at the Opthalmology Clinic 71-year-old Zoe comes in she says that about 4 hours ago she experienced a sudden flash of light followed by many floaters in her right eye her visual disturbances have since progressed to a peripheral loss of vision and it's spreading to the rest of her visual field next to her an 8-month-old male infant named nban is brought in by his father who is worried because he noticed that nuran eyes appear white in their family pictures opthalmologic examination reveals the absence of red Reflex on both eyes on further questioning the father tells you
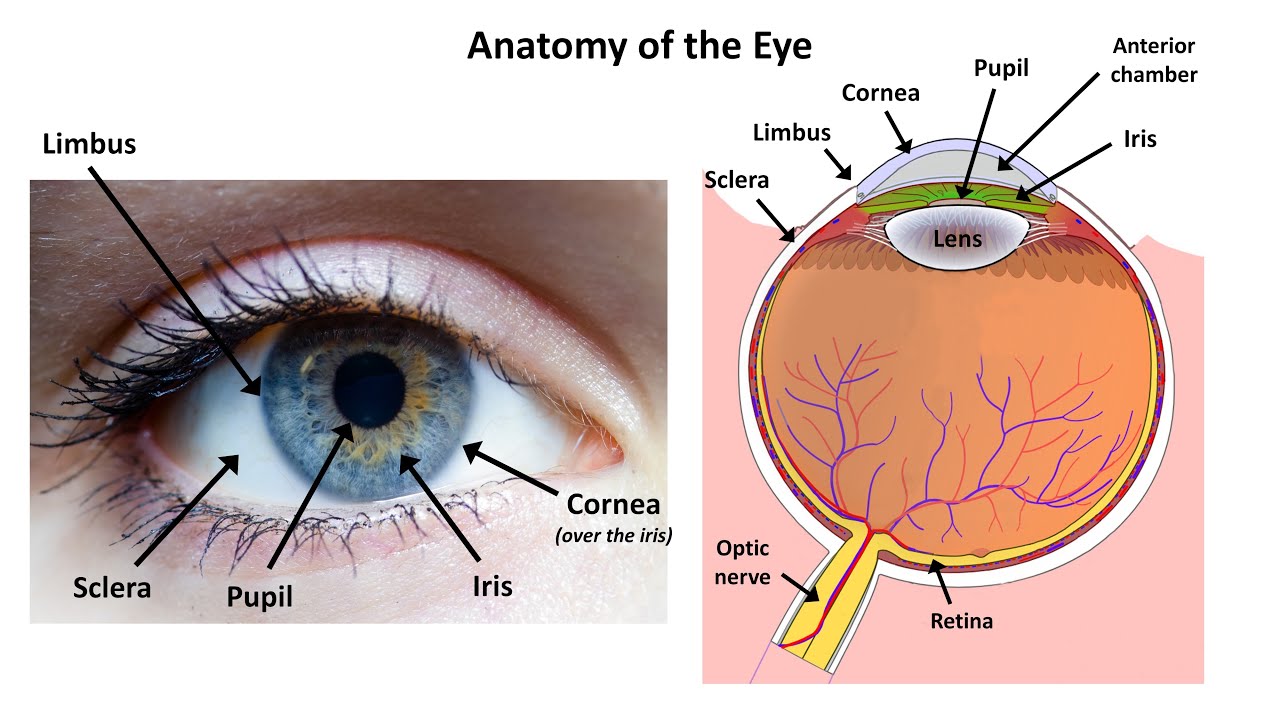
that as a child he had to have his left eye enucleated or removed but he's unsure as to the exact reason why based on the initial presentation both Zoey and nban have some form of retin disorder but first a bit of physiology if we zoom into the wall of the eye it is made up of three major layers there's a fibrous outer layer which contains the cornea and Scara and helps Shield excess light the middle vascular layer is called the uvia and consists of the iris pupil choid and ciliary body finally the neural layer consists
of the retina with its own outer pigmented layer and an inner neural layer that's composed of photo receptor cells which convert light into neural signals that travel via the optic nerve to the brain for visual processing okay let's start with age related macular degeneration or ar MD for short this refers to an acquired degeneration of the macula which is the central area of the retina it can be divided into dry or non-exudative armd which accounts for the vast majority of cases and wet or exudative arm rmd dry AR rmd is characterized by yellowish extracellular deposits
of waste materials that build up between the BR membrane and the retinal pigment epithelium for your test remember that these deposits are often known as drusen on the other hand in wet armd there is abnormal neovascularization meaning that abnormal blood vessels grow from the choid behind the retina and can leak intravascular fluid or blood in terms of symptoms dry armd usually presents with gradual vision problems such as metamorph opsia which is a typee of distortion where linear objects appear curved or discontinuous as well as scotomas or missing areas of vision and eventually it can lead
to central vision loss in contrast wet ammd causes rapid central vision loss over a few weeks or months ultimately individuals with armd can become legally blind even their peripheral vision remains intact diagnosis is based on fundoscopy and treatment focuses on slowing vision loss for dry armd multivitamin and antioxidant supplements have been shown to help while wet AR rmd can be treated with injections of antivascular endothelial growth factors or anti vef for short like bevas cisab or Rano bizum which inhibit neovascularization next there is diabetic retinopathy which is retinal damage resulting from longstanding and poorly controlled
hyperglycemia in people with diabetes melodus it can be broken down into nonproliferative diabetic retinopathy where damaged capital Aries leak blood into the retina and proliferative where chronic hypoxia results in neovascularization or the formation of new blood vessels that are fragile and can break bleeding into and damaging the retina for your tests it's important to remember that diabetic retinopathy is usually asymptomatic until late stages when it causes painless visual impairment that can progress to Blind diagnosis is made with fundoscopic examination which in the case of nonproliferative retinopathy reveals microaneurysms along with the high yield cotton wool
