>> Anabela Marcal: Hello everyone. My name is Anabela Marcal, and I'm the European Medicines Agency liaison official to the Food and Drg Administration. I've been at European Medicines Agency for 24 years, and I've had different roles, including in clinical trials, pharmacovigilance, and inspections.
In this lecture, I'll give you an overview of the authorization of medicines in the European Union, in particular, an overview of the centralized procedure. My lecture will cover, amongst others, the following topics: which products are eligible for the centralized procedure; timelines for assessment of a marketing authorization application submitted through the centralized procedure; the assessment procedure itself; who is responsible for what; early access tools available in the European Union; eye level overview on how we monitor medicines once they are on the market; and to finalize, an overview on transparency, meaning what do we publish for products we assess? How are medicines approved in the E.
U. ? In the E.
U. , we have different authorization routes, but in all cases, the same set of rules apply. Medicines in the E.
U. can be authorized through the centralized procedure or through national procedures at the level of the E. U.
member states. Let's start by the centralized procedure. So, in the centralized procedure, companies submit their application to the European Medicines Agency, and there will be one assessment at the end.
There will be one marketing authorization that will be valid in all E. U. 27-member states.
There will be one marketing authorization order for all E. U. member states, one single product name, one set of product information.
So, the labeling will be the same for all the E. U. member states.
And this is the procedure that applies for the vast majority of all new medicines in the E. U. When it comes to the national procedures, applicants submit the marking authorization application to the national competent authorities of the member states where they want to place the medicinal product.
So, they can choose if they are going to apply in two, three, 20-member states. For these national procedures, we have two distinct procedures. The so-called mutual recognition procedure, which applies where marking authorization applicants have a product already authorized in one E.
U. member state. And then they apply in another E.
U. member state and ask for the initial authorization to be recognized. So, in this process, it allows member states to rely in each other scientific assessment.
The other route, it's the decentralized procedure which applies where applicants apply for the simultaneous authorization of a medicine in more than one-member state if it has not yet been authorized in any E. U. member state.
As I mentioned at the beginning, the focus of this lecture will be the centralized procedure. The centralized procedure requires the applicant to submit a single application to the European Medicines Agency. The centralized procedure is dedicated to innovative products, and it is mandatory for specific categories of products.
Once a company submits a marketing authorization application through the centralized procedure, the European Medicines Agency Scientific Committee for Human Medicines, the CHMP must, within 210 active days, deliver a scientific opinion recommending the granting or the refusal of the marketing authorization. The scientific opinion is then sent to the European Commission who is going to issue a legally binding decision, meaning, for instance, the granting of a marketing authorization valid throughout the E. U.
27-member states. Which medicines are then approved through the centralized procedure? The centralized procedure is mandatory for certain categories of products, as highlighted in this slide.
This is established by law by regulation (EC) 726/2004. The mandatory scope includes the following products: new active substances for the treatment of HIV, cancer, diabetes, neurodegenerative diseases, autoimmune diseases, and viral diseases; medicines derived from biotechnology processes; advanced therapies; orphan medicines; and innovative veterinary medicines. For other medicines, companies have the option of submitting an application through the centralized procedure.
This is possible for the following categories: new active substance; significant therapeutic, scientific, or technical innovation; medicines whose authorization would be in the interest of patients or animal health; generic of a product authorized through the centralized procedure; and marking authorization applications, including a pediatric indication. Once the marking authorization application is submitted, the centralized procedure follows an established timeline and process. Before submission, there are a number of activities taking place.
One of them is so-called pre-submission meeting. Pre-submission meetings are voluntary. And if the company wishes to have one, they need to come six to seven months in advance of the submission of a marketing authorization application.
During this meeting, the company presents the product and can ask questions related to scientific, regulatory, or legal issues in order to facilitate the subsequent validation and assessment of the application. Other activities occurring during the pre-submission phase include the appointment of the rapporteur, who will take the lead in the assessment of the application. The request for eligibility to the centralized procedure, meaning that the company needs to have the confirmation that the product is eligible for the centralized procedure.
Request for accelerated assessment, meaning that if the company would like an assessment quicker than the standard timeline for assessment, it needs to provide a justification before submission. Once the application is submitted, it's then validated. The validation includes the following: a technical validation to check if the structure of the dossier is compliant with the use specifications and rogatory and administrative content validation.
Once the application has been validated, the review procedure starts. During the primary evaluation, the rapporteur and co-rapporteur will review the data submitted and produce independent assessment reports. These assessment reports will be shared with all members of the Committee for Medicinal Products for Human Use, the CHMP.
The members have the opportunity to provide comments, and these will be followed by a discussion at the committee meeting. After this initial phase of 120 days, the scientific committee adopts a list of questions to the applicant indicating whether a medicine is in principle approvable or whether major objections have been identified, which preclude an approval. The clock is stopped and it's then up to the applicant to prepare answers to the questions.
