all right all right Red Nation today we're going to be talking about cardiac CT this is an area that's been really hot in CT Imaging for the last 20 years and is an area where the vendors really try and show off as far as the technology such that they can image the beating heart as you can imagine Imaging the beating heart is going to be one of the most difficult challenges from a temporal resolution perspective on the system so we're going to talk all about how cardiac CT Works different options you have for scan modes
for doing cardiac CT and also about temporal resolution on the system which is very important in the context of cardiac CT coming up here at how Radiology works so as your heart is beating the idea is that we can do CT images in order to look at the coronaries look at the whole heart look at the valves all these different applications within cardiac CT and the idea for behind cardiac CT is we want to find when the heart doesn't move as much and then we want to image quickly if you're interested you can look up
what's called the wiggers diagram online this has a general information behind the cardiac Anatomy eye level the heart is beating in what's called a cyclical pattern and we're going to use some extra information in order to do what we call gating of this scan such that we use the projection data that corresponds to the area that has the least amount of motion so if we look at right here this is actually a plot of the volume of the left ventricle over time and if you think about the volume it's filling with blood and then it
ejects blood filling with blood injects blood and as it's moving that's when you don't want to do imaging so as the volume is changing that's when you wouldn't want to do imaging because that's when there's going to be motion when it's relatively quiescent or not moving that's when you do want to do the Imaging if you look at it here you can see there's one portion here that might be okay to do imaging in and then there's a portion up here which looks even better do imaging in this is for a relatively normal heart rate
and in general for most moderate and lower heart rate patients Imaging during the diastolic region is preferred so we want an image in here where there's less motion and how can we identify the area that's there's less motion we're actually going to use another signal and it's actually the electrical signal so there's an electrical signal and you're probably familiar with ECG or EKG if you're uh in Germany in the heart there's actually an electrical signal that's generated in order to tell the heart to do the contraction and this is what's called the QRS complex here
it's the biggest measurable peak in the electrical signal so NCT Imaging we typically are just talking about the r waves these are the areas that are most easy to measure in our electrical signal so we go from one R wave to the next star wave and then we look usually at a fractional percentage along that R to R interval so often in CT Imaging we're just talking about Imaging somewhere in here around 75 of the r to R interval and that is in what we call Peak diastolic period so that's right in here once that's
the case you can see how you do this on your scanner you also have an interface which looks like this where you see an R Peak and R Peak and then you have the window over which you're going to be doing your Imaging then we ask the question what's the minimum scan range we need in order to acquire the complete amount of data to make our CT image so at a high level you can think about if we had parallel beams coming from this direction and see our video on filtered back projection if you want
