Hey team dr jay gordy here i'm a researcher and lecturer at the university of tasmania and my research mostly is focusing on how inflammation can contribute to disease and in this video i'm going to cover a big piece of research that i've been doing over the last five six years of my life and much of this research occurred at the university of manchester when i was A research fellow and a postdoc i was under the supervision of dr catherine lawrence and professor david broth two amazing researchers and supervisors absolutely fantastic human beings so let me
jump into it the topic is how can inflammation contribute to alzheimer's disease which is a form of dementia the most common form of dementia and i look at whether we can target inflammation therapeutically and it's a Great summary of how i like to approach research i like to use foundational pre-clinical things um such as cell culture model and animal models and then i also like to use big data analysis and that can be of things like rna-seq data sets but it can also be things like epidemiological data like clinically relevant data taken from the human
population with the disease and i can go in both directions i can use the human epidemiological data to inform my Pre-clinical models but i can also use my pre-clinical models to inform how i analyze the clinical data sets and the epidemiological data sets so in this video i'm actually going to cover how i went from a cell model to animal models and then out to big data analysis exploring whether an existing anti-inflammatory might be therapeutic in alzheimer's disease but i'm getting way ahead of myself so let's jump into it right back in the beginning What
the heck is inflammation so here we have a diagram of some tissue we've got a blood vessel running through it and we have an innate immune cell here this is a resident immune cell that will be sitting in your tissues now this differs between where we're looking in the brain the innate immune cell is a cell called the microglia but out in your skin and liver and tissues out there this might be a macrophage so it's sitting in the Tissue and it's surveying the extracellular environment for any perturbations anything going wrong in the environment now
during uh tissue damage so here we have a metal spike being driven into the tissue we damaged the cells of the tissue these are called parenchymal cells which just means tissue cells so in the brain these would be neurons or astrocytes in the liver these would be hepatocytes for example Now when these cells get damaged molecules from inside them come out and these are called damage associated molecular patterns and these can be detected by receptors on or in the resident innate immune cell and that's how the resident innate immune cell detects damage it goes these
molecules aren't normally outside the cell a really classic one of those is atp atp is the energy currency of the cell and it should only be inside the cell at a Really high concentration like five millimolar so when the cell pops it releases the atp and this can be detected by receptors on the surface and inside the resident immune cell another thing that might initiate inflammation is an infection so perhaps when this metal spike came in not only was there damage to the tissue but also bacteria engine now bacteria have molecules on the surface And