The applicant has a period of three to six months to answer the list of questions. Once the applicant submits his answers, the clock is started at day 121, and the rapporteurs review the complementary information provided by the company. The rapporteurs prepare a joint assessment report, and if needed, the committee issues a list of outstanding issues.
The applicant can also be given the opportunity to be heard by the EMA Scientific Committee. An opinion, positive or negative, i. e.
, recommending the granting or the refusal of the marketing authorization, needs to be adopted by day 210. The CHMP opinion is then sent to the European Commission who has 67 days to prepare a binding decision. The decision to grant a marketing authorization valid throughout the E.
U. should be given by day 277. The decision, including product information, is given in all official languages of the European Union.
There are possible additional steps in the procedure. This includes, for instance, requests for good manufacturing practice, good laboratory practice, or good clinical practice inspections. The CHMP can also decide to consult with scientific advisory groups or doc expert groups.
Scientific advisory groups are groups established by the CHMP in connection with the evaluation of specific therapeutic areas. They consist of European experts selected according to the particular expertise. For instance, we have SAG, cardiovascular SAG, oncology SAG, and so on.
The CHMP can also consult other committees, for instance, the Committee on Advanced Therapy, the Pediatric Committee, and working parties. Working parties are groups of experts in specific areas, for instance, quality working party, methodology working party, biosimilars working party, pharmacokinetics working party. I've mentioned before that the rapporteur and co-rapporteurs are the ones taking the lead in the assessment of an application.
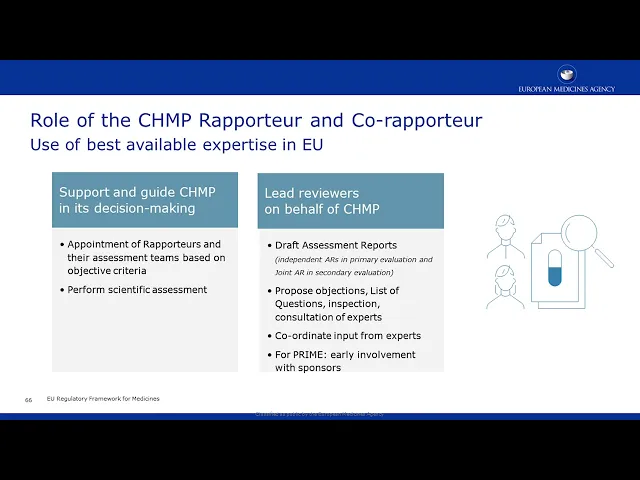
What is exactly the role of the rapporteur and co-rapporteurs? The rapporteurs, together with their assessment teams, lead the scientific assessment of an application. The rapporteurs act as lead reviewers on behalf of the CHMP.
They draft the assessment reports, as we have seen before, independent assessment reports in the primary evaluation, and then a joint assessment report in the secondary evaluation. They propose objections, list of questions in the need for inspections, the need to consult experts. They coordinate input from experts and from the committee members.
And in certain cases, for instance, for products that are given prime, they also have an early involvement in the -- before submission of the application. The rapporteurs are appointed on the basis of objective criteria. And these objective criteria include the ability of the rapporteur to fulfill the role, the composition of their assessment team, the scientific competence, the regulatory experience, and also trying to obtain an even distribution amongst the members of the committee.
We can also have rapporteurs from other committees during the evaluation of an initial marketing authorization application. This includes, for instance, the PRAC rapporteurs. PRAC is the Pharmacovigilance and Risk Assessment Committee.
During the marketing authorization application, they are responsible for the assessment of the risk management plans, focusing on the prospective planning aspects like pharmacovigilance plan and risk minimization measures. They're also responsible to issue the list of questions related to the risk management plans. And once a product is authorized, they will be [unintelligible] involved in post-authorization safety-related procedures.
We can also have rapporteurs from the Committee on Advanced Therapies, and this is specifically for products that are ATMPs. For ATMPs, the CAT rapporteurs are the ones leading in the scientific assessment of an initial marketing authorization application. And then the CHMP acts as an overarching peer reviewer.
And what is the role of the CHMP itself? The CHMP is the EMA's Committee for Medicinal Products for Human Use and is composed by one member plus one alternate from each member state. In addition, it also includes five co-opted members that are nominated to CHMP on the basis of expertise in certain areas.
This could be, for instance, expertise in medical statistics, pharmacokinetics, biologics, on ATMPs, pharmacoepidemiology, and so on. What is the role of the CHMP? The CHMP is responsible for the assessment of a marketing authorization application and to give an opinion on centralized marketing authorization applications.
