Therapy today's date is Tuesday June 16th 2015 the title for today's webinar is cancer revealed how our immune system sees and destroys tumors today's webinar is made possible through the generous support of Amgen Amgen focuses on areas of high unmet medical need and leverages its biologics manufacturing expertise to strive for solutions that improve health outcomes and dramatically improve people's lives A biotechnology Pioneer since 1980 amen has grown to be one of the world's leading independent biotechnology companies has reached millions of patients around the world and is developing a pipeline of medicines with Breakaway potential my
name is Brian Brewer and I'm director of marketing and Communications at the Cancer Research Institute Cancer Research Institute is the world's only nonprofit organization Dedicated exclusively to harnessing the immune system's Power To Conquer Cancer we fund signed ssts around the world whose work has led to significant breakthroughs in treating cancer with immunotherapy over the next 45 minutes you'll have an opportunity to hear firsthand from an immunotherapy expert how cancer treatment today is undergoing a revolution thanks to these breakthroughs after a 25 minute presentation from our speaker we will Open the discussion to questions submitted by
you you can pose your question at any time throughout the presentation by typing in the Q&A box on your screen screen we're also will be live tweeting this webinar so you can tweet your comments and questions to us at @ cancer research and be sure to use the hashtag CRI webinar today's webinar is being recorded and will be made available for viewing on the CRI website and on our YouTube channel now it's my distinct pleasure to welcome today's expert speaker Dr Jeffrey Weber is a senior member director of the Donald a Adam comprehensive melanoma Research
Center of Excellence and professor in the department of oncologic Sciences at mfet Cancer Center as a tumor immunologist and immunotherapy he focuses on translational clinical trials including the development of Novel trials in Melanoma Dr Weber earned his PhD in molecular cell biology from the Rockefeller University and his MD from New York University Medical Center he has published more than 100 articles in the top peer-reviewed journals in his field it's an honor to have you here Dr Weber welcome thank you very much Brian that kind introduction so to today we're going to talk about the concept
of anti-tumor immunity and hopefully at the end of this perhaps 25 30 minute session I'll convince you that the immune system does play an extraordinarily important role in potentially mediating the regression of established cancers I just have to show my disclosures and let's get on to the meat of the matter so first what are the players or who are the players in the immune system keep keep in mind the immune system is broadly divided into two arms there's the so-called innate immune system which is really our first Line of defense inate immunity is pre-existing it's
ready to respond to an infection inflammation or cancer it's essentially a booby trap examples of inate immune cells are macrofagos nutrifil it is not an educated immune system nor is it very selective essentially the inate immune cells kill first and ask questions later the flip side of the coin from innate immunity is the adaptive immunity adaptive immune cells are Called B cells or t- cells and they're educated in the sense that they can learn they have memory and they can recall prior exposure to bacteria viruses tumors or other stimuli and they're very specific and they
have a very selective not a general action it's not a shotgun as much as it's uh think of it as a sniper rifle and again if you compare the innate and the Adaptive immune cells for example if you look at the innate immune Receptors they're encoded in The Germ line in all of our cells whereas adaptive immune cells are in the somatic cells if you look at the receptors inate immune receptors are not clonal they're not specific they're General adaptive immune receptors on the B cells and t- cells they're clonal they're very specific the repertoire
of receptors in a B cell or a t- cell my God it's it's dozens of thousands literally whereas it's very limited in anate immune cells The targets are very specific for the inate immune cells it could be virtually anything for a B cell or a te- Cell B cells and te- cells can even destroy normal tissue they can destroy tumors viruses bacteria inflam you name it recognition of the inate immune cell is perfect but it's not quite perfect for adaptive immune cells and you want your inate immune system to work really fast it's the first
line of defense adaptive immunity takes time so it's slow it Takes weeks to develop and you have memory the Hallmark of the Adaptive immune system of the T cell and the B cell it remembers it can recall that doesn't happen with the uh innate immune system so here are the players and if you look at the left side you can see the Adaptive immune cells pardon me the innate immune cells massed cells which make histamines cause us to have allergic reactions macrofagos natural killer cells basophils eosinophils Neutrophils neut that's your first line of defense against
infection and then there's kind of the cells in between natural killer cells are sort of when they're called a natural killer te- cell they're sort of On The Fringe between anate and adaptive but if you look at the Adaptive immune cells there's your B cell making antibodies and on the right there's the t- cell and that can mature into either a helper cell called a CD4 cell or a killer cell call it a CDA t- Cell and those te- cells well I think of myself as a a t- cell chauvinist those te- cells are are
very important and if you look at the t- cells the First Signal they get to do anything comes when a a piece of a protein a so-called peptide binds to a MHC a major hisst compatibility molecule and when that t- cell receptor on the t- cell binds it has the capacity to recognize but it's not very strong and you need something called a second signal and that second Signal is something on the t- cell which is called cd28 binding to something on well it could be a dendritic cell a maccrage ironically that's in a Nate
immune cell it binds to b71 or b72 that's another signal another we call it a ligan receptor interaction strengthens the interaction of those two cells and then there are multiple potential we call them agonists or antagonists all pairs of a receptor that meets a Lian that can interact to regulate the te- Cells and release sub es from the te- cells that's called cyto release that's the third signal and one te- cell by the way can just cruise around the body interrogating targets it feels its way along a tissue it encounters a cell and if it
has good recognition wow it stays there and starts to differentiate and get activated if it doesn't recognize just moves on they're actually pretty promiscuous little critters one t- cell could literally interrogate thousands of Targets in one day and then here's the picture it shows you the different signals so again signal one is when the t- cell receptor on the t- cell recognizes the MHC molecule with that little green guy that's the peptide that's the piece of protein that's the target second signal two is cd28 me meets up with so-called cd80 or cd86 and this here