within them and they secrete molecules and these molecules are different to our molecules our host molecules so they can be recognized by receptors on or in the resident immune cell and now it has detected either tissue damage or pathogens and these are called pimps these molecules that are released by bacteria and that stands for pathogen-associated molecular patterns so you've got damage-associated molecular patterns and Pathogen-associated molecular patterns now once these receptors are activated what happens next is we need to signal the inflammatory response and that happens through a number of molecules two big groups of those
molecules one is prostaglandins these are a lipophilic inflammatory signaling molecule and so these are derived from phospholipids by lipids and then another one is cytokines so cytokines are protein-based Inflammatory signaling molecules and these are a huge regulator of the immune response here and so cytokines can be released to initiate the inflammatory response too now non-steroidal anti-inflammatories also called nsaids that's non-steroidal anti-inflammatory drugs nsaids they inhibit the enzyme that produces prostaglandins the enzymes called cox and so the cox enzymes produce prostaglandins so if you inhibit those Enzymes you inhibit the production of prostaglandins what are some
examples of insides well ibuprofen aspirin diclovanec naproxen basically all those drugs that you can get from the pharmacy to treat inflammation and pain they target this pathway they inhibit prostaglandins and they inhibit it by inhibiting the enzyme that produces prostaglandins and that's how they block pain and inflammation but once these inflammatory signaling Molecules go out they act on the blood vessel to make it vasodilate and leak so vasodilates to get more more blood to the site of injury or infection which will allow them to get more immune cells and more energy to battle the potential
infection and they become leaky to leak out proteins that might be antibacterial such as complement proteins or antibodies which we've heard a lot about but they'll also become leaky to allow Cells out and to deal with these issues so immune cells white blood cells in your blood can now come out and infiltrate into the tissue and this is why when you roll your ankle it swells up because your blood vessels are swelling and they become leaky and it's also what causes the redness during inflammation so we get cells recruited to the site of injury or
infection and there's a few there's lots of different Cells but a few famous ones one is the neutrophil now this is really interesting so the neutrophil was the most common white blood cell when it gets there it degranulates and in those granules that it releases and the compounds that it releases are enzymes that are really non-specific and just chop up everything because then they can chop up pathogen proteins to disable or kill the pathogen and also are enzymes that produce bleach And you heard me right household bleach chemically identical to household bleach is what neutrophils
