welcome to this video where we're going to be discussing the mechanism of action of salbutamol also known as albuterol salbutamol is a short-acting beta-2 agonist and an agonist is something which initiates a physiological response when bound to a receptor salbutamol selectively binds to beta2 receptors a beta2 receptor is a subgroup of adrenergic receptor adrenergic meaning receptors which bind adrenaline and noradrenaline therefore when salbutamol binds to a beta2 receptor it mimics the effects that adrenaline and noradrenaline would normally have because salbutamol mimics the effect of the sympathetic nervous system it is known as a sympathomimetic drug
so let's look at the mechanism of action of salbutamol salbutamol works by binding to beta2 receptors which cause a response from the cell on which the receptor is located so the effect that salbutamol has will vary depending on where the beta2 receptor is located within the body beta2 agonists are predominantly used in respiratory medicine to ease bronchospasm but other cells within the body also contain beta2 receptors organs where beta2 receptors are present include the bronchial smooth muscle which is the target site of salbutamol when salbutamol binds to beta2 receptors in bronchial smooth muscle it causes
an intracellular cascade that inhibits contraction of the muscle fibers this leads to relaxation of the bronchial smooth muscle and stops any bronchospasm that the patient may be experiencing such as in asthma attacks or anaphylaxis this relaxation of bronchial smooth muscle leads to an increased airway diameter and an easier passage of air making it easier to breathe another clinically important site where beta2 receptors are found are on the surface of mast cells during an asthma attack or during anaphylaxis these mast cells undergo degranulation which is the release of histamine and leukotrienes that are responsible for bronchospasm
vasodilation and increased capillary permeability stimulation of beta2 receptors on the surface of mast cells will inhibit the release of these inflammatory mediators which is extremely beneficial in asthma attacks and anaphylaxis other sites of beta2 receptors include skeletal muscle spindles which when stimulated increase the rate of contraction which is why patients may experience tremors after beta2 agonist use there are beta2 receptors within the myometrium of the uterus which can cause uterine relaxation there are beta2 receptors within the ureters and when stimulated cause relaxation of the smooth muscle thus reducing urine entering the bladder there are also
receptors within the bladder itself which causes bladder relaxation to prevent the excretion of urine and finally the gi tract reducing gi motility and the secretion of gastric enzymes although there are beta2 receptors present in these different tissues often several adrenergic receptors coexist and there is usually one type of adrenergic receptor that dominates and is responsible for the tissue's adrenergic response now let's look at the intracellular cascade that takes place when salbutamol binds to its receptor in understanding the clinical application of salbutamol this part really isn't important so feel free to skip ahead timestamps are in
the description below because salbutamol is primarily used for its bronchodilatory effect we're going to look at a smooth muscle cell within the bronchi and the intracellular cascade that takes place once salbutamol has bound to a beta2 receptor beta2 receptors are seven trans membrane receptors which means it passes through the cell membrane and does so seven times each of these seven subunits that pass through the cell wall are called alpha helices and an alpha helice is how we describe the coiled shape of an amino acid these seven trans membrane receptors are also known as g-protein coupled
receptors as the name implies these are coupled with g proteins that located within the cytoplasm these g proteins have the ability to bind guanozine triphosphate known as gtp and guanozine diphosphate known as gdp which is why they are given the name g proteins in the inactive form these g proteins are bound to guanazine diphosphate g proteins consist of three subunits labeled alpha beta and gamma which are just the first three letters of the greek alphabet and gdp is bound to the alpha subunit so now we have an understanding of the g protein-coupled structure let's look