And as seen before, this is based on the rapporteur's and co-rapporteur's assessment reports, on the PRAC rapporteur's assessment of the risk management plans, comments from other CHMP members, and consultation with experts. The CHMP is also responsible for assessment and opinions for post-authorization procedures. So, once a product is authorized, if there are variations or if there are, for instance, to include a new indication or to include a new formulation, the CHMP continues to be the main body responsible for this assessment.
The CHMP is also responsible to give opinions regarding suspension, withdrawal of a marketing authorization within the context of European review procedures. Meaning that in certain cases, even if a product is nationally authorized, the CHMP can get involved and do an assessment if this is considered of interest for the European Union. For instance, when a new safety issue arises in a specific member state related to that product.
The final CHMP opinion and assessment report reflects the scientific review of the submitted dossier, further information provided during the assessment, the discussions held at CHMP, the information provided by the applicant in a hearing. It also reflects if there have been divergent views in the CHMP. And now, the committee finally concludes on the benefit-risk.
And of course, it also explains how the CHMP arrived at specific statements in the product information. The CHMP opinion is adopted by consensus or majority vote. And in the case of majority vote, the divergent views are included in the opinion as well.
I would like now to highlight a few features of the centralized procedure. The first one is about accelerated assessment that I mentioned also at the beginning. Accelerated assessment reduced the timeframe of CHMP to review a marketing authorization application from 210 to 150 active days.
Applications may be legible for accelerated assessment if the product is of major interest for public health, particularly from the point of view of therapeutic innovation. Any request for accelerated assessment should be made at least two to three months before submitting a marking authorization application. The applicant should provide sufficient justification.
And on that basis, the CHMP will decide if this marking authorization application is eligible or not for accelerated assessment. The accelerated assessment timeframe can be reverted to standard assessment during the assessment of the marking authorization application in case of major issues with the application. Conditional marketing authorization.
EMA supports the development of medicines that address unmet medical needs. In the interest of public health, applicants may be granted the so-called condition marketing authorization for certain medicines on the basis of less comprehensive data than normally would be required. Where the benefit of immediate availability of the medicine outweighs the risk in rent, in the fact that additional data are still required.
Medicines for human use are eligible for conditional marking authorization if they are intended to treat, prevent, or diagnose seriously debilitating or life-threatening diseases. This includes also for medicines, and its use is also intended for public health emergencies. The CHMP may grant conditional marketing authorization if all of the following criteria are met.
The benefit-risk balance of the medicine is positive. It is likely that the applicant will be able to provide comprehensive data post-authorization. The medicine fulfills an unmet medical need.
The benefit of the medicine becoming immediately available to patients is greater than any risk in rent in the fact that additional data are still required. Conditional market authorizations are valid for one year and need to be reviewed annually. Once the conditional marketing authorization has been granted, the marketing authorization order must fulfill specific obligations within defined timelines.
These obligations could include completing ongoing or new studies or collecting additional data to confirm the benefit-risk balance of the medicine. The marketing authorization can be converted into a standard marketing authorization once the marketing authorization order fulfills the obligation imposed and the complete data confirms that the medicine's benefits continue to outweigh its risks. An authorization can be granted under exceptional circumstances if the applicant can demonstrate that he is not able to provide comprehensive data on the efficacy and safety of the medicine under normal conditions of use because of one of the following reasons.
The indication for which the product is intended is rare and therefore, the applicant cannot reasonably be expected to provide comprehensive evidence. Or in the present state of scientific knowledge, comprehensive information cannot be provided. Or it would be contrary to the accepted principles of medical ethics to collect such information.
The marketing authorization is granted subject to specific obligations, which will be reassessed on an annual basis. However, the marketing authorization is valid for five years. In this table, you have a summary of the main features of the different types of marketing authorization.
So, you have the standard marketing authorization where you have comprehensive data at the time of the authorization. The authorization is valid for five years, and this is the standard situation. And of course, the fact that it's a standard marketing authorization, it still may have some post-marketing requirements or some conditions for post-authorization safety studies or post-authorization efficacy studies to be conducted.
Then we have the conditional marketing authorization, where we do not have comprehensive data at the time of authorization, but it is expected that the company will be able to get such data after authorization. So, at a certain point in time, this conditional marketing authorization will revert, and it'll go to a full standard marketing authorization. The conditional marketing authorization is valid for one year, and it's renewable every year.
It's only possible in the centralized procedure, and this conditional marketing authorization is granted with specific obligations to be completed according to defined timelines. And then the marketing authorization under exceptional circumstances, comprehensive data cannot be expected to be obtained, meaning that pretty much this marketing authorization will always remain under exceptional circumstances. It's valid for five years, but there will be an annual reassessment every year.