produce and they do this for the exact same reason we use bleach in the toilet or whatever to sterilize the area so neutrophils are producing enzymes that produce bleach as well as enzymes that chop up everything there and another thing that happens is macrophages begin to phagocytose which means to eat so they begin to phagocytos The damaged cells or the pathogens going on there now a critical point there is if this response is excessive or chronic it can cause a lot of damage imagine neutrophils pumping out bleach for a very long time months years even
decades which we might see in alzheimer's disease the other thing is the major macrophages or the central nervous system equivalent of microglia phagocytosing if they continue that phagocytotic process they can start to Eat healthy cells and healthy structures right so if these processes are ongoing or excessive you can see how inflammation can contribute to tissue damage this is one of the reasons why we put ice on a rolled ankle for example try and reduce that inflammatory response reduce the pain that goes with it and perhaps some of the tattoo damage going on now inflammation being
bad has been thought For a long time for millennia in fact the greeks thought inflammation was terrible um and in fact they thought inflammation was caused by excess blood and it kind of makes sense right your ankle swells up and becomes red it seems like there's a lot of blood there right so the greeks thought that it was caused by excess blood so they believed you should drain that blood and so this is what led to blood letting or what this person is doing right here they're about To take a blade to that forearm there
to drain some blood to hopefully reduce inflammation now a little side note a little interesting quirk of history this process was done for millennia and it was believed for thousands of years to the point that the doctors who treated george washington still believed in bloodletting three doctors took over a pint of blood each possibly as up to as much as three and a Half liters of blood was drained from george washington because he possibly had maybe a flu influenza he died the next day and so it's quite likely that the doctors contributed to that or
in fact killed him so perhaps this concept of bloodletting killed george washington and it's a bit of an erroneous concept that's bloodletting however the principle that inflammation is bad may in fact be true so although the Greeks were right to say maybe this process is bad they were wrong in their methods so draining blood isn't a good idea now this is a very seminal paper from the 70s now it's from the 70s so the images aren't great but here's what they did they took mice and they depleted one group of mice of neutrophils so they
removed all the neutrophils from one group of mice now neutrophils are the main cells of the inflammatory response Most of your white blood cells are neutrophils so they took one group of mice and they depleted them from neutrophils no neutrophils then to both mice they took a little biopsy of the skin in a sterile manner and then they checked to see how the healing process went how how how did everything go when it healed now this is at a set time point i believe seven days after The skin biopsy was taken and this is the
