Acute kidney injury, or AKI, is when the kidney isn’t functioning at 100% and that decrease in function develops relatively quickly, typically over a few days. Actually, AKI used to be known as acute renal failure, or ARF, but AKI is a broader term that also includes subtle decreases in kidney function. AKI can essentially be split into three types, prerenal AKI meaning the cause of kidney injury’s coming before the kidneys, postrenal AKI—meaning after the kidneys, or intrarenal AKI—meaning within the kidneys.
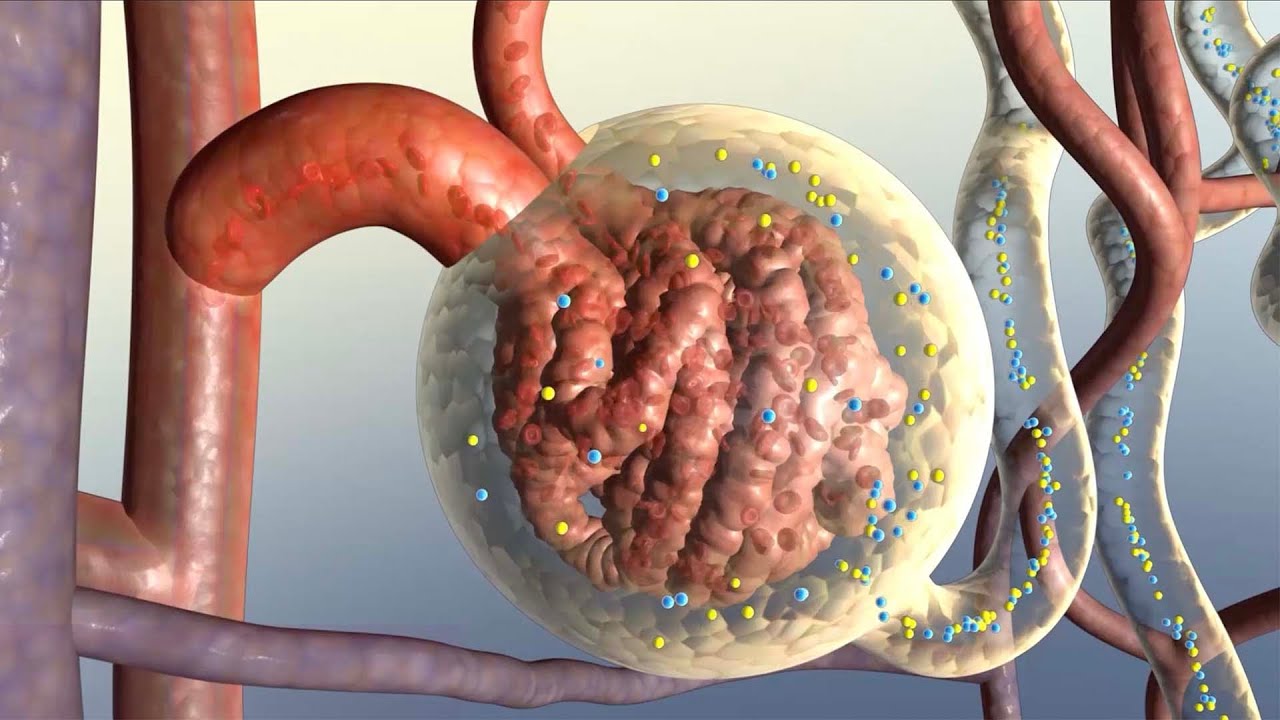
Now the kidney’s job is to regulate what’s in the blood, so they might remove waste, or make sure electrolyte levels are steady, or regulate the overall amount of water, and even make hormones - the kidneys do a lot of stuff! Blood gets into the kidney through the renal artery, into tiny clumps of arterioles called glomeruli where it’s initially filtered, with the filtrate, the stuff filtered out, moving into the renal tubule. Sometimes fluid or electrolytes can move back from the filtrate into the blood - called reabsorption, and sometimes more fluid or electrolytes can move from the blood to the fitrate - called secretion.
Along with fluid and electrolytes, though, waste-containing compounds are also filtered, like urea and creatinine, although some urea is actually reabsorbed back into the blood, whereas only a little bit of creatinine is reabsorbed. In fact, in the blood, the normal ratio of blood urea nitrogen, or BUN, to creatinine is between 5 and 20 to 1—meaning the blood carries 5 to 20 molecules of urea for every one molecule of creatinine, and this is a pretty good diagnostic for looking at kidney function! Ultimately the filtrate is turned into urine and is excreted from the kidney through the ureter, into the bladder, and peed away.
Meanwhile, the filtered blood drains into the renal vein. Alright so prerenal kidney injury is due to a decreased blood flow into the kidneys. So if you’ve got your body fluid, with fluid in circulating in the plasma as well as all the other intracellular and extracellular fluid.
So a decreased blood flow could be due to an absolute loss of body fluid, where fluid actually leaves the body. This could be due to major hemorrhage or blood loss, vomiting, diarrhea, or with severe burns where body fluid evaporates quickly without the protective skin. Decreased blood flow could also be due to a relative loss of fluid, where total body fluid stays the same, how can that happen though?