It's possible in all types of registration procedures in Europe and as well can have specific obligations and specific conditions to be fulfilled. This slide illustrates at a very high level how we monitor safety of medicines once they come into the market. So, once marketing authorization is given, how do we monitor the safety of medicines in the E.
U. ? European Medicines Agency is responsible for coordinating the E.
U. 's pharmacovigilance system for medicines and can take action if the information indicates that the benefit-risk balance of a medicine has changed. How does the EMA do this?
The safety of medicines in the E. U. is constantly monitored via reports from patients and healthcare professionals, clinical studies, medical literature, patient resistors, and collaboration with regulatory bodies outside the E.
U. The marketing authorization audit, of course, also has specific obligations to submit adverse reactions to the E. U.
system and to submit periodic safety update reports in accordance to established timelines. EMA is also a dedicated committee to the safety of medicines for human use, the so-called PRAC, Pharmacovigilance and Risk Assessment Committee. The PRAC is responsible for the assessment of periodic safety update reports, any signals that arise, pass authorization, safety studies, risk management plans.
PRAC can also give recommendations regarding the changes or suspension, or revocation of certain medicinal products due to safety issues. And to finalize my presentation, I would like to give a brief overview of what we publish regarding marketing authorizations. So, at the time an opinion is adopted, an opinion recommending the granting of marketing authorization, we announced in the CHMP highlights, that a positive opinion has been adopted by the CHMP.
The CHMP meets once a month, every month. And in addition to the announcement in the so-called CHMP highlights, we also publish a patient-friendly summary of the opinion. And this is valid for positive as well as negative opinions, meaning that if the CHMP recommends that a certain product should not be given a marketing authorization because the benefit-risk balance is negative, we also made that information available in the public domain.
The EMA also publishes information on applications withdrawn by the applicant. Meaning if at any time during the assessment of the procedure, the company decides to withdraw the application, we also put that information in the public domain. In addition to this, we also develop and prepare what we call the European Public Assessment Report, or the so-called EPAR.
The EPAR is published once the commission has issued the decision granting the marketing authorization. And then in the post-authorization, we also publish information on new safety issues, suspensions, or any other changes to the products. Regarding the EPAR.
The EPAR is the European Public Assessment Report for each product authorized through the centralized procedure in the E. U. Once the commission decision gives the authorization, we publish this comprehensive report.
The EPAR includes information about the product, and this is, for instance, the presentations, the strengths, formulations available. The proved product information, meaning the information to the doctors, the so-called summary of product characteristics, the information to the patients or package leaflet, and the labeling information, the information that will appear on the boxes. We also publish any conditions to the marketing authorization.
So, if the marketing authorization was granted under specific conditions, for instance, studies that the companies still need to complete or others, these will be also published as part of the EPAR. We published a full scientific discussion based on the CHMP assessment report. And then once the product is authorized, we'll keep updating the EPAR according to the latest post-authorization procedures.
In addition to the EPAR for each product, we also publish clinical data. Since 2010, EMA had already been releasing clinical trial reports, but on request, meaning under the access to documents policy. However, since January 2015, we are also proactively publishing the clinical overview summary and study reports of products for which we gave a marketing authorization under the centralized procedures.
So, as I said, this is applicable for all marketing authorization applications submitted after the 1st of January, 2015. We only do that after the decision on the application is taken, and we have also done that for COVID-19 vaccines and products. And just to test your knowledge, just a few questions on the topics of my presentation.
All medicines authorized in the E. U. are assessed by the EMA Committee for Human Medicines.
True or false? False. In the E.
U. , there are two main processes of authorizing medicines. There is the centralized procedure, and there indeed, the Committee for Human Medicine, CHMP is the main body responsible for the assessment.
But we also have the so-called national reauthorized products that are authorized at the national level by the regulatory authorities of the member states. And these are not seen by the CHMP. The EMA is responsible for the granting of marketing authorizations for products assessed through the centralized procedure.
True or false? False. The EMA is responsible to give a scientific opinion or a scientific recommendation.
The legal act of giving a marketing authorization is the responsibility of the European Commission. A conditional marketing authorization can be recommended when it is expected that comprehensive data can be obtained after authorization. True or false?
True. Indeed, if there is an unmet medical need, and if it's considered that after authorization that the information submitted at the time of the marketing authorization application could be complemented, and as far as on the basis of the available data, the benefit-risk of the product is considered positive, then we can -- the CHMP can recommend a conditional marketing authorization. An authorization under exceptional circumstances will be reverted to a standard marking authorization after a few years once further data is obtained.
True or false? False. The authorization under exceptional circumstances, it is not expected that comprehensive data will become available.
The EMA publishes proactively clinical stat reports for authorized products. True or false? True.
Thank you very much.