regular mice now what we can see here um is it's packed full of neutrophils right which actually tells me it's probably a little bit sooner than uh seven days might be around three days or one day so we can see it's packed full of neutrals here each little blue dot here is neutrophils and we can also see over the top here we've just got sort of fibrous connective tissue this is maybe what you Would call a scab right it's definitely not skin yet here in the mice that had no neutrophils so we don't see any
neutrophils here in this injury and this is a little histological cross-section of the skin by the way we can actually see the epithelial layer of the skin is returned so this is normal looking skin here now we've got a bit of fibrous tissue underneath so that's a bit like a scar Tissue and so this is clearly further along the healing process than this this is in a scabby zone this is in you know that sort of um you've still got it's all healed but you can still kind of see the cut it's a little bit
of a scar tissue there but it's way further along the healing process than this and so this shows neutrophils actually slow down the healing process kind of makes sense right neutrophils are there producing Enzymes that chop up everything and producing bleach that sterilizes everything and kills host cells as well you can see how neutrophils aren't doing a great thing there and so you might go well what the heck are the neutrophils doing well remember this is an injury with sterile if the injury was infected then we would probably see a different result the neutrophil splaying
spraying bleach would help protect us from the infection so it's perhaps much of what The neutrophils do is to protect us from infection but in a sterile situation they possibly are causing more damage than they should however inflammation can be good this is a very famous clinical trial so if you get a head injury your brain becomes inflamed and begins to swell and actually your intracranial pressure can shoot through the roof and this can cause very severe consequences your skull is uh can't Expand so if something's expanding inside the skull it can push up and
crush against the skull so the standard medical treatment was to give steroidal anti-inflammatories these are very potent anti-inflammatories that basically mimic your body's stress response to help dampen down your immune function now these steroid anti-inflammatories are so potent that they kind of shut the immune system down to nothing it turns the immune system Off it stops all the processes of the immune system the majority of the processes of the immune system now this was standard clinical practice and a group of doctors said hold on a minute we haven't done a placebo-controlled trial on it perhaps
we should and so they organized and got the funding for a double-blind placebo-controlled trial of steroid anti-inflammatories for the treatment of head injury now it was reported the doctors Were so sure that these steroids would work that they didn't want to enter the clinical trial they did eventually get this clinical trial underway and they managed to recruit 10 000 individuals which is a very large clinical trial it's a good clinical trial and what they found was 18 of people with head injuries died in the placebo group and 21 of people died with head injuries in