to see what parallel beams look like we had parallel beams coming from this direction and then if we had parallel beams coming from this direction here if we kind of ignore the beam hardening artifacts that we talked about in our last video we can see that that is actually the same data so the Rays passing from One Direction are the same as the Rays passing from the other direction and thus if we have 180 degrees of what we call parallel beam data that's enough and beyond that we have just what we call redundancy or measurements
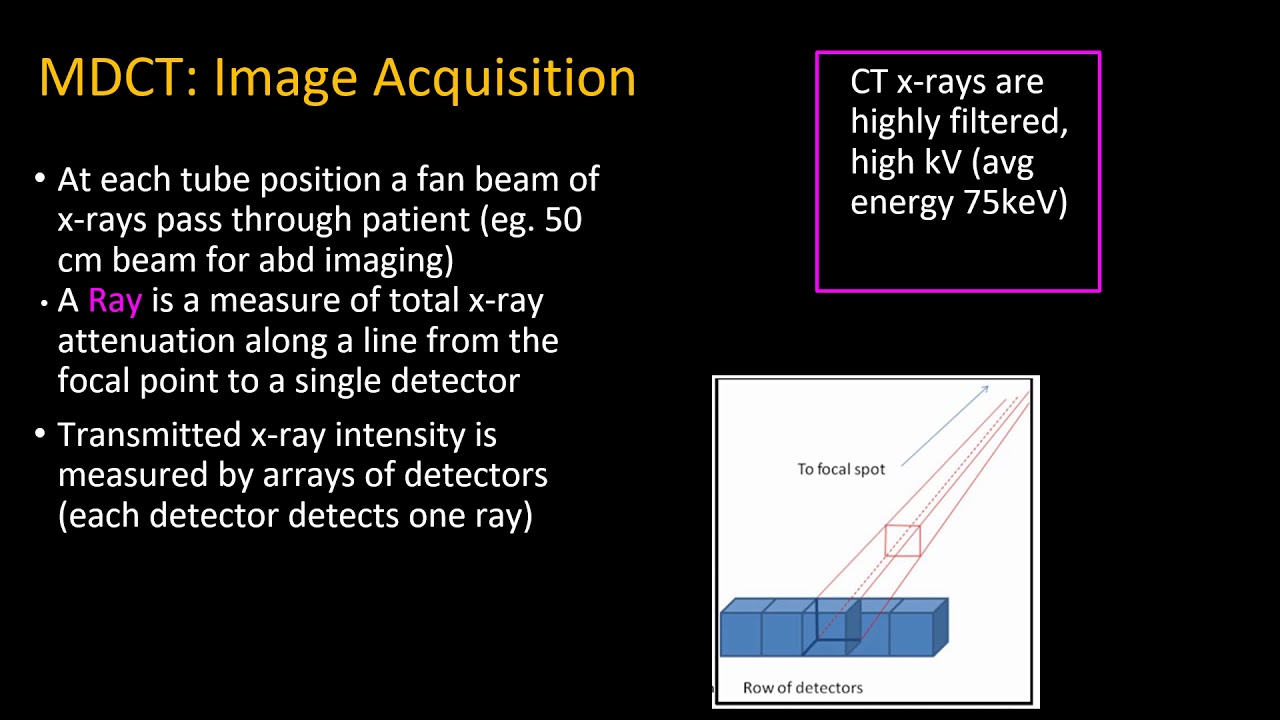
of additional data but it's not really required in order to make our CT image so we need 180 degrees of parallel beam data so how much data do we actually need from our system our system doesn't acquire parallel beam data it acquires what we call fan beam data so the data comes out in this direction see our video on third generation CT if you're interested in that General geometry but at a high level it's coming out like this from the source and then our detector is along an arc down here and then the fan angle
is essentially the angle covered by the detector so the amount of data we actually need is 180 degrees plus the fan angle if we have 180 degrees plus the fan angle then we're going to be able to re-bin into parallel beams and we can get 180 degrees of parallel beam data if we talk about the weighting function that we're going to use the projections are going to be weighted as a function of view angle and in the center they're going to have a higher weight and at the edge you're going to have a lower weight
the width of that function is actually 180 degrees at the center so what we call the full width half Max is actually 180 degrees so from that perspective what we talk about is what's the effective temporal resolution of cardiac CT if you have a single x-ray tube and detector on the Gantry it's actually approximately the rotation time divided by two high pass medium pets whoa press so low pitch helical scanning was the first way that cardiac CT was actually performed and in this case it's actually gated by the ECG signal that we talked about and
each little segment actually has a relatively low pitch so it's very close to actually an axial acquisition so you can do reconstruction which is very similar to axial reconstruction for this low pitch helical data in that scenario you can do gating like we talked about getting essentially a short scan of data and you can do that such that for each slab of data you will be able to reconstruct at the same cardiac phase then the Assumption here for the low pitch case is that the heartbeat is repeatable so that as you're going through you're going
to need many different slabs maybe seven slabs in order to image the whole heart or potentially more and as you're going through you're doing each of those slabs the assumption is if you're at the same point in the ECG signal that your heart will be in the same position if that's not the case you'll see some differences and we call those slab artifacts or artifacts of the interface between the different slabs multi-slab axial was introduced next and in multi-slab axial the idea is that you would go around the patient and you could potentially scan the
heart in a series of three axial Acquisitions so this is called usually three beat cardiac sometimes it would take four beats depending on the coverage of those axial slabs but the idea here is that you could save radiation dose because in the case of helical that was very low pitch and because we are looking at prioritizing the gating we're actually going to not be using the data that's far away from that given heartbeat that's different than traditional helical reconstruction where there are opportunities to use redundant data in the case of cardiac reconstruction you're typically using