this is your innate immune cell that's your dendritic cell it has one job and one job only and That job is to show things to the immune system and then the third signal comes when either the dendritic cell or the te- cell itself starts making cyto kindes and those cyto kindes have the capacity to stimulate lots of other tea cells and then you develop into a helper cell and there are different types of helper cells t- helper one cells T helper two cells so once you get that third signal everything starts rolling very Quickly on
the other hand what are the impediments to the immune system working against tumors well as you know we get cancers there are you know hundreds of thousands of canc cancers diagnosed each year in the United States it's between 500,000 and a million and obviously it works but it doesn't work perfectly and there are many problems or many impediments to successful anti-tumor immunity most of the antigens the things that could be Recognized by your immune tea cells are self-related meaning they're very similar to what would be on a normal cell because after all that's what a
tumor cell is it develops from the normal cell so most of the proteins the potential targets we're tolerant to them we have to be our else we'd all develop autoimmunity if we develop two te- cells that could recognize self antigens they get deleted in embryonic life they're gone we need to do that to protect Ourselves so those te- cells that could recognize tumor related proteins they may be gone and when you treat patients with chemotherapy which even today we do very often for many different types of tumors that really weakens the immune system and the
tumor micro environment boy it has many influences that suppress the immune system it is in incedible to witness how many different ways the tumor has of suppressing immunity it's an amazing defensive system in the tumor You have suppressive cyto mines substances that in normal life are are feedback negative Regulators of immunity because after all we don't want to have the immune system get activated forever you have to have a yin and a Yang but there are high levels of those suppressor cyto kindes and tumors there are even t- regulatory cells which are tea cells that
shut off the immune system and not they don't activate it they turn off we have myoid derived Suppressor cells which are related to some of those innate immune cells like the maccrage and they also have the flip side of the coin they suppress immunity sometimes the tumors modulate off MHC molecules or the very antigens that could be recognized that means they're like a stealth cell they don't get recognized at all or they could directly suppress the immune system by expressing something called pdl1 which we'll hear about in a little while and The immune cells get
stimulated to express their own negative molecules and that's very important for cancer therapy they are called checkpoint proteins because for every Yin there's a Yang every time you activate a te- cell you need a way to turn it off or else we'll all die of autoimmunity well there are these checkpoint proteins those are the breakes every car needs a brake but it needs an accelerator now what do those te- cells recognize well the tumor Antigens are the targets of the immune cells and they come in different categories the best possible antigen is right here on
the left hand side and that's a antigen that is the that develops as a result of a mutation so that only would occur in the tumor would never occur in normal tissue and that is a very specific tumor specific antigen And Then There are a whole bunch of different proteins that are relatively expressed in the tumor they're tumor Specific but they're not absolutely tumor specific for example many of them are expressed in embryonic life and they're shut off by a process called methylation which is these little lollipops here if you unmethylated them they get expressed
it sort of wakens these antigens that were present during embryonic life and they don't really belong in an adult and the tumor can show them to the immune system and sometimes the tumor can recognize those And then there are a whole bunch of other antigens that are relatively expressed on tumors but not on many normal tissues in melanoma those are the so-called melanoid antigens and finally there's the rare antigen that could be recognized by the immune system that's overexpressed simply a huge amount of it allows it to be recognized by the immune system that's pretty
rare one of them would be called p-53 which is a very common antigen and finally relatively Few tumors are virally related but the virus is foreign so if there's a viral antigen made by the tumor that should definitely be recognized as foreign by the immune system so there's a lot of direct evidence that immunity is very important for treating cancer for example immune deficient mice are more susceptible to spontaneous and carcinogen derived tumors a cyto made by tea cells called Incan 2 has anti-tumor activity it works terrifically in mice It works not as well in
people but it definitely can work in people it was the first true immunotherapy approv for melanoma and that was back in 1985 it was first shown in the New England Journal by my old boss Steve Rosenberg and that was ultimately approved in 1998 by the FDA for melanoma and kidney cancer checkpoint proteins those are the breaks on the immune system they can be blocked and the first time that was shown to effectively work in cancer was In 2010 when Steve hod a colleague published in the New England Journal and article showing benefit for patients who
got an anti-la for antibody called ipilimumab that's now an FDA approved drug since 2011 and definitely has benefited melanoma and other tumors and finally you can purify those adaptive immune cells those are the tea cells they call them T tumor infiltrating lymphocytes and if you grow them and then transfer them to patients with Melanoma they can make sure those tumors will shrink there's a lot of indirect evidence that the immune system is important for example in certain histologies for example colon cancer the presence of a te- cell infiltrate in the primary tumor is a positive
factor and that's called the immunoscore and that was uh first put forward by a guy from Paris called jome galone and that was published in science almost 10 years ago in melanoma there are certain factors Associated with a good outcome and one of those factors is whether there are tea cells in the tumor that's a good thing and if there's pdl1 staining on the tumor that's also important that's a reflection of what we call an immunogenic tumor micro environment finally in ovarian cancer if you have a lot of t-regulatory cells they are associated with a
poor outcome so again having lots of the bad guys the t- regulatory cells not a good thing in Most cancers so is there immune response to cancer heck yes can the immune system reject cancer absolutely but as we stated there are many impediments to having effective anti-tumor immunity for example there are many mechanisms of immune suppression just take a look go from left to right in the normal situation here's your activated t- cell t- cell meets up with its Target the antigen presenting cell there's a little antigen there the t- cell Receptor recognizes the antigen