spots which are fluffy white patches on the retina now in addition to these findings proliferative retinopathy also shows neovascularization treatment of non-proliferative diabetic retinopathy relies on blood glucose control while proliferative diabetic retinopathy can be managed with anti-f injections peripheral retinal photocoagulation or surgery bear in mind that both nonproliferative and proliferative diabetic retinopathy can be prevented by keeping blood sugar under control similarly there is hypertensive retinopathy which refers to retinal damage from chronic uncontrolled hypertension for your exams remember that it is associated with an increased risk of stroke coronary artery disease and kidney disease now only
in late stages hypertensive retinopathy may present with decreased or blurred vision fundoscopic examination May reveal microaneurysms and cotton wool spots but what's even more characteristic is the macular star which results from the star-like deposition of exudates into the macula along with flame-shaped retinal hemorrhages and arterio venous nicking this is seen when an arterial with a thick arteriosclerotic wall compresses a vein that it happens to cross so this vein bulges on both sides next to the Crossing in severe cases papal Adema or swelling of the optic dis can also be seen treatment of hypertensive retinopathy requires
immediate and long-term control of blood pressure moving on to papal Adema which refers to swelling of the optic disc this is classically caused either by severe hypertensive retinopathy or by increased intracranial pressure due to a space occupying lesion such as tumor or Hemorrhage symptoms include blurring flickering or even complete vision loss for your exams remember that in the case of increased intracranial pressure individuals will often experience nausea and vomiting as well for diagnosis fundoscopic examination might reveal an enlarged blind spot and an elevated optic disc with blurred margins treatment focuses on managing the primary cause
if a reduction of intracranial pressure is needed diuretics and anti-hypertensives are commonly used next retinal vein occlusion refers to the compression of the central retinal vein or one of its branches due to a thrombus a narrow vein or from an atherosclerotic artery Crossing it this manifests as an acute monocular vision loss for diagnosis look for a history of cardiovascular risk factors such as diabetes melodus and hypertension or hypercoagulable States like polycythemia vera for diagnosis fun scopic examination May reveal optic disk swelling retinal hemorrhages and dilated veins that give a characteristic blood and thunder appearance edema
in affected areas can also be seen treatment can include laser photocoagulation and steroid or anti-f injections now don't confuse retinal vein occlusion with Central retinal artery occlusion which also results in acute monocular vision loss this can be caused by an embolism resulting from atrial fibrillation cardiac vegetations or a patent for Rayman ovali but might also be due to thrombosis of the retinal artery usually as a result of atherosclerosis on fundoscopy the retina appears cloudy with attenu vessels and the characteristic cherry red spot in the fobia OR Center of macula for your exams note that this