the minimum amount of data available so the helical acquisition for cardiac is relatively dose inefficient so the multi-slab axial was a big Improvement in dose efficiency you still can have those same artifacts at the boundaries between the different slabs in multi-slab axial there's a concept on a dual Source scanner of a high pitch acquisition so on the Dual Source scanner you actually can think of two different helices because there's two sources and two detectors so as those two different helices travel around the patient you can actually have a higher pitch than if you just had
one source and detector combination so in this scenario the Siemens health and ears have introduced what they call the turbo Flash and they have a flash mode specifically for cardiac where you can do perspective gating if the heart rate is relatively stable you can actually gate so that you have the table motion starting ahead of time and then you will image the volume using this high pitch helical acquisition so in this scenario you actually aren't doing the same gating where everything in the volume is at one given phase in this scenario you're just reconstructing based
on the data that you have and more of a typical helical acquisition so in that scenario you're actually changing the phase As you move down in the volume as the data range is changing you're changing the cardiac phase because the position that you acquired the data at is actually linked to the time then finally we have wide cone axial scanning so if you were designed a cardiac specific acquisition it would most likely look like this kind of wide cone axial scan because you can cover the whole heart in one beat and you're going to have
freedom as far as the phases that you can acquire so the wide cone axial is really optimal from the perspective of covering the whole heart within one beat the different things that we talked about banding artifacts those traditionally will occur on either the low pitch helical mode or on the multi-slab axial mode you would not have significant banding on either the wide cone axial or on the fast helical acquisition that's prospectively gated because in both of those cases you're only using one given beat in order to make that image volume and as far as the
phase consistency like we talked about if you assume that the object is going to come back to the same location then the low pitch helical the multi-slab axial those are both going to be at a consistent phase and the wide cone axial you actually don't have to have that assumption in order to get an image which is at one given phase in the case of the fast helical acquisition it's intentionally not going to be at the same phase such that you would optimize the image quality of each of the slices independently but they would be
at a changing phase with respect to one another as far as Dynamic Imaging if you want an image and make a movie or make measurements in the systolic and diastolic phase to look at something like ejection fraction if you're looking at that kind of dynamic Imaging as a function of the different phase it's going to be again dependent on that assumption if it's repeatable if the heart is returning to the exact same spot you're actually going to do okay with the low pitch helical or with the multi-slab axial when that's not the case you're going
to have banding artifacts and in the wide cone axial you actually don't have this assumption again and you are able to do the dynamic Imaging again this is not possible with that fast helical acquisition because you don't have the ability to do multiple phases of reconstruction if you're looking to image the lungs as well and you want a full field of view in this scenario if you don't have the Dual source and you do a low patriotical or you do an axial scan you'll be able to get the full field of view if you are
