in this video we're going to talk about differential diagnosis for patellar tendinopathy enroll in our online course now link is in the video description hi and welcome back to physiotutors if you're a regular follower then you have watched our earlier more general video on six tips to diagnose lower limb tendinopathy they were number one epidemiological data two highly localized pain at the tendon emphasis three muscle wasting four hallmark signs and five pain onset 24 hours after high and fast load activity and 6 at last a proportional load pain relationship in this video we will specify
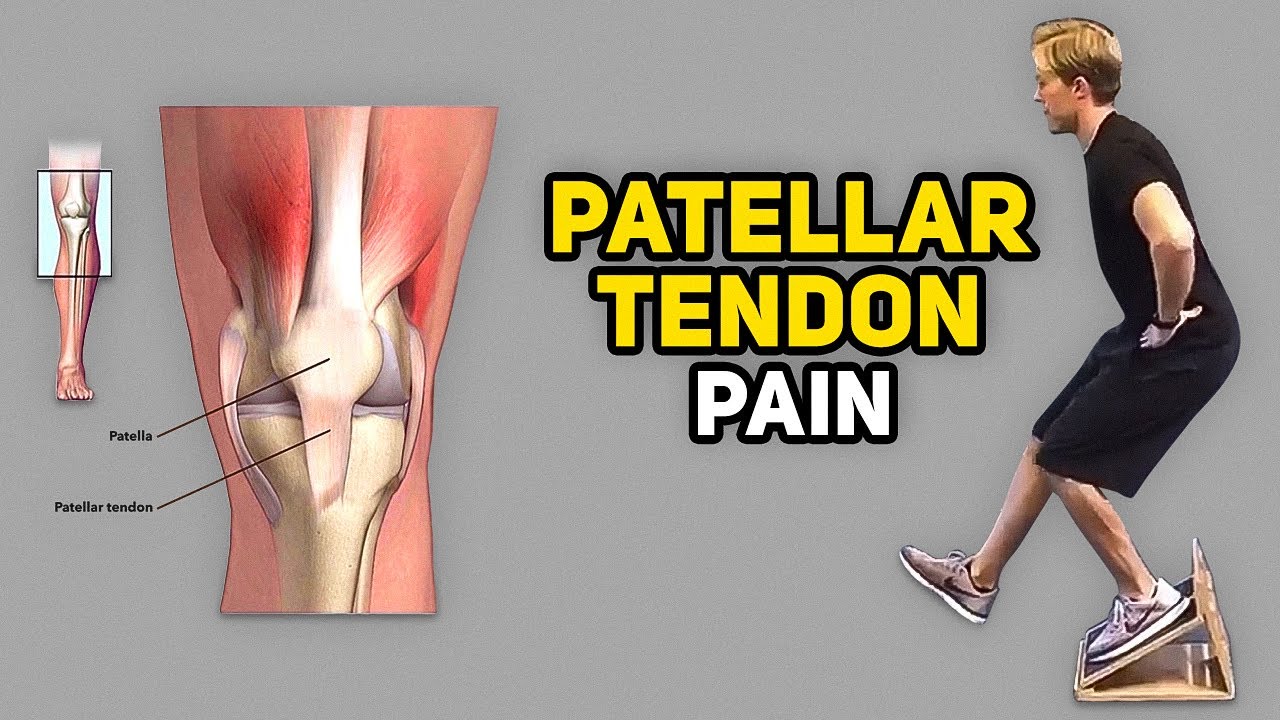
those 6 points for the patellar tendon and look at possible differential diagnoses so first epidemiology patellar tendinopathy is most prevalent almost exclusively in young jumping athletes between 15 and 30 years of age and more common amongst men the athletes who can jump the highest and run the fastest are usually the ones who run the highest risk of suffering from it number two localized pain while patellar tendinopathy can occur at the inferior pole of the patella it can also occur at the insertion of the tendon at a tibial tuberosity which is rarer if a patient reports
pain at the base of the patella you might suspect quadriceps tendinopathy a useful test to confirm patellar tendinopathy is the royal and hospital test which has a good sensitivity of 88 and a specificity of 98 percent to differentiate patients with patellar tendinopathy from other sources of anterior knee pain to perform the test palpate the patellar tendon for tenderness from proximal to distal with the knee in full extension then palpate the tendon spot again in 90 degrees of knee flexion this test is positive if pain in the flexed position is less or absent in this position
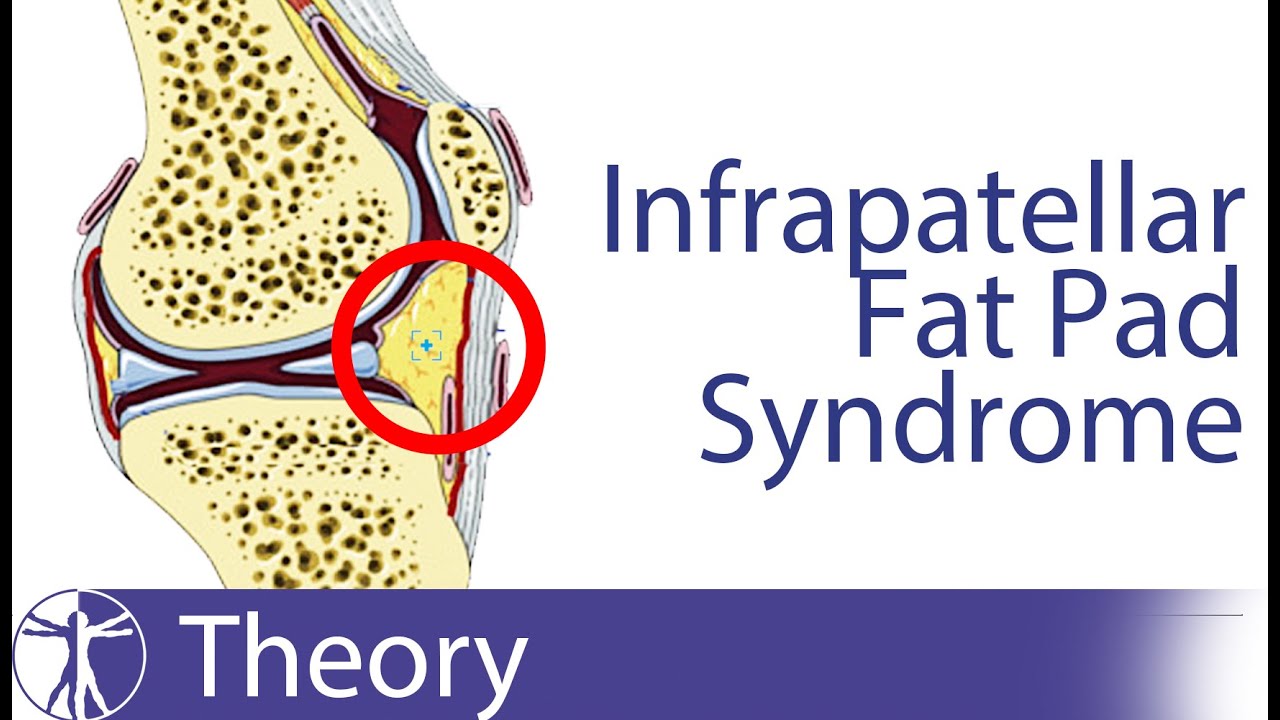
you can also directly perform the hoefus test to see if the fat pad is involved or not the procedure for it is pretty much the same as for the royal and hospital test only that you start in the flexed position and that you now palpate the infra-patellar fat pad for tenderness left and right of the patellar tendon then you palpate again with the knee straight this test is also positive if pain in the extended position is greater than in the flexed position note that fat pad irritation usually presents with more diffuse pain and is usually
aggravated by over-extension of the knee in young athletes at the start of puberty you'll have to keep growth plate pathologies in the back of your mind the most common one is oscar schlatter disease an overuse injury characterized by ossification of bone along the growth plate at the tibial tubercle in the most severe version osgood schlatter might result in an unfurious tibial tuberosity growth plate cinding glass and johansson is the equivalent of osgood schlatter only that now the apex of the patella is affected a very common differential diagnosis namely patellofemoral pain presents with diffused knee pain