Well one example of this is distributive shock, which is where fluid moves from the blood vessels into the tissues, which keeps the total body fluid volume the same but you have a relative decrease in blood volume. Another example is congestive heart failure which is where the heart can’t pump blood to the tissues, so a portion of blood just pools in the venous side and isn’t pumped to the body, meaning less blood is sent to the kidneys. Finally, the issue could be local to the renal artery itself, for example, it could become narrowed, as in renal artery stenosis, or blocked by an embolus—which is a blood clot from somewhere else in the body.
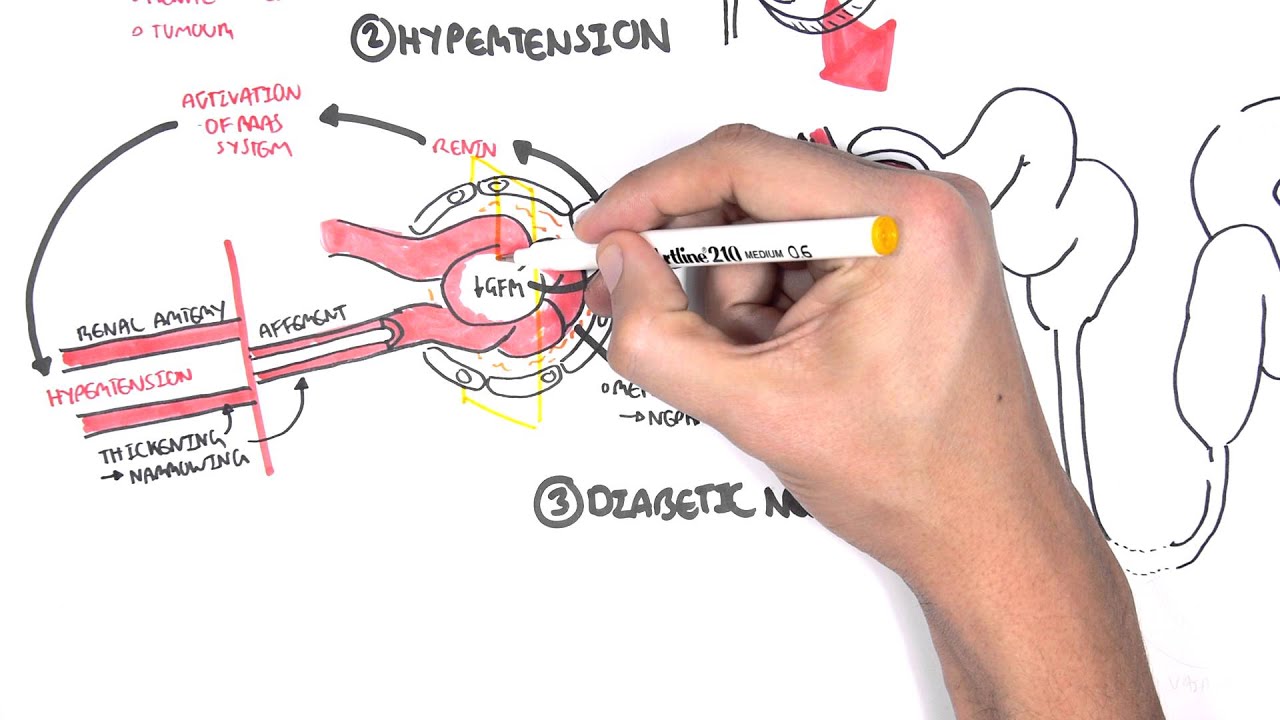
Whatever the case, less blood’s going to the kidneys, right? So less blood’s going to the glomeruli, which means less blood’s being filtered, so there’s a decrease in the glomerular filtration rate, or GFR, which is how much blood, usually in mL, the kidneys filter through their glomeruli per minute. If less blood’s being filtered, that means less urea and creatinine are filtered out, and more stays in the blood, which is called azotemia—high levels of nitrogen-containing compounds in the blood, this will also tend to cause oliguria, an abnormally low amount of urine production.
Also with less blood being filtered, the kidneys activate the renin-angiotensin system, which causes aldosterone release by the adrenal glands, which tells the kidneys to reabsorb sodium. When sodium gets reabsorbed, water gets reabsorbed as well. Water and sodium reabsorption is also tied to urea reabsorption, so in a prerenal situation, urea gets reabsorbed and so even more urea gets into the blood, resulting in a BUN to creatinine ratio of greater than 20:1.
Now, looking at what gets excreted in the urine, more sodium and water being retained means that less is excreted, and the urine sodium is usually less than 20 mEq/L, that the fraction of sodium excreted to sodium filtered, or FENa, is usually less than 1%, and finally that urine is more concentrated because remember less water is excreted, so typically the urine’s greater than 500 mOsm/kg - most of which is urea (which is why your pee smells so nitrogen-y when you’re dehydrated). Alright, so to recap, prerenal acute kidney injury is where the kidneys aren’t functioning at 100% and this is due to less blood flowing into the kidneys. Now that you know all about prerenal AKI, check out these other two videos on postrenal AKI and intrarenal AKI!
Thanks for watching, you can help support us by donating on patreon, or subscribing to our channel, or telling your friends about us on social media.