at the intracellular cascade that takes place once salbutamol has bound to the receptor on the outer surface of the cell the g-protein-coupled receptor will undergo conformational change this conformational change will cause the alpha subunit to detach from the guanosine diphosphate and will instead bind guanosine triphosphate this will cause the alpha subunit to disassociate from the beta and gamma subunits and will then bind to and activate a membrane-bound protein called adenylyl cyclase some textbooks will refer to this as adenylate cyclase but essentially it means the same thing once activated adenylyl cyclase will use adenosine triphosphate otherwise
known as atp which is the primary source of energy for cells it will remove two phosphate groups and convert it into cyclic adenosine monophosphate cyclic means a circle and in chemistry this will be one form of circular bonding cyclic adenosine monophosphate is just adenosine monophosphate that has been transformed into a circular structure with bonds by adenylate cyclase this cyclic amp will now bring about a response from the cell which makes cyclic amp a second messenger cyclic amp will then act upon protein kinase a and the activity of protein kinase a is directly dependent on the
levels of cyclic amp within the cell remember that a kinase is an enzyme that adds a phosphate group to another molecule known as phosphorylation in this intracellular process protein kinase a is going to phosphorylate so add a phosphate group onto the myosin like chain kinase the myosin light chain kinase is responsible for adding a phosphate group to the light chain of myosin in the presence of calcium and calmodulin thereby activating myosin so that it can interact with the actin causing muscular contraction so when protein kinase a adds a phosphate onto the myosin light chain kinase
it inhibits it from working therefore there is a reduced activation of the myosin which means there is a reduction in the actin myosin cross bridge formation leading to reduced contraction and relaxation or in this specific case relaxation of the bronchial smooth muscle now that we have an understanding of how salbutamol works let's look at its clinical application is most commonly used in respiratory medicine to relieve the symptoms of an asthma attack or other conditions associated with reversible airway obstruction such as exacerbations of chronic obstructive pulmonary disease and anaphylaxis due to the short acting nature of
sabutamol it is used as a reliever therapy meaning patients use salbutamol when they are experiencing symptoms longer acting beta2 agonists can be used in the prevention of symptoms in asthma and copd another use for salbutamol is in the treatment of hyperkalemia salbutamol stimulates sodium potassium pumps within cells which when activated remove intracellular sodium and bring in extracellular potassium this stimulation is achieved through several steps including raised cyclic adenosine monophosphate levels sodium potassium pump stimulation causes an immediate cellular influx of potassium which reduces serum potassium levels however this is also an important side effect of salbutamol
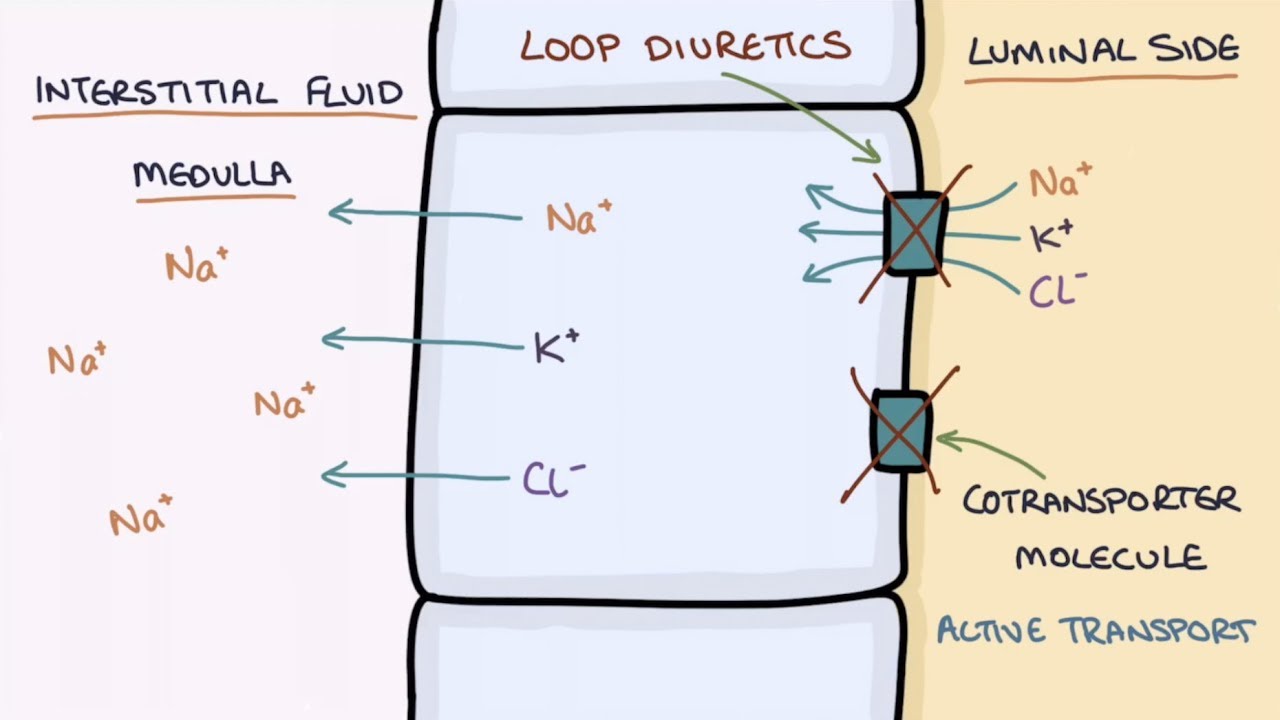
use patients suffering from an acute severe attack may take repeated salbutamol doses leading to a pronounced drop in plasma potassium this will be more pronounced in patients with pre-existing hypokalemia such as malnourished patients or patients treated with loop diuretics the adverse effects of salbutamol result from its stimulation of the sympathetic nervous system common side effects include tachycardia palpitations anxiety tremors hypertension headaches and muscle cramps very rarely sabutamol can also cause hyperglycemia and as we've just mentioned excessive use can lead to hypokalemia to recap salbutamol is a short-acting beta-2 agonist which binds to beta-2 adrenergic receptors
and causes a sympathetic response the main target for sabutamol is the bronchial smooth muscle but beta2 adrenergic receptors are also located on other cells and tissues throughout the body which is what causes some of the adverse effects when salbutamol binds to beta2 receptors in bronchial smooth muscle it causes an intracellular cascade that inhibits contraction of the muscle fibers this leads to relaxation of the bronchial smooth muscle making it easier to breathe salbutamol is commonly utilized in asthma attacks as well as anaphylaxis exacerbations of copd and the treatment of hyperkalemia thank you for watching and i
hope you found this video helpful be sure to check out our other videos on pharmacology and if there are any topics you would like us to cover then please leave a comment in the comment section below