the Steroid treated group an absolute increase of over three percent it turned out um and that's a massive effect size and so it turned out the steroids that were shutting off the immune system shutting off inflammation were actually increasing your risk of death and so this tells us that inflammation may be doing good things right if you think about those macrophages phagocytosing up that broken damaged cells that's good right you need to clear the debris right So this leads us to the conundrum right the immune system and the inflammatory response obviously has some good things
and some bad things it's a double edged sword we have the production of toxic compounds we have the phagocytosis of healthy cells and tissues we have but we um we also have delaying of the repair process the repair processes can't get underway until the neutrophils have finished spraying bleach about for Example but then we also had the good side which is phagocytosis of unhealthy cells debris and pathogens and the coordination of the repair processes so many of those cytokines i talked about actually trigger some of the repair processes to allow the tissue to get back
to normal so the inflammatory response has good and bad things so what my research is focused on and what a lot of people are now starting to focus on Is what are some of the molecular switches that we can flip to prioritize the good responses from the immune response and minimize some of those damaging responses going on there must be molecular switches that are flicking on these different responses and can we cause a mostly healthy immune response and so to do that we need to start not using those non-specific Anti-inflammatories that shut down the entire
immune system we need to start looking for things that just flick off some of those bad pathological responses some of those molecules that are involved in the bad pathological responses causing that tissue damage now so i'm researching inflammation and alzheimer's disease now this is eloise alzheimer's he's the person who Discovered and described it this is actually the first patient that was ever diagnosed august data with alzheimer's disease now a great way to just review what alzheimer's is is to look at augustine to the very first patient identified with alzheimer's disease she was 51 years old
and was committed to an insane asylum in 1901 that's what it was called back then it was actually called the asylum for lunatics and epileptics in Frankfurt now 51 years old is very young for alzheimer's disease that's the one unique thing about august ether is it's very young but there's one of the things that caught eloise alzheimer's eye he was like she's very young to have this kind of cognitive deficit now um yeah so most alzheimer's patients between the age of 70 and 75 around six People will be die six percent of people will be
