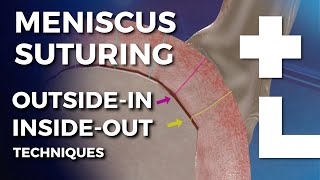
so three certainties in this world are death taxes and if you remove meniscus tissue you will get post menisectomy arthritis why because we increase local contact stresses 65% after partial excision up to 235% after complete excision this is a nice illustrative example showing post menisectomy as a dose response as you remove more meniscus you increase contact pressures over a smaller surface area which leads to post menisectomy arthritis when you're approaching meniscus repair you need to have an entire toolbox in your armamentarium inside out outside in and all inside which we'll be discussing now so what
are the essential elements needed for miniscus repair well it's what I call the ABCs of miniscus repair you need an anatomic reduction you need biologic preparation and augmentation where necessary and circumferential compression critical elements for for successful repair the reason I like speed cinch as an all inside device is it's ergonomically designed it's a one-handed operation it's simple fast I like the 20 coreless Fiber Wire because it's friendly to the meniscus smaller implants means less trauma to the meniscus when we look at the needle design there's a sharp cutting tip and round body that allows
easy penetration with minimal tissue damage and the numbered laser lines are easily readable uh that measures the depth the implant is actively expelled past the needle tip which decreases the depth of penetration and this is very important because it reduces the needle exposure beyond the meniscus why is this important well if you study your MRIs you see that your neurovascular structures are very close to the posterior aspect of the capsule how close are we coming uh well this is a nice paper by the Madrid group that shows on the lateral side of the meniscus from
an ipsilateral portal we're becoming within five millimeters of the poal artery and within s millimeters of the paranal nerve so it's important to perform these procedures in knee flexion as much as possible and it's also nice to have a device that's safe that doesn't increase his exposure beyond the capsule so here's a typical case 23-year-old presents with a locked knee uh confirmed lateral miniscus bucket handle tear this is an ideal candidate for an all inside speed cinch repair remember your ABC's anatomic reduction biologic preparation and circumferential compression your first Stitch is your absolute most important
stitch for anatomic reduction here we use a vertical uh mattress stitch for a vertical longitudinal tear and then we use our not Pusher cutter to really dial in the amount of tension that we want we don't want to over tension these repairs then we move in that danger zone so here rather than performing a vertical mattress suture I like to perform a horizontal mattress suture and this showcases the versatility of the speed cinch here we don't penetrate as far behind the capsule where we're very close to that poal artery and then if we look at
our final construct we'll Place three femoral sided implants and most importantly we'll place two tibial sided implants so it's very important to fix the unders surface of the meniscus why is that unders surface fixation important well if you only fix the top portion you're compressing the femoral side of the tear but you're actually gapping open the medial side of the tear allowing Ingress of sovial fluid and then you only get partial healing what you need is you need circumferential fixation and compression so inside out we did the Stacked vertical mattress technique and this is something
we need to replicate with the all inside technique if we do that successfully you get followup MRIs that look like this where the meniscus is very quiet there's no signal uh we're not wondering if it's healed or not healed as Drew mentioned to you using the curve is very advantageous I'm looking very forward to using that curve bender and that's going to allow us to get the unders surface of the uh meniscus and possibly a reverse curve in the future will also help that undersurface here's another case 15-year-old football player with an ACL tear full
thickness radial tear the postor Horn of the L miniscus we know these radial tears are Sinister tears because as they go through the final 20 to 30 peripheral circumferential collag and fibers we lose our hoop stress when we lose our hoop stress we lose the meniscus function so here we're performing a horizontal mattress suture for this full thickness radial tear and what's nice here is you can see the compression of the tear that knot will eventually go to our first tissue penetration then we know that we're fully compressed here we get a nice robust repair
uh it's very satisfying what about the clinical outcomes of the all- inside uh device so over 730 cases now in the SOS system we want to improve pain and function in our patients so we can see here at 6 weeks pain is significantly reduced in these cases and by 3 to 6 months uh cous ADL for Fung is achieved and very durable over the 2-year outcomes so we're going to transition to the KNE scorpion I think the KNE scorpion has been an absolute game changer for miniscus repair if you haven't had this in your hands
