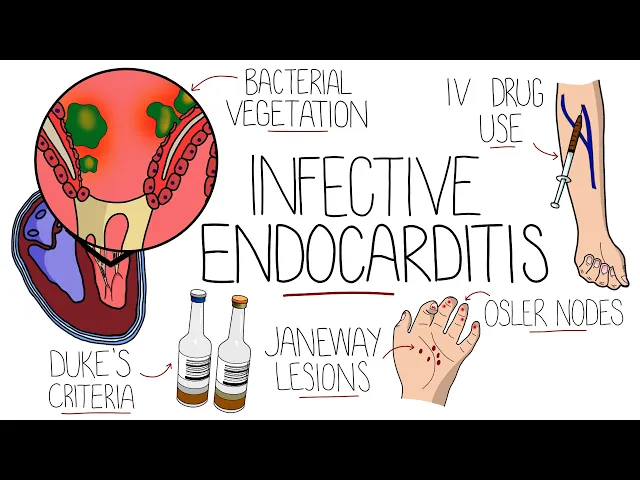
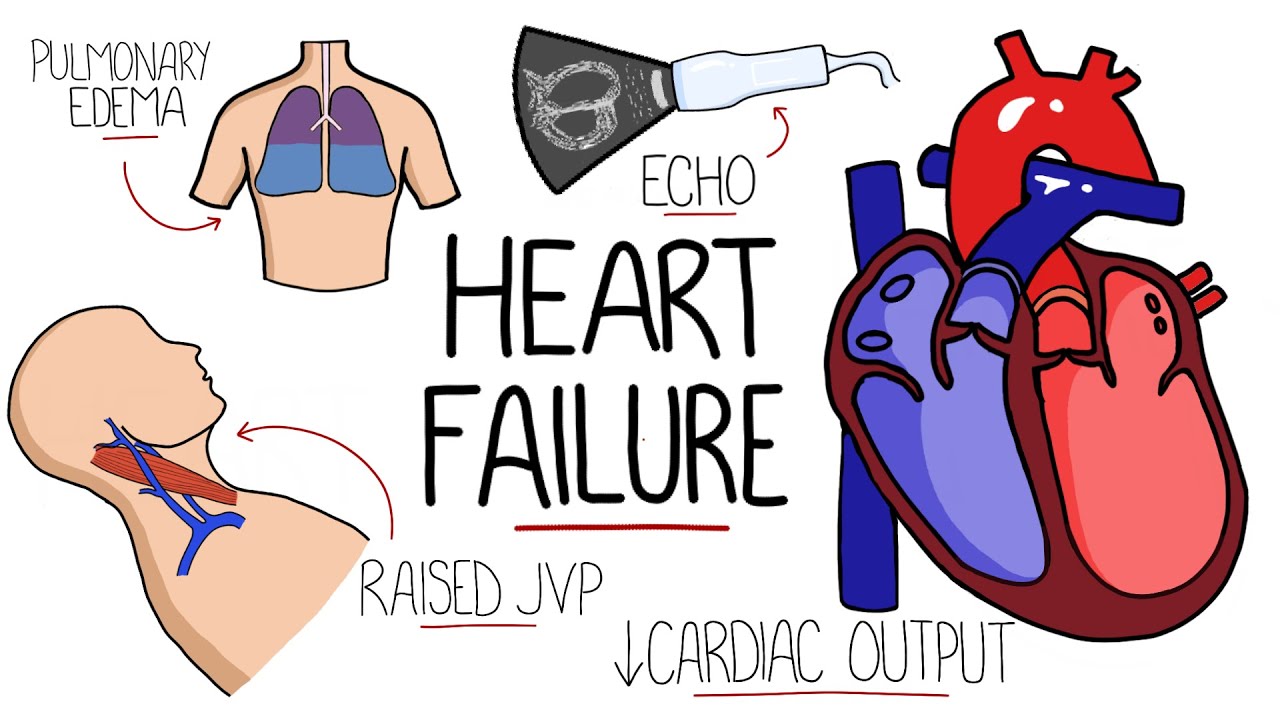
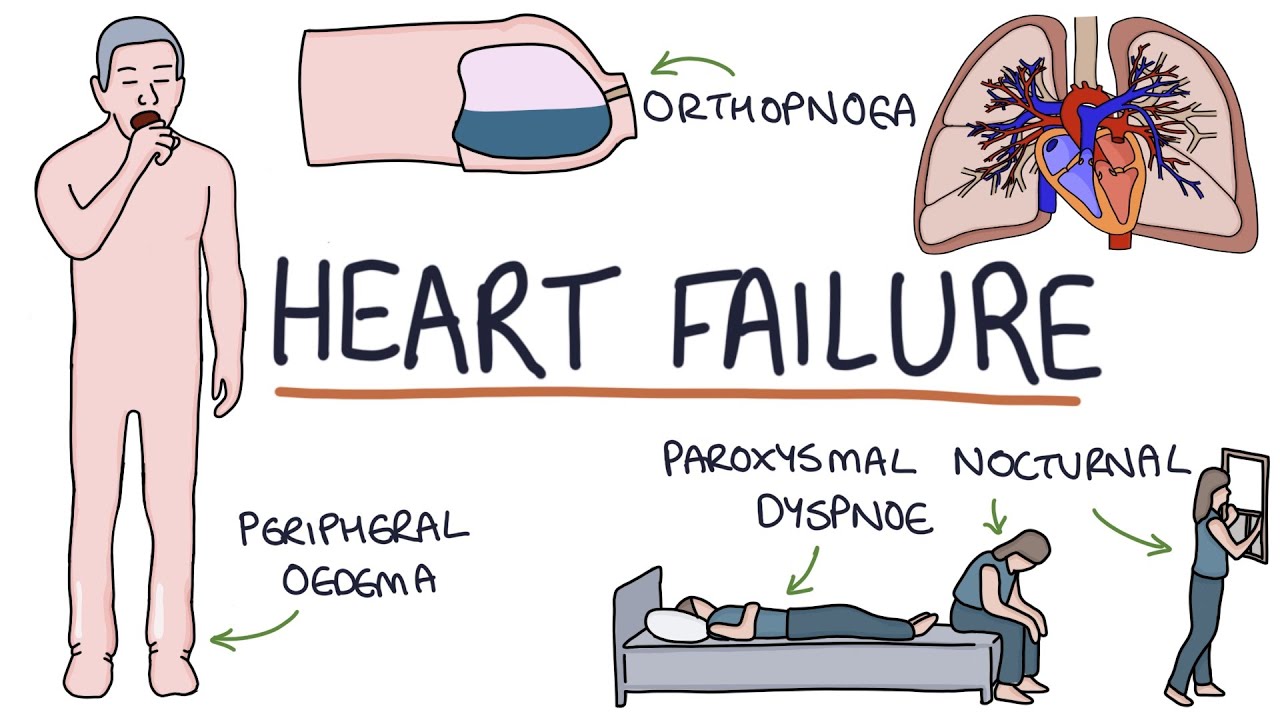
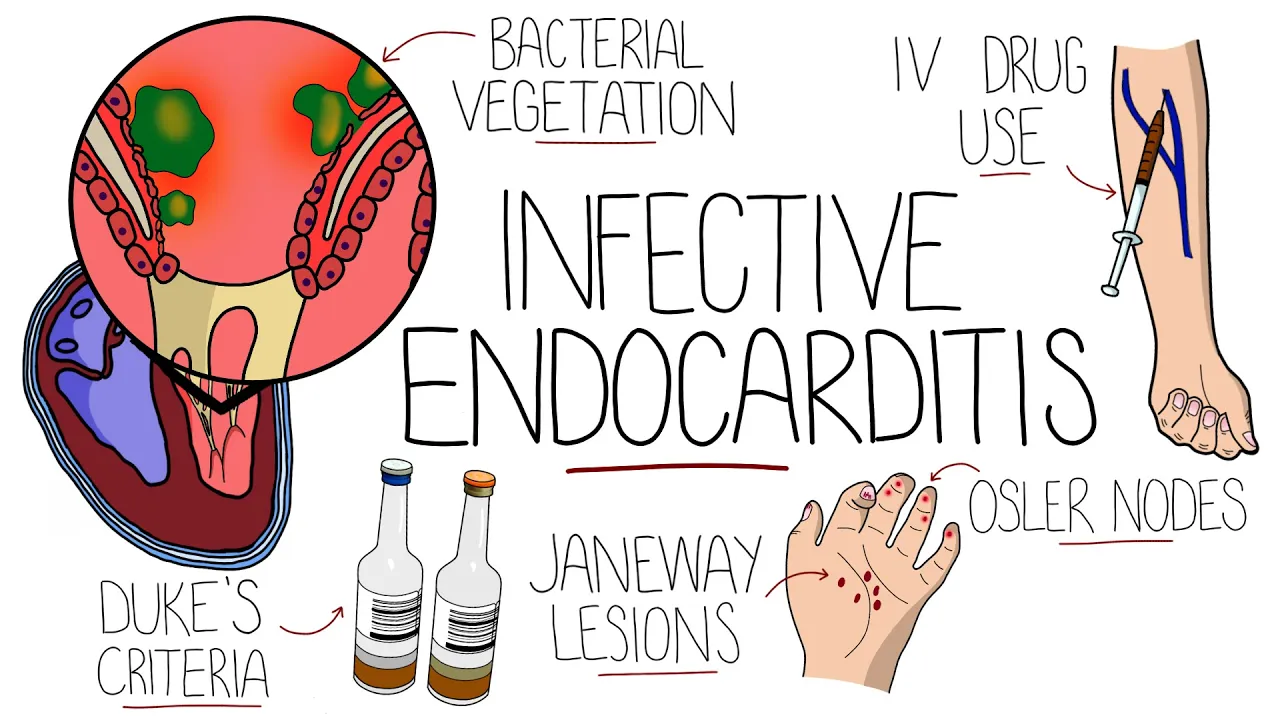
infective endocarditis is a life-threatening infection of the heart specifically the endocardium which is the innermost layer of the heart most commonly this is from a bacterial infection involving the heart valves for infectious endocarditis to develop there needs to be the presence of a bacterial infection in the blood termed bacteremia there are rare exceptions such as a contaminated prosthetic valve being installed bacteremia can come from the transition of bacteria from another infection site into the blood introduction via intravenous drug use and from procedures like dental procedures however the endocardium is normally resistant to colonization by microorganisms therefore for infectious endocarditis to develop there also needs to be an injury to the endocardium this could come from turbulent blood flow direct injury from solid particles injected during intravenous drug use mechanical injury from devices and chronic inflammation such as in autoimmune conditions this injury causes formation of fibrin platelet deposits termed non-bacterial thrombotic endocarditis to which bacteria are able to adhere and to proliferate forming a vegetation that is then covered by a biofilm protecting it particles from the vegetation can also detach and travel along the bloodstream forming septic emboli and therefore can affect other organs that brings us onto the complications cardiac complications include valvular insufficiency most commonly the aortic and mitral valves and less commonly the tricuspid valve ultimately this can lead to the