diagnosed with alzheimer's disease and above the age of 85 around about 33 of people will be diagnosed with alzheimer's disease so it's an age-related condition that normally kicks in around that later stage of life not normally at 51 which is very young she was very forgetful and confused these are very common symptoms of alzheimer's disease she had mood swings this is another symptom that Typically kicks in a little bit later um in the disease um and she was eloise this caught eloise alzheimer's idea because she was young and she was very cognitively normal and then
there was sort of a very clear steep progression in the decline in cognitive function such as creation of memories and understanding now when she died around five years after diagnosis which is actually around the rough average uh Uh average time of death after diagnosis so today if you're diagnosed with alzheimer's disease there is an expected lifespan of around five some five years some people live much longer but on average five years after diagnosis now after she died eloise alzheimer's took brain sections from her and stained them and he recognized the three histological hallmarks of alzheimer's
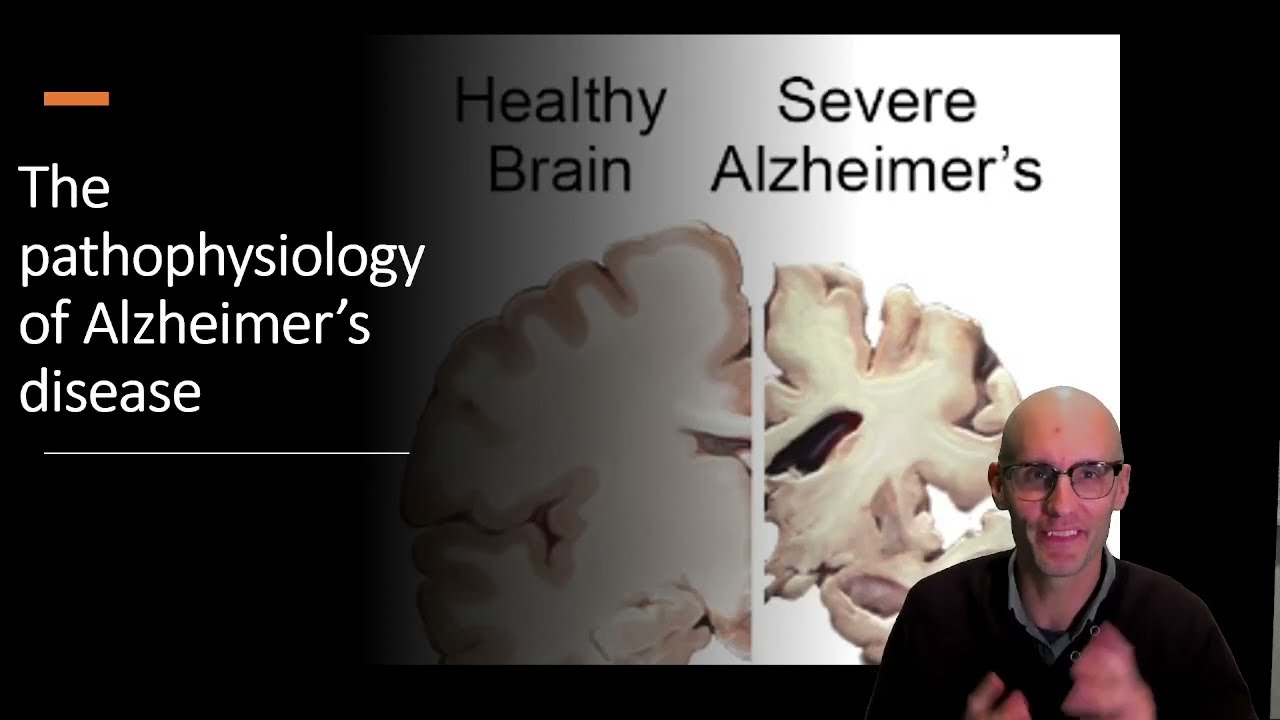
disease right so this is what's going on in the brain in alzheimer's disease We have these extracellular plaques now these right here you can see this very ugly aggregate thing this is a neuron just for context of the brain cell and neuron and over here we have this ugly protein aggregate now this is an insoluble very large protein aggregate it actually gets much larger than this sometimes and so the insoluble protein aggregates that are made up of a protein called amyloid that sticks together and clumps Together and eventually forms this large aggregate in the brain
another thing that we see is intracellular protein tangles so these are extracellular these are outside the cell protein tangles these are inside the cell so it seems like the neurons become stressed and the cytoskeleton the protein structure of the cell can become tangled so we start to see these tangles here this is the neuron and we can see These tangles here and you can actually see it in eloise's alzheimer's slide this is the original slide it was rediscovered this is some of his original slides i should say it was original it was rediscovered in the
90s in munich university basement they found some of eloise alzheimer's original slides and you can actually see the tangles here just at the base of the axon there and there's the tangles there But the third histological hallmark this was identified by eloise alzheimer's in 1906 so well over a hundred years ago were these clusters of non-neuronal cells around those protein aggregates that i was talking about the amyloid protein aggregates we get clusters of non-neuronal cells around it so this is a drawing by eloise alzheimer's and the p here is for plaque and here are these
non-neuronal cells clustering around now that Hallmark that third histological hormone was largely ignored for around about 90 years maybe 85 to 90 years until some people said hey what is going on with those clusters of non-neuronal cells and this is really the first paper that sort of woke us up to the idea of what what they were and the answer is it's inflammation those clusters around those insoluble protein aggregates is inflammation in the brain so this is an immune chemistry stain it's very hard to See in 1991 they identified that the inflammatory cytokine remember those
