient is standing another Finding is called shifting dullness to understand how this works let's imagine an exam table on which we have a patient with aites in this case looking a bit jaist now imagine percussing along his abdomen from the midline outward it starts off sounding very resonant and then suddenly there's a transition point where it begins to sound dull why is that imagine what the inside of the patient's abdomen looks like all the acidic fluid which can move around relatively freely under the effect of gravity settles to the bottom
what looks like empty space on top is where the air filled bowels literally float thus percussion above the transition Point sounds resonant and Below sounds dull to know whether or not the existence of such a discret transition is from aites we need to ask the patient to roll onto his or her side and we repeat the same process again now the transition Point relative to external landmarks seems to have moved that's because the acidic fluid inside remains in the most dependent position another finding in the cides is called a fluid wave the technique used to
identify this requires two examiners one examiner places a hand on one side of the abdomen and the other examiner lays his or her hand vertically against the mid line the first examiner then makes a sudden inward motion with one hand and attempts to feel delayed push against the opposite hand as a consequence of a wave passing through the intrarenal fluid the hand on top is meant to prevent movement of the abdominal wall itself from causing a false positive although it's frequently done I personally find the fluid wave challenging to interpret and believe its interobserver agreement
to be low moving back to the other findings attributable to portal hypertension there's lower extremity edema which forms for much of the same reason as aites including a contribution from hypo albuminemia these two findings usually coexist in curosis finding aites in the absence of lower extremity EMA should be a trigger to search for another ideology of the aites such as an intraabdominal malignancy there is also splen omegal though its development may be multifactorial as splenic size does not correlate well with portal pressures I won't review here the techniques used to identify a large spleen other
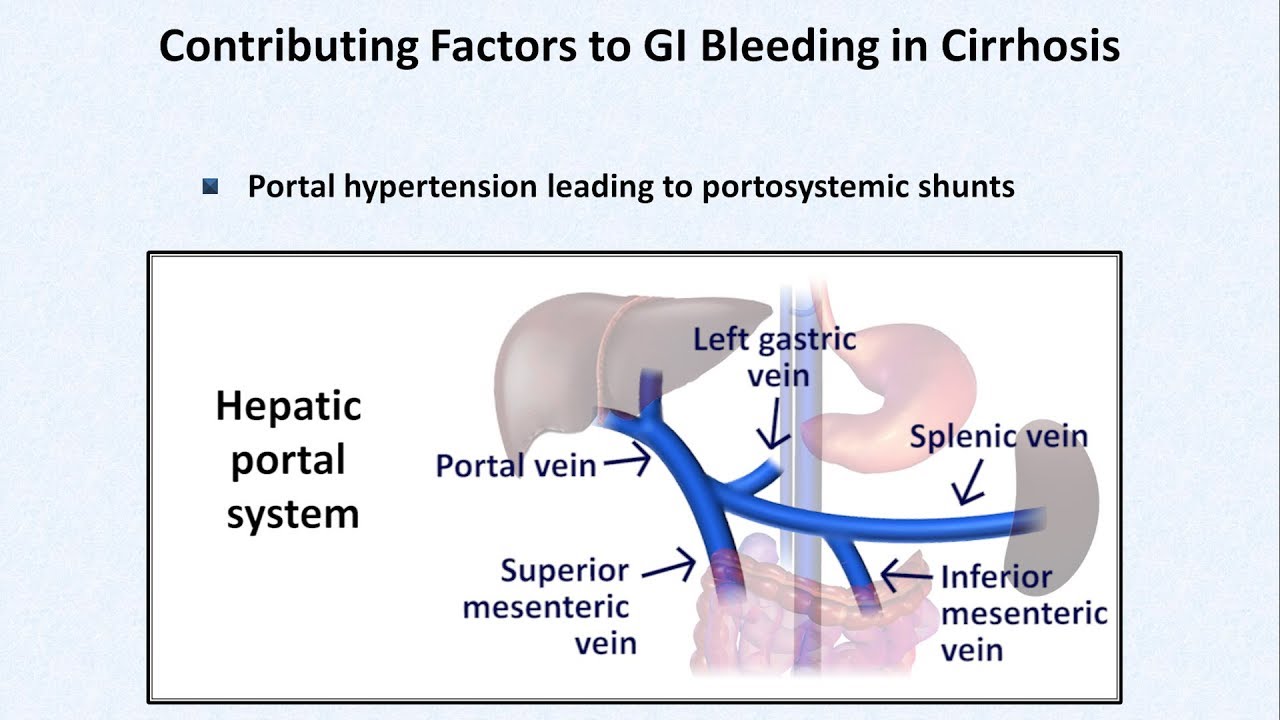
than to point out that palpation for splenomegaly is much more reliable than percussion next there can be prominent Venus collateral formed as blood seeks an alternative route back to the heart that bypasses the portal system these alternative paths are called ptic cable or PTO systemic anastomosis in one possible anastomosis par umbilical veins which usually drain into the portal system and are tiny instead dilate and demonstrate reversal of flow blood then moves from the portal system backwards to the enlarged par umbilical veins to the abdominal wall where visible collaterals are created with theep gastric veins in
its most classic form this finding is called kaput medus or head of the Medusa the monster from Greek mythology the name is derived from the fact that the radially oriented tortuous veins mimic the appearance of the Medusa's snake covered head occasionally the flow of blood through these collaterals becomes so prominent that a continuous Venus hum is audible with oscilation this sound is referred to as the cral here balart murmur though I personally don't like that term because classically the word murmur is reserved for sounds emanating from the heart the creal here balart and hum seems
more appropriate to me so those were all findings caused by portal hypertension let's look at another set of findings the one of abnormal hemodynamics there are three mild to moderate hypotension whereby a typical systolic blood pressure of a cerotic patient is 90 to 120 Mill M of mercury mild to moderate tardia with a typical resting heart rate of 90 to 110 beats per minute and less commonly discussed but equally as important a blunted cardiac response to physiologic stress so even if cardiac output at Baseline for the cerotic patient is increased heart rate and contractility are