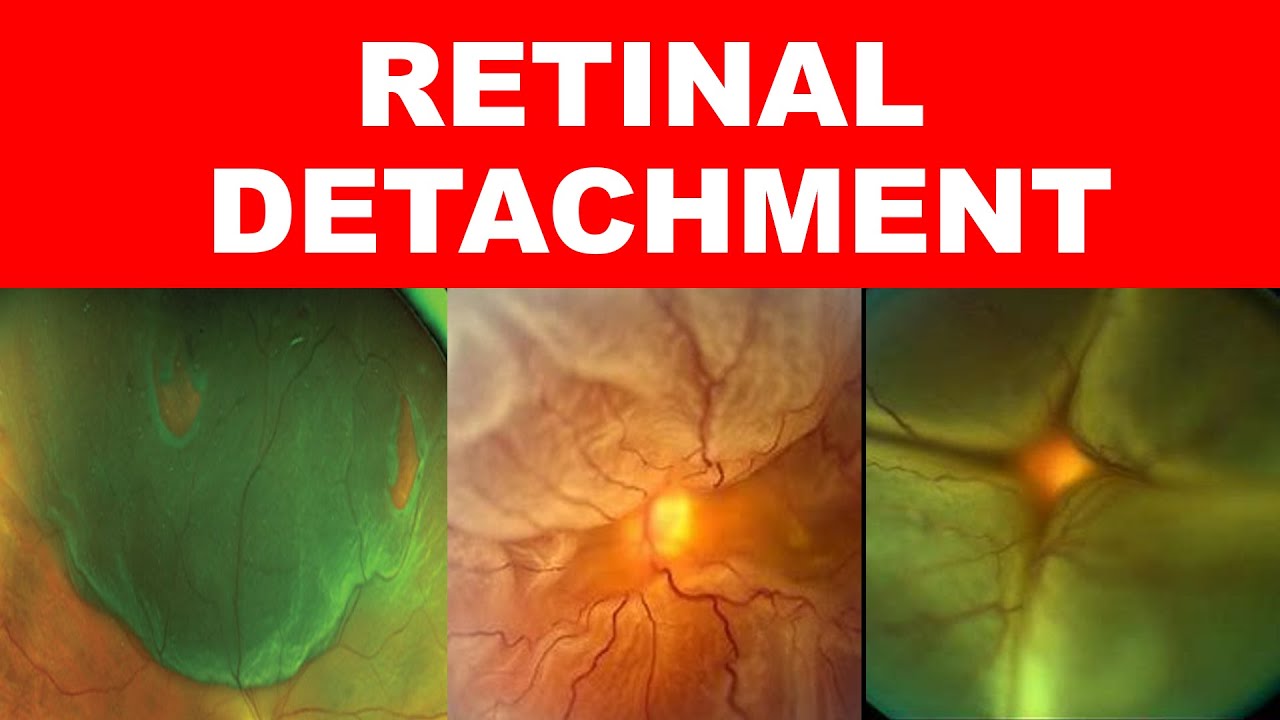
is seen because the macula receives its blood supply from the choid which remains unaffected while the surrounding retina is pale and Es schic due to the retinal artery occlusion treatment may include hyperbaric oxygen therapy which involves the inhalation of 100% oxygen at a pressure that's higher than the atmospheric pressure the purpose of this is to raise the amount of oxygen delivered to the esic retinal tissue finally to prevent further embolism it's also important to find the embolic source next retinal detachment occurs when the neurosensory layer of the retina is separated from the underlying retinal pigment
epithelium resulting in degeneration of the photo receptors and eventually vision loss the most frequent causes are retinal breaks which can be secondary to head trauma or Vitus degeneration which is a natural process that occurs with aging where the vitus humor changes from being a thick gel to a watery fluid significant vitous degeneration can lead to a posterior Vitus Detachment which in turn causes traction on the retina and potentially a retinal tear the liquefied vitus can then seep through the tear and under the retina causing it to detach another high yield fact is that retinol breaks
are also much more common in those with high myopia less frequently retinal detachment can occur without without any tears this is typically the result of traction on the newly formed blood vessels in proliferative diabetic retinopathy or inflammatory affusions the classic exam vignette will present someone with light flashes or floaters described as fine dots veils cobwebs clouds or strings followed by sudden visual field loss in the affected eye this typically begins in the periphery and progresses toward the central visual axis over hours to weeks like a curtain drawn down diagnosis is based on fundoscopic examination which
may visualize crinkling of retinal tissue or changes in blood vessel direction for your test remember that retinal detachment is an emergency and requires surgery to restore sensory function next is retinitis Pigmentosa this is a hereditary degeneration of the retina that results in painless Progressive vision loss what's high yield to know is that it starts with night blindness and peripheral vision loss and in late stages goes on to affect central vision retinitis Pigmentosa takes its name from the fundoscopic exam showing a pattern of bone spicule shaped dark spots and blotches that are visible around the macula
of the retina unfortunately there is no effective treatment the last retinal disorder is retinol blastoma this is a relatively common tumor in childhood caused by the mutation of both alals of the retinol blastoma or rb1 gene on chromosome 13 now retinol blastomas can be hereditary in which case the individual usually inherits a mutation in one of the AL of the rb1 gene if for some reason a random mutation occurs in the second alil of the rb1 that leads to the development of retinol blastoma this is known as the two hit hypothesis for your test keep