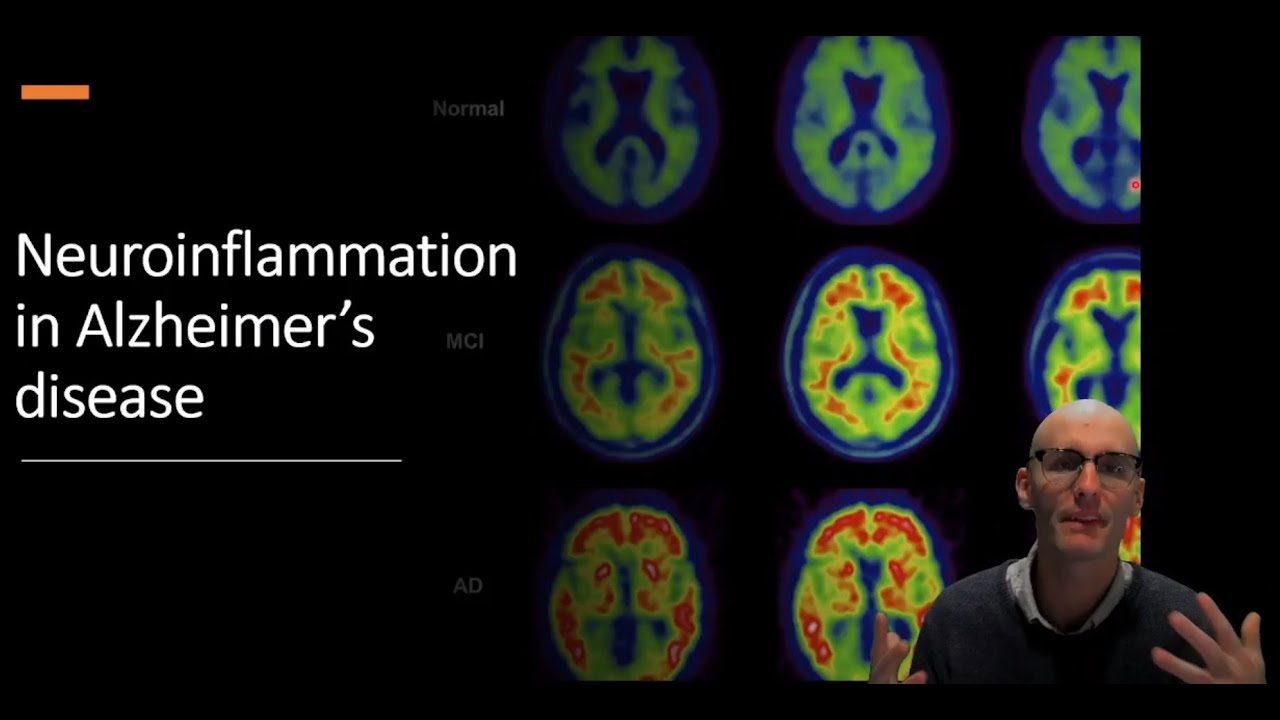
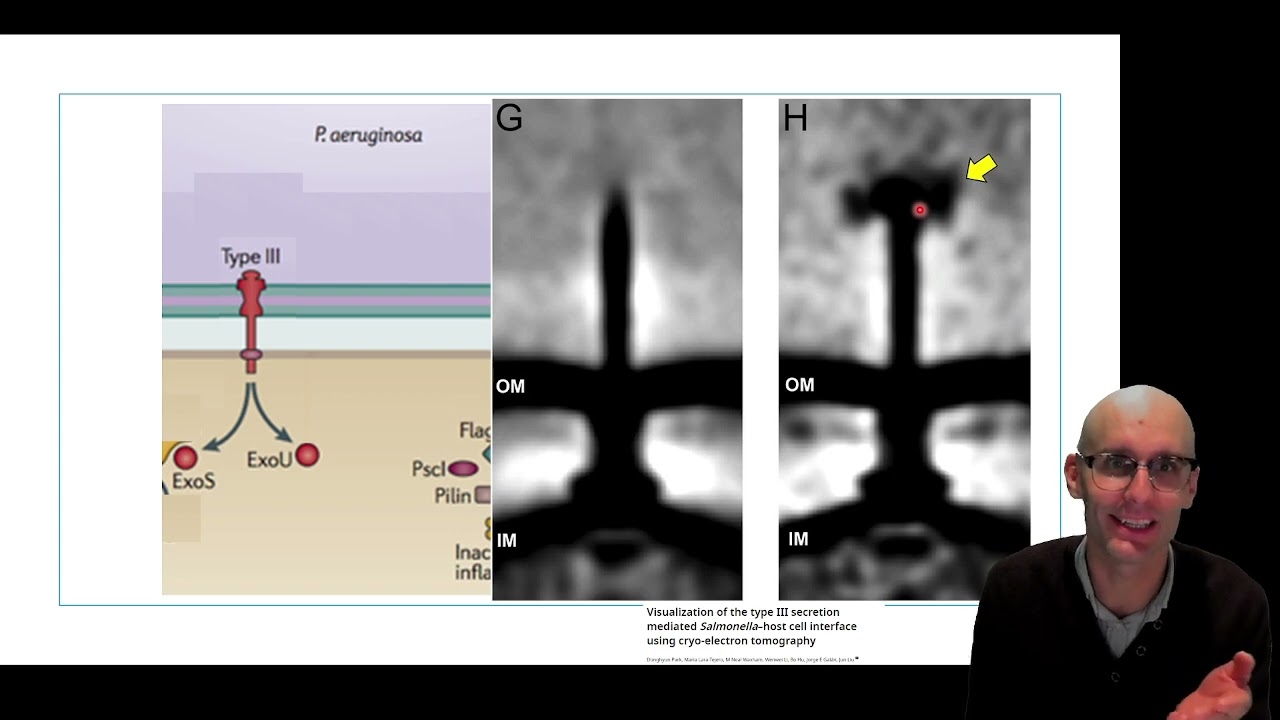
inflammatory protein signaling molecules cytokines the inflammatory cytokine il-6 is expressed in cells around that plaque there um sorry let me just this is so unprofessional i tried to general anyway here we go sorry ah anyway so we've got this Inflammatory cytokine being expressed in cells around the plaque there now obviously we've got more modern techniques now we can actually use pet imaging pet imaging pet imaging with a radio label tag to identify activated immune cells in the brain in particular microglia so this is the radioligand here and this is the brain in a healthy control
and this is the brain and alzheimer's disease so we can see during alzheimer's disease there is massive Neural inflammation going on there is inflammation in the brain now one of the critical things here is that we know that amyloid builds up those protein plaques it builds up in your 50s and the symptoms hit you in your 70s and 80s so you had 30 years of these plaques or 20 to 30 years of these plaques in your brain probably 20 or 30 years of inflammation in the brain imagine cells entering your brain and producing bleach for
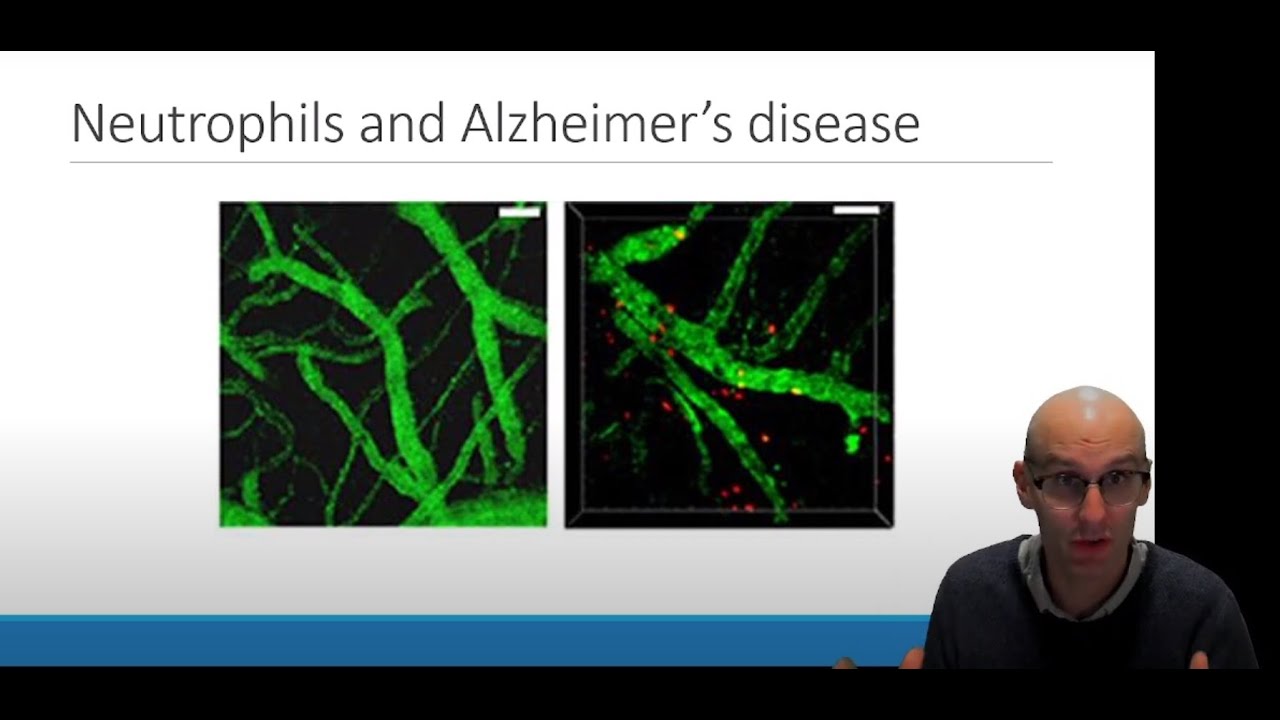
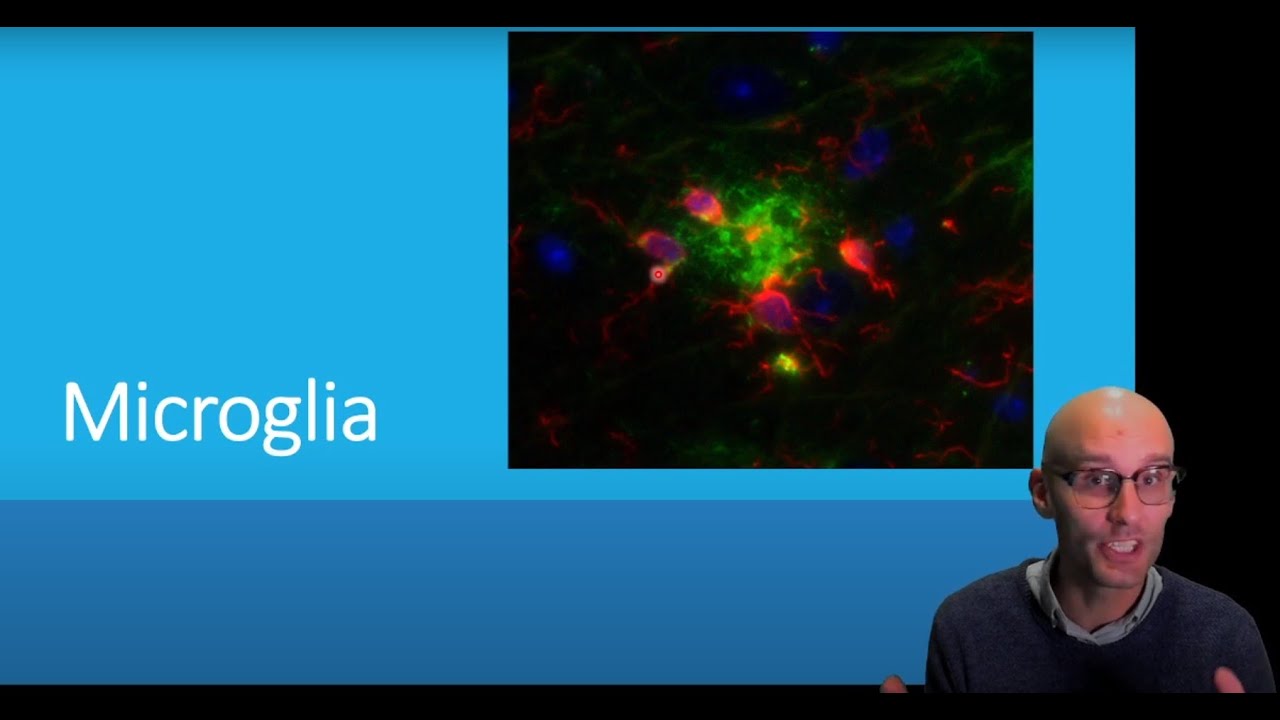
20 to 30 years this could be a Significantly pathological effect going on inside the brain there now this inflammation isn't global pet imaging isn't down to that cellular level so it looked like the whole brain was inflamed but actually it's little pockets of inflammation so this is some of my data here in black we have the microglia the innate immune cells this is a healthy brain section and we can see that the microglia are All spread out and this is what they normally do they're spread out and they have these large processes and they're just
evaluating inflammation going on there no they're evaluating the extracellular environment going on there here is an alzheimer's brain and we can see these punctuated inflammatory microglia these clusters of non-neuronal cells just like what aloe's alzheimer's drew in 1906 these clusters of Non-neuronal cells around those plaques here so there will be a plaque there you can't see it because we haven't stained for it and you can see these clusters of activated angry looking microglia around their plant this is a modern image here this was taken by me as well and here are fluorescently labeled the amyloid
which it makes up that fibular plaque in alzheimer's disease and green and in red are labeled the microglia and so you can see they're clustering around It clearly interacting with it and in yellow yellow as red plus green we have microglia eating the amyloid so they're trying to phagocytos are trying to eat those fibrils and so we can see little pockets of the green in the micro glare as they can attempt to consume the fibrils now here's a big question right so these Liberals um these amyloid fibrils are insoluble so what receptor is being activated
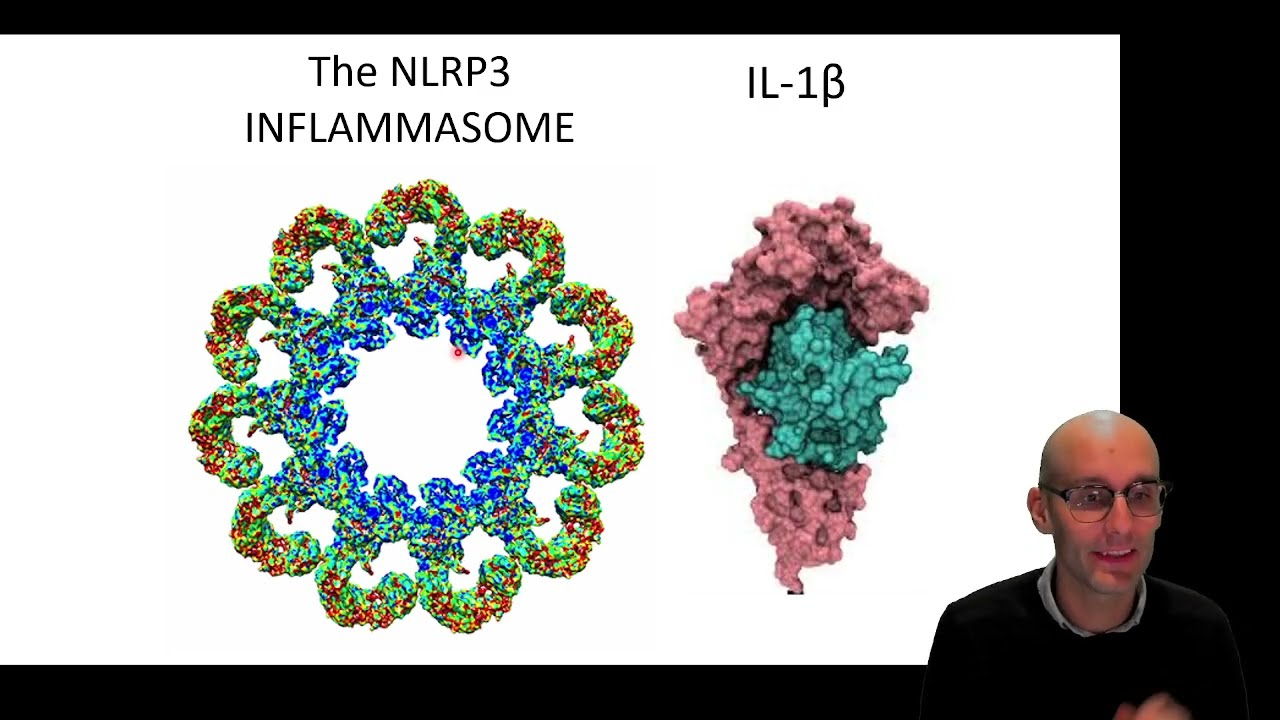