unable to increase further in the setting of sepsis or hypovolemia this has rarely been referred to as serotic cardiomyopathy the ideology of these abnormal hemodynamics is not entirely clear though there is strong speculation that it comes from some as of yet unidentified circulating baso active substance let's move on to discuss the findings due to decreased number of functioning hepatocytes starting with decreased protein synthesis in this discussion of physical findings the protein of greatest relevance is albumin as mentioned earlier hypo albuminemia contributes to the formation of a cites and a lower extremity edema in addition it's
believed to be part of the mechanism behind two findings of the fingernails the first of these are called teres Nails in which the majority of the nail bed appears white with no lunula leaving only a small strip of pink between most of the nail bed and the white nail tip the finding is not specific for curosis however when seen in a patient with unnown history of alcohol dependence the probability that the patient has underlying curosis increases dramatically another nail finding is murky's Nails these are composed of alternating white lines running parallel to the lunula the
lines are actually not part of the nail but rather lie within the nail bed thus they disappear with pressure placed on the nail and they do not move with nail growth as with Terry's nails they are not specific for curosis and how hypo albuminemia and malnutrition in general contributes to these findings is not known the next problem is decreased conjugation of B Rubin normally when red blood cells break down the he molecule is released from hemoglobin and then converted into a compound called B Verdin within the macrofagos this is then converted into unconjugated B Rubin
because unconjugated B Rubin is relatively insoluble for efficient excretion into the bile it must be joined with glucoronic acid in the liver to form conjugated B Rubin unconjugated and and conjugated bil ruin are more commonly referred to as indirect and direct bil Rubin respectively which is a reference to the lab techniques used to measure them when there are too few hepatocytes functioning bil Rubin cannot be conjugated which means it can't be effectively excreted into the bile and thus its concentration increases this leads to the findings of jaundice a yellowish discoloration of the skin and sclero
ioris a yellowish discoloration of the eyes both of these can usually be detected when the total B Rubin exceeds 2.5 to 3 Mig per decil there's an old discussion about which location in the body is best to detect jaundice for example when I was in med school I remember a seasoned Professor insisting that under the tongue was the best location in my experience when it comes to identifying early jaundice far more important than location is the quality of light bright white daylight is probably best certainly much better than the fluorescent lighting found in many hospital
rooms the next pathophysiologic arrangement in curosis is the decreased detoxification of blood now that's a very vague description of a very complex collection of biochemical processes but there's a reason for that we don't really understand the biochemistry involved what we do know is that failure of detoxification leads to somnolence slow and slurred speech and a finding called asterixis All of which together comprised a clinical syndrome of hepatic enop to demonstrate asterixis the patient is asked to hold his or her arms outstretched with wrists extended and fingers straight there is an occasional irregular Motion in which
one hand at a time will experience sudden flexion of either the wrist and or the metacarpal joints which will then immediately return to the previous position for the most part asterixis is discussed only in the context of liver failure but it can also be seen in advanced renal failure and hypercapnia among other forms of metabolic incopy in the simplest story of what causes hepatic and cyop it's attributed to the simple compound ammonia the higher the ammonia the worst the incopy unfortunately this is not strictly true here's the results of one of multiple studies that looked
