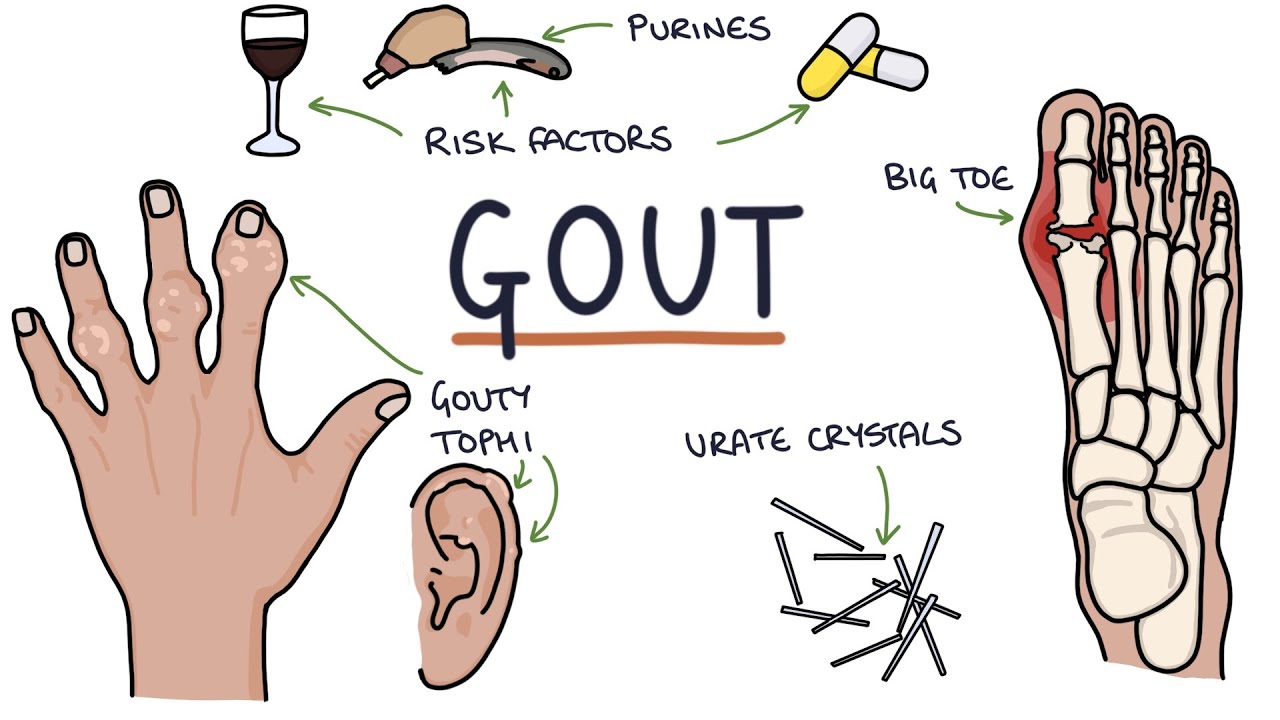
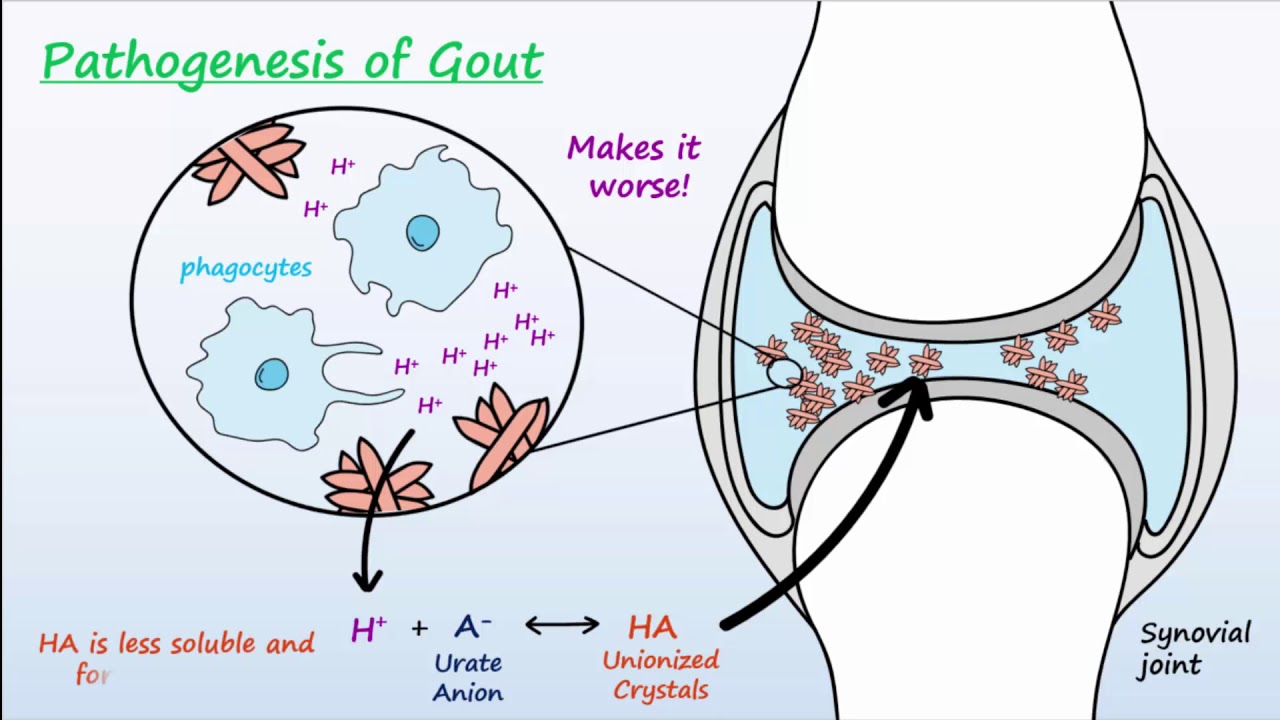
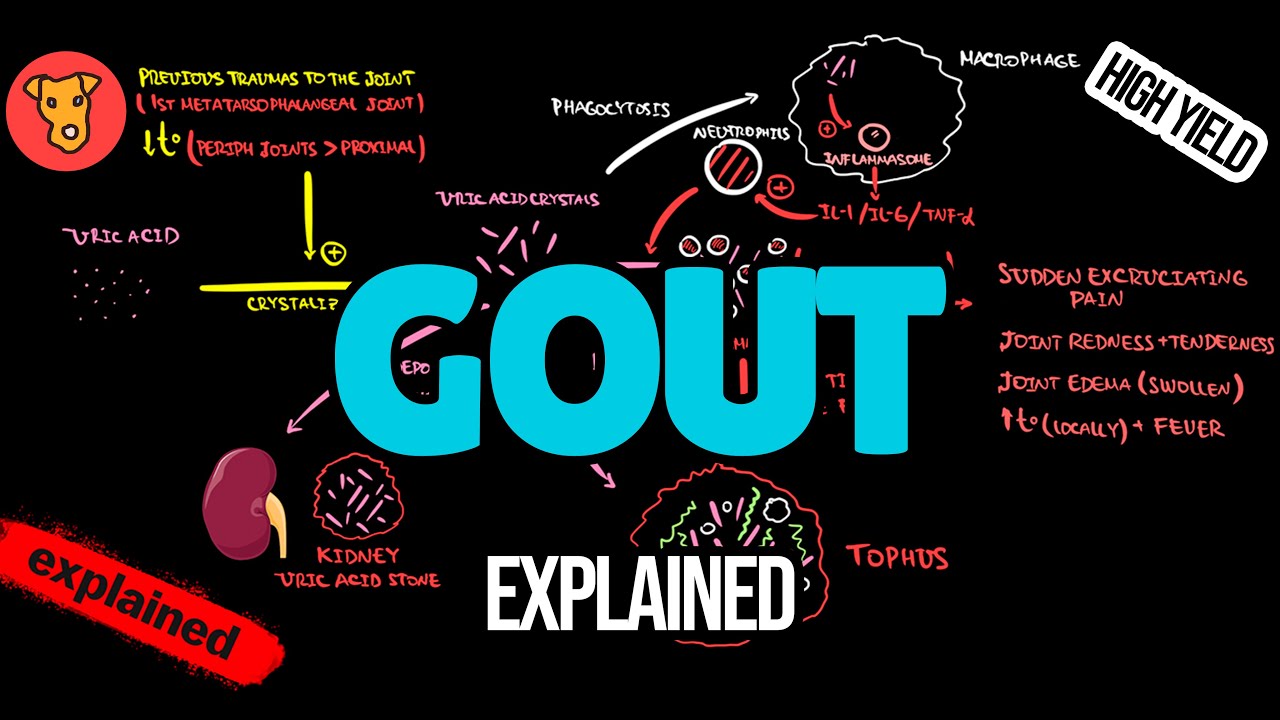
it's medicos perfect metaphor medicine makes perfect sense let's continue our Rheumatology playlists in the previous video we start talking about gout today I'll tell you how can you diagnose gout with that being said now let's get started before we get started let me answer the question of the previous video how can you tell if the patient is an over producer of uric acid or an under X creature of uric acid easy you measure the amount of uric acid in the urine and 24-hour period if you find the uric acid in the urine low therefore by definition the basin is an under excrete err but if there's a lots of uric acid in the urine then definitely the patient is an over producer what do you mean by too much more than 800 milligrams per 24 hours I strongly recommend that you watch these videos in order and my players called Rheumatology we have talked about all of these before if you haven't watched my previous videos I don't know what you're doing with your life crystalline arthropathy are throw joint pathy pathology and it has crystals so inflammatory arthritis caused by deposition of microscopic crystals into joints and other tissue chisel muscle tendon kidney bursa etc gout is an inflammatory arthritis affects the first metatarsal phalangeal joint it's mono articular therefore it's asymmetrical it could be acute or chronic the acute is called acute gouty arthritis or acute gouty attack the chronic is called chronic to fascias gout joint disease is peripheral and none o to immune let's add all of the previous words together to have a definition be out is a crystal and inflammatory asymmetrical mono arthritis that could be primary secondary acute or chronic in over producer or under extruders of uric acid involves small peripheral joints specifically the first metatarsal phalangeal joint or your big toe due to the position of microscopic crystals they are monosodium urate and they are more common in males than females hyperuricemia is not the same as gout a normal serum level of uric acid does not rule out gout gout is inflammatory pain and swelling you can have fever affects small joints pain at night chronic disease with acute flares when you have acute flares you'll find neutrophils joint fluid analysis will show inflammatory pattern inflammatory pattern you have white boxes between 2000 and 100,000 we have high ESR and CRP they are acutely elevated in acute gout and chronically elevated in chronic gout we have discussed this case before this is a patient with an