in mind that hereditary retinol blastomas are typically bilateral and are associated with an increased risk of developing other malignancies like osteos saroma soft tissue saroma and malignant melanoma another high yield fact is that an individual with hereditary retinol blastoma has a 50% chance of passing on the mutated alil to their child now there are also sporadic retinol blastomas which occur when two two spontaneous mutations affect both rb1 alals for your exams remember that sporadic retinol blastomas tend to be unilateral now in terms of symptoms what's especially high yield is that retinol blastoma typically presents with
lucco Coria or white pupil so when flash photography of the person is taken instead of the red eye effect they'll have white pupils this is particularly noticeable for unilateral cases since in the normal eye the light will reflect from the fundus and appear red but the tumor that grows on the fundus will block light so it appears white remember that another cause of lucco Coria is congenital cataract the tumor can also cause eye pain if large enough now if the tumor metast izes it can also present with anorexia or lack of appetite weight loss vomiting
headaches or neurologic impairment diagnosis of retinol blastoma begins with a red reflex test which functions similarly to flash photography light is directed from an opthalmoscope through the eye and then reflected back from the retina and appears red and since the retinoblastoma blocks the light the red reflex will be absent in the affected eye this is followed by a fundoscopy examination to confirm the diagnosis of retinol blastoma and to determine its exact location and extent of involvement definitive treatment consists of a nucleation or complete removal of the eyeball all right as a quick recap retinal conditions
include age related macular degeneration which is most often dry or non-exudative and rarely wet or exudative diabetic retinopathy results from longstanding and poorly controlled diabetes melodus and can be proliferative or nonproliferative hypertensive retinopathy results from chronic uncontrolled hypertension papal Adema refers to optic dis swelling due to hypertensive retinopathy or increased intracranial pressure retinal vein occlusion is associated with a thrombus or an atherosclerotic artery compressing the retinal vein or a branch while Central retinal artery occlusion is due to embolism or atherosclerosis retinal detachment is usually due to retinal tears but can also be caused by diabetic
traction or inflammatory affusions and is a surgical emergency retinitis Pigmentosa is an inherited Progressive retinal degeneration finally retinoblastoma can be hereditary or sporadic and causes lucco Coria and absent red reflex okay back to our cases 71-year-old Zoe came in complaining of an acute case of vision loss that's described as the curtain being drawn down in her right eye this was preceded by flashes and floaters this is classic for retinal detachment which was then confirmed with fundoscopy and treated with surgery in an emergency setting on the other hand nban the 8-month-old infant presented with bilateral lucco
Coria this along with the absence of red reflex and the possible family history suggests bilateral hereditary retinol blastoma diagnosis was confirmed with fundoscopy and treatment involved enucleation helping current and future clinicians Focus learn retain and Thrive learn more