and you have all these other positive interactions that activate the cell those are called the co- stimulatory molecules that's what we call signal 2 but what if the t- cell can't get to where the antigen is what if there's an anatomic barrier it ain't going to happen what if when you have the te- cell meet the antigen there's a substance that kills the cell that's called fast or fast Lian if there's fast On the t- cell and it meets up with fast Lian on the antigen presenting cell it's going to be dead that's called apoptosis
program cell death or what if it meets up with the antigen but there's something that turns off the second signal that's ctla4 well you have an ignorant t- cell there's no activation or if a regulatory T Cell comes up and makes immunosuppressive cyto kindes like il10 or TGF beta you'll have an ignorant t- Cell no activation so there are an awful lot of ways to go wrong and not too many ways to go right in cancer and look at this if you look at this diagram here's your t- cell there are many accelerators on these
te- cells and think of the agonistic molecules as it's like a car and here's the these are all accelerators the problem is these are all the brakes and if you have more brakes and the brakes are working more avidly than the accelerators the te- Cell is going to get turned off and that's what happens in the tumor micro environment you have a lot of ways to accelerate the t- cell the problem is you probably have more ways to put the brakes on so it's a assessment of what's the dynamic interplay between the accelerators here and
the brakes here and every accelerator and every break has something to interact with either on the tumor cell or on the antigen presenting cell so if you have lots of Things interacting with the accelerator you're going to activate the t- cell it's going to be like a car moving forward if you have a lot of things that interact with the brakes you're just going to be permanently on the brakes and that car is going nowhere so that's you look at that Dynamic interplay within the tumor and the big question is okay well the immune system
can recognize cancer is it doing it actively do we have immune surveillance against Cancer and this was proposed by Lewis Thomas and McFarland Bernett and actually McFarland brunnett in part got the Nobel Prize for this something like 30 years ago but it was proposed literally 40 years ago 20 years ago there was a lot of skepticism and there are those who thought it was disproved but thank God and it's to the credit of many scientists including Bob shriber and Jim Allison and many others that this whole idea of immune surveillance Has been resurrected and there's
now a clear concept of immune surveillance that is the immune system constantly on the watch against cancer trying to eliminate it when it arises obviously that doesn't always work but there are three phases there's an elimination phase where both our innate and adaptive friends work together to recognize and destroy a tumor that's trying to develop before it becomes clinically apparent then you reach an equilibrium You're occasionally going to throw off some tumor cells and they're residual occult or hidden tumor cells sometimes they're not destroyed in the elimination phase and they're kind of held in a
state of dorcy or suspended animation and why because there's an Adaptive immune response that's ongoing and as long as that immune response is ongoing the tumor cells aren't going anywhere they're just going to be held in dorcy the problem comes when Something changes a mutation immunosuppressive influence whatever it is that somehow the tumor cells get edited and they are no longer recognized or destroyed by the Adaptive inate immune system they grow and in a diabolical manner they actually induce an immune supressive micro environment within the tumor and then they become clinically apparent so again three
steps three phases and here's a picture here's your normal cells and this goes Counterclock or pardon me clockwise so up top you have your normal cells and eventually you know the tumors are going to get they're going to try to grow the cells become transformed but you go down here they'll summon up your innate and adaptive immune cells which are the multicolored cells and you're going to get rid of these red tumor cells eliminate them and you're protected so a small number of cells May pop up boom recognized by the Immune system eliminated you're in
great shape the problem is over time there's this genetic instability and you select the tumor cells for their ability to evade and avoid the immune system So eventually you reach this difficult equilibrium where some of the tumor cells will grow some of them will be recognized some others will evade and you'll just sort of sit there for a while with a few tumor cells just hanging out the problem is something Will then change and eventually they'll escape and now you get lots of tumor cells begin to grow they're all going to evade and avoid the
immune system and not only that in this amazingly diabolic manner they'll summon up the T regulatory cells so one thing piles up on another you get a snowball effect the tumors grow they bring in the regulatory cells suppresses immunity they bring in the myoid derived suppressors suppresses the anate immune cells now you got a Tumor and that's a real problem and is there evidence for this in an animal well here's an interesting experiment and it's easy to understand so what you do is you actually raise tumors in in an environment where there's no immune cells
in a mouse and that Mouse has a name it's called a rag tumor and you let tumors grow in the rag Mouse and then you transplant them out of this rag Mouse which stands for recombination deficiency and you Transfer them from the immunosuppressed mouse to another mouse who also has no immune system guess what's going to happen the tumors are going to grow nothing is getting they're not being eliminated Etc but what happens you have now the ability to take the tumor tumors that grew in the immunosuppressed mouse put them back into a normal Mouse
it's called WT wild type wild type just means normal immune system now all of a sudden some of them are getting rejected they Stop growing so look down here so isn't that interesting so it says during the process by which they're actually in the immune supressed Mouse they're able to grow once you put them into the wild type Mouse all of the sudden the tumor syst the immune system becomes awakened and now they can recognize the tumor and again going clockwise so we're always going to go clockwise in all these Fancy cartoon diagrams there's always
an inhibitory influence and a stimulating Influence there's a yin and a Yang every step of the way so there's the elimination but there's the editing so you have the accelerator and you have the break so the story of immunity against tumors is there's always this this pushing and this pulling that's going on so if you start at the very beginning releasing the antigens sometimes there'll be tumor cell death that's immunogenic the tumor cell will die and can be recognized by Release of antigens other times the tumors are diabolical they die in a way that hides