and is more prevalent in young women with marked knee valgus during squatting if you're doubting applying a rigid tape with the mcconnell technique to reduce patellar compression and lateralization can confirm pfps in case the tape has a positive effect at last diffuse pain deep to the quadriceps tendon might be due to irritation of the suprapatellar fat pad and painful clicking might indicate suprapatellar plica syndrome both conditions can only be confirmed with imaging number three muscle wasting to examine muscle wasting observe the quads and calves for muscle bulk and differences and palpate them for tone which
is often reduced if patients have not been using them much the hallmark sign for patellar tendinopathy is pain when sitting with a bent knee like when sitting in the car for prolonged time like with other tendinopathies of the lower limb patellar tendinopathy presents with typical warm-up pain so after a patient has warmed up pain gets less number five pain onset or exacerbation 24 hours after high and fast load activities in a case of the patellar tendon you have to specifically ask for an increase in volume intensity and frequency of jumping that has led to the
onset of symptoms this is often the case after prolonged break as well and secondly the pain is usually increased 24 hours after those high and fast load activities so after an excessive jumping session and six proportional load pain relationship like with aeroteninopathy you are looking for an increase in pain with an increase in load on the patellar tendon a good starting provocation test can be decline squats in which very low intolerant patients report pain from as early as 30 degrees of flexion then continue with double leg hopping single leg hops maximal hops and maximal forward
hops for distance a very intense test is to ask a patient to come to a sudden stop on one leg after jogging or running as if they were to change directions pain levels have to increase with increasing difficulty so say if the decline squad was scored with a 3 out of 10 single leg hopping should be a bit higher with the highest scores at maximum hopping or a sudden stop from running all right this was our video about differential diagnosis for patellar tendinopathy if you want to learn how to rehab patella tendinopathy make sure to
watch the video to my right if you are looking to become an expert in tendon and muscle rehab of the lower limb check out our upcoming course on that topic with expert ana king on study.physiotutors.com and last i want to thank you for watching and please like this video if it was helpful to you don't leave without subscribing if you want to stay up to date with our latest video releases i'll see you next video bye

![How To Fix Patellar Tendonitis / Tendinosis [Jumper’s Knee Rehab Exercises]](https://img.youtube.com/vi/-dJIxiZcy_8/maxresdefault.jpg)




![How to Fix Knee Pain [Is It Patellar Tendonitis?]](https://img.youtube.com/vi/w5fXd5FCS_0/maxresdefault.jpg)