acute gouty attack what's the next step you have to aspire the joint arthrocentesis with joint fluid analysis why to rule out septic arthritis first and then to diagnose our to confirm the diagnosis of gout once you have your diagnosis you can start your treatment and we start by treating the acute attack first and then later we manage the patient chronically by reducing their uric acid level in the plasma we have talked about the risk factors of gout before in the previous video please watch it and don't forget gout is not common in premenopausal women why because estrogen is Yurika Surak it gets rid of the uric acid in the urine which is huge by the way and we will use this fact in trying to treat the chronic gout patients by giving them Eureka szerik drugs what are the causes of gout could be primary or secondary we have talked about them in the previous video what is the pathophysiology of acute gout in acute geard have increased amount of solute what do you mean by salt in this case its sodium you rate because it's gelt if it's pseudogout that's a totally different story usually calcium Tawhid or whatever crystals but now we have sodium urate monosodium urate cool depending on ph and pressure and temperature we form nucleation point and if you remember the flask experiment from the previous video we had nucleation points nucleation points equals crystal formation the fate of the crystal will depend on what happens if the patient and the doctor manage to decrease the uric acid level the crystals will dissolute it will just disappear wonderful risk factors such as trauma inflammation surgery or rapid drop of uric acid because the doctor was an idiot this can lead to crystal shedding from the cartilage to the joint or the purse and this is ugly a different input will give you a different output what will you see in the patient with acute gout clinically the cardinal signs of inflammation which include redness hotness swelling pain loss of function and in Latin this is ruber Keller tumor dollar funky listen I'm having a blast systemic symptoms fever confusion and even delirium yes it can happen because the pain is so severe during recovery disk emission and itching are common we have talked about the difference between Poe dakara and Toph I in the previous video put Agra big toe acute gout mostly in the big toe second most common location Nate you have neutrophils Toph I they mean stone chronic gout chronic to fascias gout VIP and MTP in the hand and the feet the second most common is ear pinna the olecranon of your elbow and your pre patellar burr say these are rocks hard yellowish