development of heart failure cardiac abscesses can also form most commonly in the aortic root and emboli may travel down the coronary arteries and generate a myocardial infarction the central nervous system is commonly affected including ischemic and hemorrhagic strokes and the formation of cerebral abscesses mycotic aneurysms which are aneurysms caused by infection of the vessel wall can form throughout the body's vasculature but they are particularly common in the cerebral vessels emboli can travel to the kidneys and cause renal infections and immune complexes formed to the emboli can deposit in the kidneys causing glomerulonephritis the spleen is also a common site of embolization leading to infection and abscess formation if the emboli go into the pulmonary circulation such as when the tricuspid valve is affected this can lead to septic pulmonary embolism fever is present in 97 of people often being persistent with no obvious other cause and may be associated with rigors or night sweats fatigue is common and patients may also complain of dyspnea or shortness of breath on exertion and chest pain in some cases hematuria is also possible if there is renal involvement on physical exam there may be a new or changing heart murmur and there may be blackening of the extremities if emboli have reduced the blood flow janeway lesions are painless cutaneous lesions on the palms of the hands and soles of the feet and are the result of micro emboli and splinter hemorrhages can be seen in the nail beds due to capillary injury often confused with janeway lesions are oslar nodes which are painful arithmetic nodules typically on the tips of the fingers and toes thought to be due to a local immunological response roth spots are visible on fundoscopic examination of the eye as small white-centered retinal hemorrhages coming from retinal capillary rupture we've said that bacteremia and a predisposing endocardial insult are typically needed for infective endocarditis specifically structural heart disease is the largest risk factor which used to be commonly from rheumatic heart disease however in the developing world it remains the most common predisposing factor prosthetic valves and cardiac devices like defibrillators and pacemakers are significant risk factors present in around one in four cases of infective endocarditis underlying congenital causes of structural heart disease were present in around 12 percent other factors include intravenous drug use an immunocompromised state which can allow bacteria to reach higher concentrations in the blood another major factor is exposure to healthcare settings which is thought to account for one in three cases in the developed world as we said the infection is usually bacterial and the most common causative microorganism varies by country generally between staphylococcus aureus and streptococci but from recent study averages staphylococcus aureus is present in around 26. 6 percent streptococcus meridian species in 18. 7 followed by other streptococcus species at 17.
5 percent and enterococcus in 10. 5 these make up over 80 to 90 percent of causative agents with the remainder being gram-negative bacteria including the hakket group or fungi like candida albicans infective endocarditis is most commonly seen in patients over the age of 50 which is a relatively recent change because in the early 1900s it was most common in patients under the age of 30.