using the Dual Source there's going to be a constraint on the field of view based on the size of the second detector and then also based on the fact that you're doing a fast helical acquisition if you're using wide cone axial you will not have a constraint on the field of view the like we talked about the tempo resolution of a single Source scanner you're going to be able to say is approximately the rotation time for one time around divided by two then you can kind of heuristically do that again for a dual Source scanner
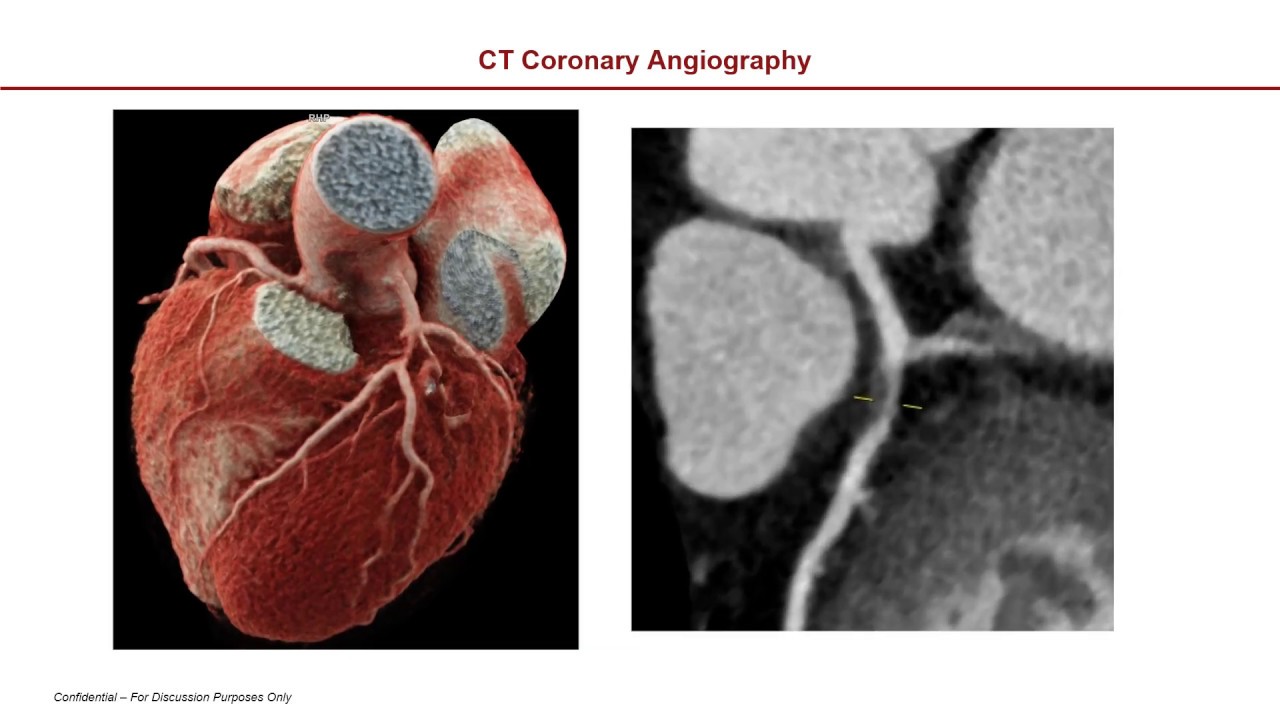
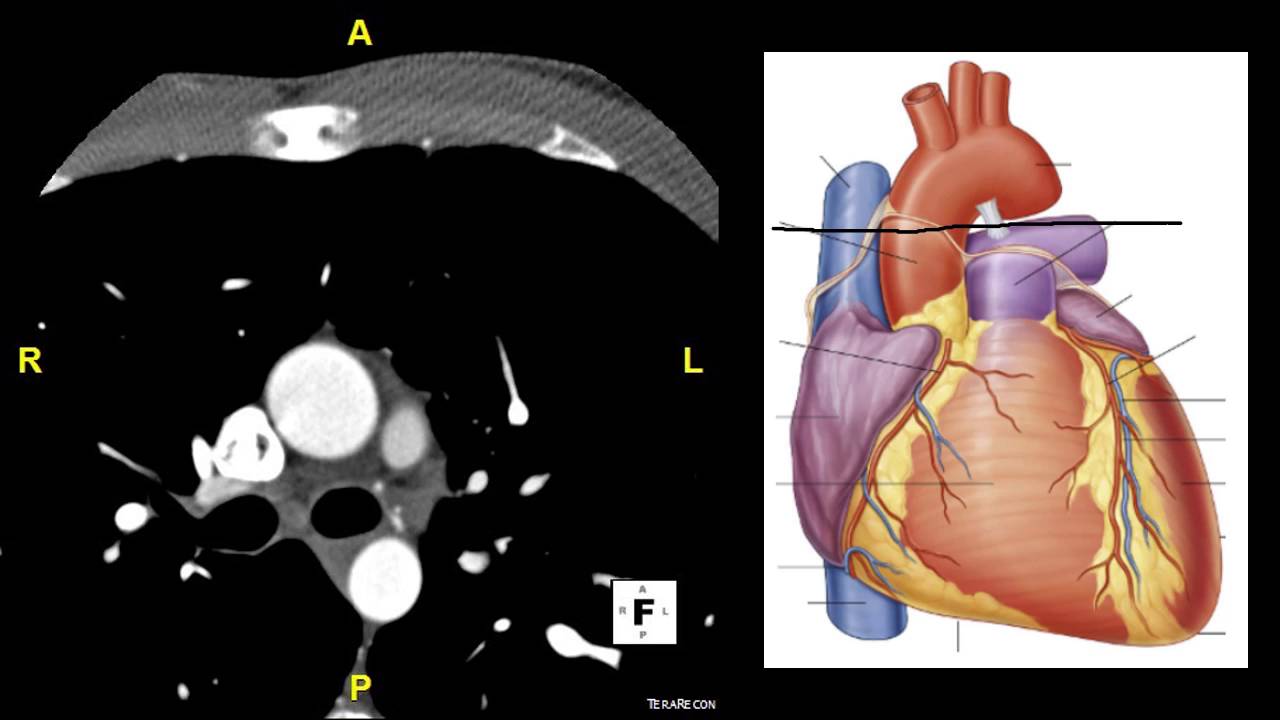
and divide that again by a factor of two but even though the Dual Source scanner does have the shortest temporal window to take the acquisition there are still residual motion artifacts you can see that here if you look at the left ventricle actually you can see there's significant residual motion artifacts during the acquisition itself and you can see in simulations that were done at GE if you look at the coronary artery there's a simulation of a coronary artery moving at the same velocity on the left is a single Source acquisition on the right is a
dual Source acquisition and in both scenarios you can see there's a significant tail here so this tail is due to the actual motion that was occurring doing the ACT during the acquisition so if there is motion of the coronary if you don't have an actual quiescent period what will actually happen depends upon the direction of that motion with respect to the source but in this case you can see this tail here and in the case of a dual Source system you're actually going to have two tails that are going to be added together with one
another but those tails are each significantly shorter so there's actually less of a span of the artifacts but you can see that there is not the ability to take a perfect image even with dual Source scanning there is potentially still motion artifacts we believe that motion correction should be used to optimize the image quality on all scanners and just like how cameras have both a fast acquisition then they also have software in order to help reduce the motion artifacts ocean artifacts can be significantly mitigated in CT scanning as well first product to do so was
called snapshot freeze this is introduced by GE Healthcare about 10 years ago now in 2012. the idea here is that we actually take multiple images so we make one image at the center phase we make one image a little bit earlier and one image a little bit later and the original snapshot freeze we would identify the coronary tree and the original snapshot freeze is actually just working to improve the Reconstruction quality in the coronaries after the coronary tree is identified then the areas where the coronaries are will actually track the motion based on those three
images and then we will do a motion compensation such that we can get images with significantly improved coronaries since that time some of the other vendors have also added Solutions so Canon has a solution that's coronary specific here and then Phillips has a solution also which is coronary specific so Phillips was more recently FDA approved and Canon's has been out for some time as well so if you look at the correction for these algorithms as long as there is good opacification in the vessels they can be detected and you can see here the vessel quality
especially in the RCA which is your fastest moving vessel especially for higher heart rates this is the case of a 70 beats per minute this is an 80 beats per minute patient you can really appreciate the Improvement in the coronary image reconstruction think about a simple test that you could perform you could actually think about having motion and then a stationary period and then motion again and have that motion be a linear motion velocity is set there based on the literature and you also want to consider different motion orientations if you haven't seen our video