white chalky nodules multinucleated giant cells are granule own because this is chronic signs and symptoms of acute and chronic gout were discussed in the previous video please don't forget that gout can give you five different conditions now to today's topic how can you diagnose gap between history physical exam and the labs labs what do you mean by that the most common thing of the most important thing is joint aspiration and then serum urine tests and imaging we will need a Rheumatologist a pathologist and a radiologist how can you diagnose gout history male in his 40s meat B or C food drugs trauma surgery fructose all of these are risk factors around for doesn't have to be 40 physical acute gout warm red tender swollen joint the big toe is on fire slabs joint spray-shun is the most important thing arthrocentesis with joint fluid analysis and then in the serum and there and what will we do uric acid in the serum uric acid in there and this is not reliable in the acute attacks also we will need glucose renal function test and lipid why to diagnose concurrent metabolic problems ESR and CRP and white blood cells expect to have neutrophilia in the blood if you have an acute gout and then imaging x-ray and ultrasound x-ray in acute gout normal chronic gout will demarcated erosions these are the trophy the Toph I can cause soft tissue swelling on x-ray and ultrasound will visualize the small crystals a common example is what if the uric acid crystals are so small and you could not palpate them on physical exam do an ultrasound joint aspiration is the most important thing what are you expect to see intracellular needle shaped monosodium urate crystals that are strongly negatively by a refrigerant under polarized microscopy this is just huge before you try to mess around with pathology you need to understand the physiology what's the normal joint fluid aspirate when I aspire a joint what is expected the color should be colorless or straw colored aspect clear not turbid consistency thin and string G viscosity moderate white blood cell differential less than 200 with p. m. ends less than 25% RBC's non-existent or 1 at the very most free of bacteria free of fungi free of viruses glucose slightly lower than that of the blood cell count in the joint fluid analysis normally less than 200 non inflammatory less than 2,000 per microliter inflammatory between 2000 and 35,000 some people say between two thousand and hundred thousand perryland is more than hundred thousand and this is seen in septic Arthur's which one is goat gout is here how about a rheumatoid arthritis flare it's also here mr.