them from the immune system and then you'll take those antigens the little red guys and you'll try to have them recognized by the immune system well that's great if the green guys the immune stimulating cyto kindes are around they'll be recognized but if the immune suppressive cyto kindes are around they'll be ignored and then again you deliver these antigens to the lymph Node here's your lymph node and things will go really well in the lymph node if you have the right priming and activating substances present but if the immune cells Express too much of the
break like these things ctla4 pd1 pdl1 nothing's going to happen and then you'll get them out of the lymph node you try to traffic them into the bloodstream and generally things will go well they'll get into the bloodstream but now they'll try to get into the Tumor and if and here this is out of the blood vessel in red into the tumor in white they have to squeeze through the walls and if you're expressing immunosuppressive influences here they're not getting into the tumor if you're expressing these things on your blood vessels well then they will
squeeze through the wall and get into the tumor and finally you're actually at the tumor if the tumor cell doesn't have that which could be recognized it's Ignored it's like a stealth bomber but but if it does have that which could be recognized the t- cell could destroy the tumor and then if in the tumor you express the suppressive influences you're in big trouble unless you express high levels of the immunoactivating substances like interfer on gamma so at every point of the way there's a push and a pole and it's very complicated because there are
plenty of bad guys hanging around and there's one of the Big bad guys the regulatory te- cells and they can inhibit immune responses in many different ways so again this time we're going to go clockwise so inhibitory cyto mines these regulatory te- cells make these cyto kindes that suppress immunity they can directly kill the te- cell they can actually secrete these things called granzyme which latch onto the te- cells and it kills them or they can metabolically disrupt the te- cells by certain cyto kind secretion or They can actually Target the antigen presenting cells right
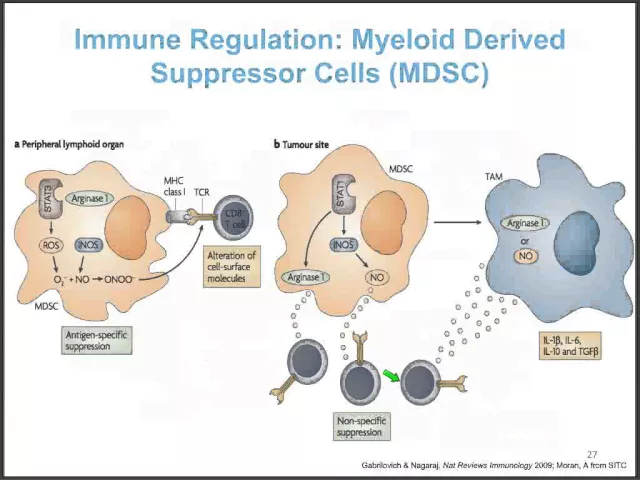
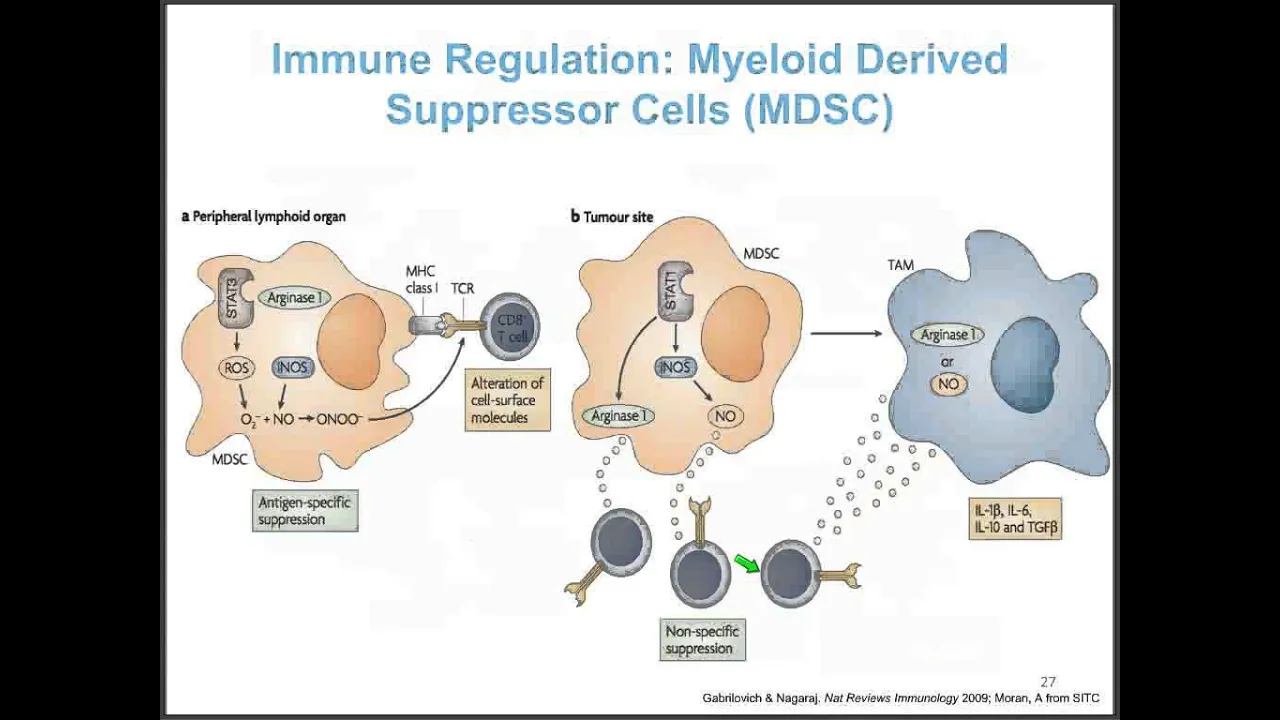
so here here's your regulatory te- cell it'll put the kabash on the antigen presenting cell or it'll convince it to send off cyto kindes that suppress the immune cell so it's amazing how many ways you can go wrong and that was the Adaptive regulatory suppressive cell there's also an innate suppressive cell called a myoid derived suppressor cell because it's derived from the myoid cells which Are the neutrophils the macrophases the monocytes so it's just kind of this big Blobby cell which can specifically present anti to the immune te- cell but it does the double whammy
it shows it the antigen the t- cell starts to get activated then it starts secreting all kinds of nasty things like arginase or reactive oxygen species which absolutely puts down the te- cell and then when it and that's in the peripheral lymphoid organs in the Lymph nodes once it gets into the tumor oh man it starts making all this stuff nitric oxide arginase you name it and it converts the macras from attacking cells into something called a tumor Associated maccrage which means they're useless cells not only are they useless they're actually making cyto kindes that
suppress immunity so it's amazing how many ways you can go wrong and how few ways you can go right and this just again shows it graphically here you are In the primary site of the melanoma if there's a barrier and the immune cells can't get into that tumor they're going nowhere in the lymph node and here down at the uh uh Center it shows the actual lymph node and if we pull our arrow down you'll see here in the lymph node you can go wrong if the t- cell makes ctla4 in the turquoise because it
then is going to latch onto the antigen presenting cell it's going to suppress It alternatively once you get into the tumor so you went from the primary to the lymph node now you're hit sitting in the tumor if the tumor makes pdl1 it's going to bind to pd1 on the t- cell what do you think happens there it acts as a break it's going to shut off the t- cell so you got a real problem and those problems occur anywhere along the pathway so it sounds pretty pessimistic but the amazing thing is for each way
that the tumor tries to suppress Immunity there's a vulnerability and if there's a vulnerability you can attack it and one of the most successful ways we've been able to attack it is with something called checkpoint protein inhibition a concept originated by Jim Allison and Jeff Bluestone and many others that has borne terrific clinical fruit that I'll show you in a few moments you can also try to vaccinate patients and although that's kind of the Holy Grail of tumor immunity I regret to Say there's not a lot of evidence that you can successfully achieve clinical benefit
by vaccinating patients against cancer coming up the road is a whole series of experiments and trials where we can actually pull tea cells out of the patients and instead of them hanging out in the immunosuppressive environment of the tumor we grow them outside the body and we transfer them and those are till tumor infiltrating lymphocytes clonal te- cells we can genetically Transduce te- cells and then we have these chimeric antigen receptor te- cells we call them car te- cells and you're going to hear an awful lot about those car te cells in the future so
cancer vaccines I'm going to dismiss it in one slide there have been hundreds of Trials of cancer vaccines only one cancer vaccine ever approved it's called provenge for prostate cancer it's a cell product made from live cells and it shows surv sural os's overall survival Prolongation has been shown in a randomized trial with this vaccine it's not very toxic but it does not shrink any tumors it does not prolong PR progression so it doesn't change the progression free survival and to be honest it's not widely used in practice in oncology in fact in my own
hospital they don't even have it on the formulary so what does that say yes there is some evidence of benefit to this vaccine but there's not a lot of belief that it Really does much good and that's it's really sad the best antigen in the world and I'll very briefly spend the time here would be what we call a neoantigen so here is a tumor and in that tumor you're going to see mutations in a few of the cells and you can actually isolate those mutated proteins and you can actually synthesize proteins and peptides pieces
of proteins that are from those antigens we call them neoantigens because they're Normal proteins but they're mutated and then they become recognized by the immune system even though the parent molecule cannot and it turns out that in cdat cells that recognize these things the only a very small proportion of these are proteins that are oncogenic proteins the rest of them are just normal proteins they're called passengers and it turns out that we can actually recognize many of these so-called passenger mutations very Interesting so what about checkpoint proteins that's where all the hot action is in
oncology in fact at this most recent ASCO meeting our big cancer meeting in Chicago someone told me this was the immunotherapy ASCO because this is where all the excitement was and let me tell you why checkpoint proteins are the breaks on the immune system the agonistic molecules are the accelerators so if your immune system is a car you Got a break and you got an accelerator one set of proteins limits immunity to avoid autoimmunity and the other enhances immunity and the problem is in the cancer bearing State you got too much break and not enough