about motion artifacts check out our video about motion artifacts in CT and you'll see why there's really a strong dependence on the direction of the motion and the types of artifacts that you're going to get we looked at four different directions of motion and then at different resting times so if you look at it as a function of resting time here is a artery and then we had a little calcification within the artery and this is before we did a segmentation on this side here and this is after we did a segmentation and then on
the left in each panel is the straight filter back projection result and on the right is after the motion compensation so you can see that as your resting period gets smaller there's going to be more and more motion blur occurring in the images and if you do just straight filtered back projection the object really gets spread out significantly such it's really tough to differentiate how much of that object is actually the calcification versus how much of that object is actually the vessel it's also the case that you want to have a system which is robust
with respect to the direction of motion because because the systems in general don't control the angle at which the X-ray tube goes on and off the idea is just to take the image at the right phase and so the angle is something that you actually don't have control over so we want it to be robust with respect to the different angles so if you look at just filtered back projection you can see there's some directions where there's relatively little difference and then there's some directions when where there is significant difference but if you look at
the motion correction case it's significantly improved and you could make plots of the error and this is basically a mean error over all those vessels you can also look at the variability standard deviation with respect to those vessels so namely how different are they going to be if it's moving in different directions both the error and the variability are significantly reduced and they're very stable in the case of the motion correction all the solutions that I talked about before those are all coronary specific so then GE was the first also to introduce a whole heart
solution which goes beyond the coronaries and looks at valves looks at implants and this is the whole heart solution and so you can see here before the correction and after the correction there's a significant Improvement in the image quality as there so much improvement with these algorithms there's actually an effective temporal resolution which is about 24 milliseconds in the case of these images and can comparison with the native images which if it was taken at uh 0.28 second Gantry the native reconstruction would be about 140 milliseconds over a cohort of patients you want to see
that your vessels are consistently interpretable such that you can actually perform your diagnosis and before having the snapshot freeze too if you looked at just the native reconstruction 92 percent of the vessel segments were interpretable and then over 99 of the vessel segments were interpretable with the snapshot to freeze correction so this to appreciate the clinical benefit that you can have in terms of more vessel segments being interpreted you really need to try these types of Corrections out in clinical practice next check out our video on motion artifacts in X-ray and CT in order to
really understand why we have these motion blurs and artifacts in our X-ray and CT images coming up