osteo osteoarthritis is here microscopic examination now if you see crystals you get them to the lab polarized light microscopy negative birefringence this is gout positive origin this is pseudogout and here is a table to compare between the joint fluid analysis in each case this is gout clarity translucent to opaque and you can say turbid or white white turbot because of the neutrophil why white because of the crystals color yellow to a pearlescent white blood cells 2000 to 75,000 a pollutant is huge because you know these are crystals so apple isn't a is like a multiple colors together p. m. ends more than 50 because it's acute culture is negative because there is no freakin bacteria okay in order for your test to be diagnostic you need to find at least one intracellular monosodium urate crystals what do you mean by to cellular inside a neutrophil or greater than or equal three extracellular monosodium urate crystals you can obtain the crystals from a joint bursa or at ofus wherever you can do it do it in doofus these crystals are needle shaped monosodium urate strongly negatively by rendered under plane polarized light now what the flip is birefringence and what the frick is plane polarized light this is physics baby pay attention this next segment is not going to be easy it requires you to do without your stupidity for a while after the segment you can reclaim your stupidity back just like how the proximal convoluted tubules reclaimed its bicarbonate back birefringence what does refer engines mean a refraction so let's go back to this this is reflection and this is a refraction does anyone remember physics by the way both of them happen at the same time like it's not like it's either reflection or now if they happen together there is a reflection there is refraction and there is even absorption within the surface that's why when you shine a light on a surface for a long period of time it gets hot because of hate because of absorption let's focus on a refraction from the first medium to the second medium of course the speed of light here is different from the speed of light here that's why there is a refraction and it depends on the speed of light within the medium which depends on the refractive index of the medium it's medium or each substance has a different refractive index water is different from oil is different from crystals by refraction is the same as birefringence what's that having a refractive index that depends on the polarization of light this is not just one refraction this is two reflections in the same substance so here is the first substance which is none birefringence light n refraction and reflection again but this is just one ray here a birefringence material such as the cavity crystals the monosodium urate light n two rays and two outcomes and this is called horizontal polarization and this is vertical polarization I cannot draw 3d but imagine this is one of them and the one of them is like this one is vertical one is horizontal why the flip does that happen imagine that this is your uric acid crystals lovely needle shaped within it there are atoms some of the atoms are horizontal and some of the atoms are arranged vertically and that's why you have by refrigerants so this is a birefringence material suggest the crystals you all have vertical polarization and horizontal polarization and the degree or the angle between them is 90 normally if it's just Mona like not birefringence just a regular material with no birefringence you will get refraction index which is n but if you have something like a crystal and you have two arrays you should calculate Delta n which is the difference between the two refraction indices inside a birefringence material so each substance thats birefringence will have a different Delta N and you should be able to calculate Delta N and you'll find the Delta n for gout is different from Delta n for pseudogout is different from Delta n to any other crystal correct but do you really think that doctors whose primary reason for going into medical school is that they suck at math are going to measure the Delta N and the speed of light and different media in order to diagnose the patient Oh give me a break we want to make it easy so that every dadgum black-coated human being who has an MD in do and B can figure it out so how do we do it use colors if the color is yellow it's good if the color is blue it suited yet look at you but there's a caveat first let's know the difference between a none polarized good old regular visible light and a polarized light what's the difference this light goes in many direction yeah it's still a straight line but in many different directions but this polarized light is only in one direction like this the laser beam is an example of polarized light if it's a true laser not the $0.