accelerator so what are you going to do well you could hit the accelerator or you can cut the brake and ipilimumab is a drug that cuts the break it's a ctla4 activating antibody and that was first approved in 2011 and Definitely benefits those with melanoma pd1 is probably a more important break on the immune system so if you block pd1 it turns out you can generate significant clinical benefit and pisab and noolab were two PD blocking antibodies both approved at the end of 2014 and I'm going to show you quickly some data that I hope
will convince you that these antibodies against pd1 had dramatic benefit in melanoma now it's many other tumors they are beneficial or Have been shown to have benefit in lung cancer had neck cancer ovarian cancer certain types of colon cancer Hotchkins disease you name it almost almost any cancer will show benefit when you block pd1 and this just shows the cartoon on the C cell you got all those brakes and all those accelerators the accelerators are in green the BL brakes are in red you got lots of pd1 on the t- cell and guess what it
recognizes pdl1 on the maccrage it can Recognize pdl1 on the tumor so the tumor itself makes the very substance that binds to pd1 and blocks immunity very diabolical even the dendritic cell that shows the antigens to the immune system makes pdl1 it makes a lot of other things things but blocking the interaction between pd1 and pdl1 particularly in the tumor micro environment turns out to be extraordinarily important why well here's the evidence this was a trial of A pd1 antibody it's called pisab and it was tested in patients who had seen ctla4 antibody impilo map
they were refractory they had melanoma and it was a trial which randomly compared pisab to chemotherapy it was a randomizer what we call phase two study and look at the progression free survival that is the time that it took the patients to start growing after an initial response I think you'll agree that at the doses of pemro used here in Green and red there's no question that they literally look identical and they are clearly superior to the chemotherapy which is shown here at the bottom that's in blue and the difference in time what we call
the progression free survival clearly Superior in pism AB at either dose to chemotherapy alone so no question in one of its first tests when you do a head-to-head trial pd1 antibody beats chemotherapy nine ways to Sunday and then if you look at the other Antibody called noolab and again there are two antibodies out there and this time these are previously untreated patients here the response rate with nool was 40% versus 13.9% with chemo boy that's a lot better that's an easy one but look at the survival this is the survival in sort of a brick
red color of the patients who got noolab who previously had no other therapy we call this first line therapy and this is the survival with DEC carbine Chemotherapy it splits apart very early at three months and it stays apart and what is almost certainly going to happen is this is going to continue and continue and continue and continue and a lot of these patients are going to be alive five years later of the patients with chemo almost everybody's eventually going to die so now in first or second line we have antibodies that clearly provide benefit
and if you look at combining These drugs together the noolab and the ipilimumab and again this is taken out of a um manuscript that was just published a month or two ago if you put both drugs together so you hit two brakes at so you cut two brake cables at the same time clearly Superior in blue for what we call progression free survival compared to just the epilim so again very impressive difference in both response rate and progression free survival for the Combination of killing the brakes twice you block ctla4 and you block pd1 beats
the heck out of blocking ctla4 alone and then if you compare pd1 to ioimo AB and again here's pism ab and we're looking at two different doses or two different uh schedules of pism map every two weeks and every three weeks this is a survival curve and as you can tell it really doesn't make a difference the two pmap schedules are identical clearly Superior to epilim app so again in patients who Were previously untreated you're better off getting the pd1 antibody than getting the ctla4 antibody ctla4 antibody still works but the pd1 antibody works better
suggesting that pd1 is a more important break than c84 these drugs are now being tested in my God 20 different histologies they're thousands of patients being evaluated it's already approved in lung cancer it's going to get approved in head neck cancer bladder cancer kidney cancer Hodkin disease you name it very promising and that's just the beginning I told you there were 10 or 15 braks and 10 or 15 accelerators that's only two out of about 30 think of all the other antibodies that we're going to be able to test now that's checkpoint protein inhibition let's
finish up by talking about Cell Therapy cell therapy is where you actually take the te cells out of the imos suppressive mil of the body and you expand them to huge numbers and you Give them back to the patients sometimes with Incan 2 to make them grow better sometimes you get rid of all the tea cells by giving chemotherapy we call that lympo depletion and here it just shows different strategies if you look at til these are tumor infiltrating lymphocytes that you just grow out of the tumor you can actually take lymphocytes and put a
new T Cell receptor gene into them shown here in Red so that you redirect them so Previously these would be directed against nothing in particular if you isolate the t- cell receptor you want and genetically transfect it you'll make them all into specific te- cells directed against whatever that te- cell receptor recognizes and finally you can graft a hybrid molecule that kind of looks on the outside like a B cell antibody but on the inside it's like a t- cell receptor that's called a chimeric antigen receptor and that's Another way to redirect those lymphocytes to
kill that which you want to Target so again do tilil work well here's a group of 91 patients and 20 of them were complete responders and it showed if you have a complete response which occurs it's about 20% of the time with these tumor infiltrating lymphocytes with il2 look how far out we are this is almost 10 years out these patients are almost surely cured so if you get a complete response to this Tumor infiltrating lymphosan NOA and for someone who's out eight or nine years without progression I'd say they're in pretty good shape to
be cured you can even grow these til and grow them so that they recognize mutation specific antigens from a tumor so this is a cangia carcinoma gallbladder origin tumor and these are tumor infiltrating lymphocytes so T and they were grown because they were stimulated Specifically against one protein called herb B2 2 and this just shows that these te- cells only recognize the mutated herb B2 and they don't recognize the wild type the normal that's why it's called a neoantigen the neoantigen is a mutated Protein that's normal but once it becomes mutated it can be recognized