it's absolute must in your meniscus repair toolbox I love it because it's easy to use it's low profile and curved gets in the back of the knee it's single portal uh self- retrieving so it's very efficient it's versatile uses o and 20 suture you can pass a variety of uh Stitch configurations including circumferential horizontal mattress and as Dr Stewart will show you invaluable for root tears here's a 15-year-old patient with a horizontal cleavage tear of the postor horn and body the lateral meniscus the time honored gold standard of course would be to resect one of
these leaflets and feel all warm and fuzzy about leaving some meniscus remaining what does that look like if you look at the contact pressures a is the normal meniscus C this is a single leaflet resection and D is a double leaflet resection you actually there's no difference between single and double leaflet resection for these cleavage tears what we need to consider in select cases is repairing some of these cleavage tears and again it goes back to the ABCs anatomic reduction uh biologic preparation circumferential compression you can see here with the knee scorpion a single pass
self- retrieving through a passport canula gives you a nice circumferential compression Stitch with 20 Fiber Wire here we place them every 5 to 10 millimeters and we get a very nice robust repair when we look at it in the lab uh here's the native meniscus you can see that contact area and pressures are abnormal with the horizontal cleavage tear but restored when you repair it well that's good but how do they do clinically Peter kerswell just published the systematic review in arthroscopy nine studies 98 repairs and demonstrated that the repair rate of horizontal cleavage tears
was very similar to other tears in the literature if you get into a tight medial compartment one Pearl is considered performing an MCL lengthening with the neon valgus you can pepper the femal cided portion of the MCL to give you 2 to 3 millimet of opening and what that's going to do for you is turn it in from Mission Impossible to something that's very accomplishable what about a radial repair with the knee scorpion here's a patient ACL injury and has a double radial tear of the lateral meniscus here the Scorpion is a very nice option
so again we want to achieve an anatomic reduction circumferential compression so we place our first uh suture again very nice that's why I love the Scorpion you can see self- retrieving through your passport canula the other reason I like it is because you can very precisely place your neck suture which allows you to get that anatomic reduction of your tear and then when you're not tying these you can just feel the compression going through the tear uh which is a very nice feature I think these radial tears it's very important uh the strength of your
repair is related to the number of sutures that cross the repair site so one other advantage of the knee scorpion is that it creates a very small perforation that meniscus here we're going to get a total of four sutures in a very small area which gives us a very nice uh robust repair uh that's uh hopefully going to heal for us or at least partially heal when we look at not tying for radial repairs compared to Inside Out techniques uh we find that the not tying actually better resists cyclic displacement then Inside Out sutures and
overall is a stronger construct the final type of tear that we can uh address is a vertical tear and we can do this with a a circumferential compression Stitch we talked about the importance of circumferential compression here we can do it with one pass or one stitch rather than multiple stitches in that stacked vertical mattress configuration the final Advantage is that it maintains normal meniscus Mobility when we suture the meniscus to the capsule we stiffen the meniscus I think it's important that we maintain its normal meniscus Mobility especially on the lateral side near the poas
hiatus so we should consider augmentation of our repairs especially in the sty of an isolated repair that is a repair without an ACL injury we can perform this with a power pick or an all at the notch you see a nice e-lux of marrow elements into the joint and these e-lux of marrow elements have actually been showed very nicely in a goat model to improve the rates of complete healing uh 87% compared to 29% without this bone marrow venting so in conclusion it's important we save as much Native meniscus as possible remember your ABC's a
miniscus repair anatomic reduction biologic preparation circumferential compression the speed sych in my hands has been very efficient and reliable and the knee scorpion provides a versatile approach to miniscus repair and completes your miniscus repair toolbox










![CPR & AED Refresher Course with Nurse Eunice [Adult, Child, and Infant]](https://img.youtube.com/vi/xoXZCDH2bIU/mqdefault.jpg)