at the levels of Venus ammonia as a function of the clinical severity of incopy among patients with curosis each small dot represents a single patient you can see that patients with grade zero or no clinical evidence of incopy do not have different ammonia levels from those with mild to moderate incopy and all three of those groups essentially overlap with the normal range it's not until the incopy is severe in stages 3 or four that the ammonia level can differentiate the alter mental status from hepatic and cyop from other ideologies there are a number of theories
about this observation the most obvious is that ammonia itself is not a direct contributor to encylopedia of the condition another proposed explanation is that ammonia levels May Vary significantly over the course of the day but the development or resolution of clinically evident incopy is delayed by a number of hours due to permeability of the blood brain barrier and other similar factors one finding related to detoxification that is more definitively linked to a specific toxin is called feder hepaticus this is a specific odor to the breath of patients with Advanced liver failure which is sometimes described
as either a sweet musty odor or slightly feculent one multiple Studies have demonstrated that this compound dimethyl sulfide is the predominant cause the final relevant pathophysiological der rement is an abnormal balance of the sex hormones specifically in liver failure there appears to be an increased systemic release of an androgen called andrin diione this leads to increased peripheral conversion to estrone and from there to other estrogens in addition there appears to be an increase in sex hormone binding globulin which binds to testosterone decreasing the amount of the free biologically active form of this hormone the net
consequence is an imbalance between estrogens and testosterone there are five major physical findings related to this imbalance testicular atrophy gynecomastia loss of axillary and chest hair Palmar athema which is manifested by redness of the thear and hypothenar eminences which blanch with pressure and which spares the center of the palm and last spider angomas also called spider nevi which are small skin findings typically seen on the chest shoulders and upper back these also blanch with pressure and they refill from the center outward a few spider angomas are occasionally seen in normal healthy individuals but an arbitrary
cut off of more than five is generally considered suggestive of underlying pathology you might have noticed that nowhere in this video have I yet discussed examination of the liver itself while detection of a firm nodular liver Edge on palpation may suggest therosis estimation of hepatic signs on exam has limited role in its diagnosis part of the reason for this is that measurement of the liver in a single Dimension provides a relatively inaccurate estimation of size and thus probability of liver disease due to the great variability of the liver shape in three dimensions between different people
most importantly however curosis can result in either an enlarged or once Advanced a small shrunken liver I'll end with the evidence Behind These physical findings that is what are the sensitivities and specificities of the findings for curosis or more importantly the positive and negative likelihood ratios in article and jama's excellent ongoing series on the rational clinical exam looked at this issue in 2012 here's a summary of their review of the literature the physical findings are listed from highest to lowest positive likelihood ratio the best available evidence demonstrates that of all the findings of therosis the
ones whose presence most significantly increases the odds of a patient having therosis is Terry's nails and gynocomastia this is interesting because in my experience these are among the least frequently discussed findings of curosis the more commonly discussed findings of distended veins incopy and aites are up there as well and notice where pegal is the very bottom so the presence of a omally only modestly increases the odds of patient has curosis the last important observation to make here is that the positive likelihood ratios are as a whole much much more significant than the negative likelihood ratios
that means that the physical exam is much better at ruling in a diagnosis of curosis than ruling it out that concludes this video on the physical findings of curosis and I hope you found it interesting and useful [Music]