or unmasked by the immune system and here it shows the tumor burden this was traditional lymphocytes the so-called regular till the tumor grows it shrinks But then it starts to grow again and each one of these lines is an individual tumor but if you give the cells directed against this neoantigen herb B2 whoa everything starts to come down and if you continue this all these go down almost to zero and this particular patient is a near complete responder with tumor infiltrating lymphocytes grown from a cango carcinoma patient that only recognize one neoantigen incredible there are
many ways to skin That cat as I said you can have normal te- cells and this simply shows this is a normal te- cell receptor what if you genetically modified it put in a new one well you just have to change these Alpha Beta chains and now you have a transgenic t- cell receptor that may be of a tumor specific variety but you can put the gene encoding these new te- cell receptor genes into virtually every t- cell on the body and they'll be redirected and here's the cheric antigen Receptor this is the top of
an antibody which is shaped like a y you delete out the rest of the antibody and you Graft in the transmembrane sequence from the t- cell receptor genes so it kind of fakes the te- cell into thinking it's got a t- cell receptor but at the surface it's not the te- cell receptor it's the antibody so again a chimeric antigen receptor and they work incredibly well in hematologic or blood malignancies and I'll just point you to some nice pictures showing bone marrow taken over with chronic lymphocytic leukemia so this is a bone marrow pack with
tumor cells after you treat with these chimeric antigen receptor bearing te- cells the the tumor starts to clear away and then it's almost completely gone by six months after treatment and it just shows that the tumors themselves can disappear so it's truly amazing that simply by taking a antibody against a Substance called cd19 making it into what's called this chimeric receptor sticking it into the immune cells and transferring them back intravenously you can make many leukemia patients completely free of disease so there are 27 trials now going on in which these chimeric antigen receptor cars
are being used against cd19 which is a molecule on B cells and B lymphocytes and thus on B cell leukemias and the response rates are Very high in chronic lymphocytic leukemia CL adult leukemia and pediatric leukemia and it turns out the longer the cells hang out in the body big surprise the better they work and the downside is you can get something called a cyto storm so when you transfer the cells they are so active they work so well they secrete all kinds of nasty cyto kindes which cause side effects you can get CNS symptoms
you can get high fevers and low blood pressure from the release Of all these cyto kindes so the good news is that many patients go in through a mission and stay there the bad news is there are some side effects you're going to hear an awful lot more about these cars because there are folks developing cars for solid tumors not just for the so-called hematologic malignancies so what's the conclusion to all this mostly good news see I told you The bad news in the beginning I told you what all the potential downsides were but now
I'm giving you the good news tumor immune surveillance is a real phenomenon tumor immunity admittedly faces many hurdles due to the escape from elimination of many tumors and tumor antigens these mutated neoantigens as I showed you for that one cangia carcinoma patient and viral antigens and by the way an increasing number of tumors have a viral ideology they may be The best antigens to generate protein immunity nonetheless we've had spectacular success in many tumors with checkpoint protein inhibition especially with pd1 blockade the immune suppressive mechanisms that are the impediments to successful anti tumor immunity that
exist in cancer can be overcome and the rational or the evidence that you can overcome them was shown by those outstanding slides showing clear benefit To checkpoint protein inhibition that I showed you the success of these new adoptive cell therapies with till with the chimeric antigen receptor te- cells the C T cells clearly shows that immune tolerance to cancer can be overcome and the thought I'll leave you with is a thought that I left the audience with a couple of years back at askco when I gave a talk and the line is the best is
yet to Come so I thank you for your attention and I think we have time for questions that's great thank you so much Dr Weber it's uh very exciting to see all the uh different stop signals and the different go signals and while that poses a lot of complications it also provides uh what looks like to be many many opportunities for developing Therapeutics that take advantage of what we now know about how the immune system SE cancer and how it interacts with Cancer uh so thank you very much for walking us through that um I'd
like to remind everyone who is uh watching the webinar that the Q&A pod is now open and you can submit your questions by typing into that Q&A pod I will go through the questions and field them for Dr Weber um in the meantime we do have a few questions that were submitted in advance of the webinar uh the first one Dr Weber is uh our immunotherapies intended to replace the current standard of care or Are they to be added on top of the current standard of care well as as we all know uh there are
many histologies where chemotherapy can induce either complete responses potential cures or certainly clinical benefit in prolonged survival those therapies aren't going to go away in the Frontline therapy with those of the standard of care you know the simple-minded way to look at it is we're going to add immunotherapy to the chemotherapy which surprisingly you can Do many chemotherapies are not that immunosuppressive so you can add chemotherapy to them classic example is nonm cell lung cancer so chemotherapy is not going to go away anytime soon although for melanoma chemotherapy was never particularly promising and I think
that will as I've said in the past go the way of the dodo but for lung cancer breast cancer many other common histologies chemotherapy is going to stay here for a while we'll need Radiotherapy uh for localized disease for symptomatic disease and as a primary modality in head neck cancer and lung cancer interestingly little sideline radiation followed by immunotherapy can lead to spectacular responses and that's because there's somehow the radiation sets up the immune system and primes it to work better so we're not going to see these drugs go away anytime soon so you you
spoke a lot about the The important critical step in the immune response to cancer or where the marker or the antigen or the protein that alerts the immune system to the presence of danger or cancer that that's that's that's key to getting to initiating the the immunity cycle so I've heard that um one way to do that is with cytotoxic therapies like chemotherapy and radiation where you you go in and you kill those cancer cells quickly they release their antigens to The immune system that then pick it up um and Trigger further responses is that
is that what you've seen or is that what you believe well the urban legend is that if you get some evidence of tumor destruction you will effectively Prime the immune system if you have an effective way of completely destroying a tumor and it dies an immunogenic cell death and the answer is yes that's not always going to be the case the abscopal effect at least In melanoma where you radiate and then give AAL liab and in the face of iil liap progression then see responses is pretty rare it happens so it's kind of the exception
that proves the rule but um I think that we're going to see this more and more in other histologies I think the abscopal effect will happen in breast cancer so when you have a really sensitive histology like breast cancer lung cancer sensitive to radiation and You get complete near complete destruction with an immunogenic cell death yeah I think that these things add together no question okay and you you reported some uh depressing results I mean negative results are good in terms of they at least teach us what doesn't work um but I'm I'm speaking of
uh your slides on vaccines and how there really hasn't been despite many many Trials of different types of vaccines um very little evidence of real clinical benefit For patients um now that checkpoint Inhibitors have kind of they're on the ascendency and we're finding that there are ways to combine those with other forms of therapy for benefit to patients do you see vaccines perhaps enjoying a Renaissance or soon to be a renaissance when used in combination with checkpoint Inhibitors I still see issues with the vaccine field um having a potent checkpoint protein Inhibitor will not make
a bad antigen into a better vaccine I think that when we begin to understand how to use the neoantigens viral antigens and the potten antigens that are truly immunogenic combining that with the proper combination of agonistic antibodies or substances and checkpoint protein blockade will generate a successful anti-tumor response where the vaccine will be part Of that combination vaccines alone for cancer I don't see it okay um question about side effects uh what are the typical side effects of IM theapy you mentioned with vaccines for instance that there really aren't or in prenger's case you don't
have very many side effects but what about with things like checkpoint Inhibitors well checkpoint Inhibitors like ipilimumab and pisab and theab as I tell patients it's easy to discuss the side effects of The different drugs because they're all pretty much similar types of side effects we call those immune related Adverse Events and they tend to be organ specific they are associated with the action of the drug sometimes there's some feeling that they're associated with benefit from the drugs but for example you can see rashes caused by a inflammatory infiltrate in the skin you Can see
uh colitis inflammation of the colon you can see hepatitis inflammation of the liver pancreatitis which is inflammation of the pancreas you can see pneumonitis which is inflammation of the lungs and these are often uh asymptomatic um amazingly you can see Sky High abnormalities of the liver which in a hepatitis patient would make them really sick but in a patient getting say noolab pisab they'd have no symptoms which is back Ling you can see Uh abnormalities of the pancreas functions the amas and lipase and the patient will feel happy as a clam whereas if that patient
had pancreatitis from a gall stone or alcoholism they'd be ring on the floor Flor in pain so it's uh you see these characteristic uh inflammatory changes in individual organs for example you could see nefritis and you can see clear inflammatory changes even on a CAT scan of the kidneys but the small bowel that That moves right next to the kidneys perfectly fine so these are bizarre drugs and explaining this to patients is not an easy thing to do uh and then the patients will say well doc why is it that way and you don't have
a good answer why why does uh in one patient the liver get amazingly inflamed uh and in the next patient it's the pancreas or the colon uh sometimes you see multiple organs involved but thank goodness mostly it's individual Organs and we don't know yet I think when you're when you're dealing with individual immune systems you are and individual people you are likely to see the quite a diverse range of respond so it's it's it's a thrill a minute trust me it's never ending excitement and then there are other amazing things that we discover like ctla4
can be expressed on the pituitary the pituitary that's this Little gland at the base of your brain why is it expressing an immune marker and that's perhaps why ipilimumab can induce inflammation of the pituitary which prior to maybe 2002 uh would have been uh a reportable episode that you could publish so it's it's actually very baffling understanding some of the side effects of these drugs here's a question about um kind of the the order of therapy that a patient Might receive so uh for instance epil lium ab noolab and pembrolizumab are all FDA approved now
um but can a melanoma patient start with a pd1 therapy or does that patient have to first fail anti-la 4 therapy well if you go by the package insert Neo as we call it and pemro are approved for those who failed ipilimumab or if they're B mutated a b inhibitor in in fact the national Comprehensive Cancer Centers Network or nccn which helps to set Guidelines for the treatment of cancer patients that is recognized as such as an authority in this country and abroad has recommended with its highest level of recomend Commendation that you can use
the pd1 antibodies in front line before epil liap and I absolutely agree with that and there was a discussion at the plenary session of ASCO by Mike Atkins who's a terrific guy from Georgetown and he basically uh told the audience that he thinks that ipilimumab Is now a second line drug which I think it is pd1 or pdl1 antibodies are the first choice in melanoma and you don't don't have to have failed if liab or a BF inhibitor to go on a pd1 blocking antibody these are very good drugs and the issue is when should
you actually combine them not not when you should sequence them but when should you combine them um and the answer to that question is the jury is still out but at The plenary of course we heard Jed wchar presenting some terrific data showing Major League increased responses PR prolonged progression free survival and improved response rate in those patients with melanoma who got the combo of ippi and Neo compared to either drug alone so on the other hand the the toxicity rate was almost as high as the response rate so there are issues with uh with
these drugs but still the benefit was very Striking uh something that I don't think you touched on in your presentation was anotic uh viral virus therapy in cancer and this is an area that's received a bit of attention with a high-profile television spot I believe it was um viral therapy for a form of brain cancer that had some dramatic results what can you tell us about analytic viral therapy yes the uh I guess it was a 60 Minutes episode uh at Duke in their brain tumor center with a relatively small number of Patients who had
an oncolytic virus directly I believe was directly injected into the tumor bed and those patients have had fantastic survival much better than you would have EXP expect all very encouraging um the most mature data we have for the anotic viruses with something called tve which is a genetically inactivated herpes virus that can't replicate uh but can uh Express something called gmcsf to boost the Immune system it's had some promising results when directly inject a tumor the virus will spread pretty much within the tumor itself and result in a significant immunogenic cell kill it's the perfect
immune priming to combine with checkpoint protein inhibition and right now there's some very impressive data with that combination suggesting that patients who get an initial treatment with this TC into the tumors you kill tumors develop Immunogenic dead cells it acts to Prime the immune system and if you then follow up with hippie Li AB or pisab or noolab uh you might get some very impressive results so that's that's where I think it has some utility all right great well thanks for that we are almost out of time so we'll we'll wrap up with one last
question um in your view Dr Weber where do you see immunotherapy going over the next five years what what can patients Expect well I think that the drugs that were approved in melanoma and lung cancer will be expanded to many other histologies you're going to see large randomized trials um you're going to see new drugs come along things like cd137 antibody Ox 40 you'll see antibodies now prepared against other checkpoint proteins like Vista btla cd244 so there are at least eight potential targets for antibodies that Just kill the brakes there are another eight or 10
potential antibodies or small molecules that hit the accelerator you're going to see increasingly complex combinations um you know we're into double double combos but then you're going to see um triple combinations or quadruple combinations and sequential therapies so it's going to get pretty complicated but I think things for the patients are only going to get better and better and we'll be able to derive a Profile for a patient um uh where prior to treatment you're going to do some either Gene profiling of the patient or uh profiling of the tumor um and uh I think
we'll be able to predict in advance which group of drugs any individual patient should get so for example uh you'll you'll do a tumor biopsy and maybe do a blood test and the amalgamation of those two will tell you Oh no this is a patient where PD antib pd1 antibody wouldn't work you should do epil lium app plus XYZ or we'll now come up with uh new ideas to alter the immune micro environment so that that patient that wouldn't have responded to pd1 antibody would so that's the that's the future the future is combinations and
expansion of of this type of therapy to the major histologies you know the epithelial histologies like Breast prostate colon and lung which accounts for a huge uh chunk of all cancer patients around the world gastric which interestingly is the most common GI cancer around the world probably more than colon uh although not so in the US and really the the tumors that provide major morbidity and Death Around the World you're going to see immunotherapy being applied to them that being said you're going to have to train an entire generation of oncologists to Deal with these
drugs and their unique side effects yes so I I don't I don't anticipate losing my job anytime soon I hope not because uh this has been very very fascinating and I'm sure that uh the people that you work with also appreciate um your your very Charming personality um when you talk about uh you know combinations of things of course um where you're combining two three possibly four drugs uh this is certainly going to raise some questions About affordability and cost um which we don't need to get into today that's not the the topic of today's
webinar but um that I think is also going to be another issue uh going forward as we as the science tells us us that uh these combinations are more effective we'll have to sort out those issues when we cross those bridges so you are absolutely correct um it is something that weighs on the minds of all the investigators um it is something that Weighs on the uh Collective uh consciousness of many of the Pharma biotech companies uh they're all thinking about this because let's face it there's only so much money in the world and there's
there are limits to what proportion of the us GNP can be devoted to healthare we have other things to spend the money on too and ideas on cost Effectiveness and um things like being Reimbursed for example only if you get a response um paying a certain amount of money upfront and then subsequent treatment is free there are all kinds of creative models that I think will be out there and you know in this country there has been much research done by um uh pharmacoeconomics experts and there's there are a few people who are really stand
out around the country and there's one guy who I think at hopk he's at Hopkins I believe named Smith And he's published extensively on this and Americans are willing to pay a certain amount of money per year of Life prolonged and pd1 antibodies because their median survivals are turning out to be very long probably well over two years in front line just for a single antibody clearly provide benefit and the question is how much are you willing to pay and it turns out Americans are willing to pay between 50 and $150,000 per year of life
saved and I Think if we stay in that ballpark hopefully we won't break the bank and we'll we'll stay within a rational range but when it gets above that the question becomes how are we going to afford that so that's that's I'm not an economist but uh that's a question that ways in our minds well with that um I'd like to uh begin our conclusion so once again thank our very generous sponsor amen for supporting today's Webinar also would like to let you know that we have uh two more webinars coming up on the 23rd
and 25th of June uh one is about immunotherapy and brain cancer with Dr David Reen and the other is uh more of a perspective look at what's going to come down the road over the next five years uh elaborating probably at Dr Weber on on what you just said um that's with Dr Jed walchuk on the 25th all of our webinars uh you can register for all of them at cancer research.org Webinars you can also view previous webinars there and if you're a cancer patient or someone who's caring for a cancer patient and you are
interested in learning more about immunotherapy or if you are Healthcare professional Dr Weber you mentioned that we there there will need to be an effort undertaken to train a generation of oncologists and not just oncologists but also oncology nurses and pharmacists um as as cancer treatment develops thanks to breakthroughs in Immunotherapy U resources like uh I'm the answer to cancer which you can get at the answerto cancer.org can be very helpful uh for helping to explain some of the the very basic concepts uh that we are seeing in immunotherapy and we also provide information on
clinical trials there for patients who are looking to connect with an immunotherapy clinical trial so once again that's the answer to cancer.org finally if you'd like to learn more About the cancer research institute and our research funding programs or if you'd like to support our mission uh you can visit us at cancer research.org uh we have a lot of resources there as well and with that um I thank you all again Dr Weber for this very excellent webinar and all those who attended and we look forward to seeing you all at our next webinar thanks
very much thanks bye bye