to induce the inflammation going on remember that's the first step that we need for inflammation so we need a receptor being activated so what is that receptor well we now believe this is one of the major receptors involved there's probably many but this is one of the major receptors involved and this is probably the most beautiful thing you've Ever seen in your life and if you're a researcher you're probably considering changing topic right now to research this look at this molecular structure here isn't it fantastic so each one of these each one of these curly
tails here is a receptor called nlrp3 and it's actually a cytosolic receptor so it sits in the cytosol now it's looking for perturbations in the cytosol and when it detects a Perturbation in the cytosol it oligomerizes into this thing here that we call an inflammazone it's a very large protein complex it actually keeps oligomerizing adapted molecules here and it gets so large it gets as big as an organelle so i'll get this big as a mitochondria kind of thing and you can see it um fluorescently down the microscope but that absolutely mess of things very
very beautiful and what are they doing once they're activated what They do is they induce the release of interleukin-1 beta now il1 il1 beta is an inflammatory cytokine in fact it's probably the most potent inflammatory cytokine it never gets up to very high levels in the blood because if it did you would probably die very quickly it's a incredibly inflammatory cytokine we don't typically use it in the clinic as a market for inflammation because it doesn't get up to those high levels because it's so potent We typically use other cytokines that are that are signaled
to be released by ir1 so i one choose causes a whole bunch of more cytokines to be released such as il-6 or tnf alpha and those are the ones we look clinically because they reach higher levels in the blood because they're not quite as inflammatory as il-1 so this is how it goes let me just take you through the molecular process here a little bit so the first thing that we Need is your cells don't normally express pro-ir1 so you need the turning on of the il1 gene now this is regulated by enf camper b
if you're any if you've ever done any sort of uh immune research you'll know the term nfk b it's a transcription factor that regulates so much of the immune response so the first thing we need is that turning on to get to pro ir1 now pro ir1 is an inactive form of il1 it essentially is il1 with Another kind of useless chunk of protein attached to it to turn that il1 off so it's not active and it can't be secreted as a pro form so what we need is that chunk to be chopped off we
need that to be cleaved off and when we cleave off that chunk we get the release of the mature inflammatory cytokine il1 beta so who does the cleaving well an enzyme called caspase one does the cleaving so caspase one chops this useless chunk off causing the release of That now caspase-1 it too is uh produced in a pro form of caspase-1 so it's actually inactive and what we need to get this caspase-1 activator activators we need it to attach to the inflammasome so we need nlrp3 to detect a perturbation oligomerized into that ninja star and
then we get this adapted molecule coming in here that basically connects the receptor to the enzyme and so then once we get the enzyme attached to the Adaptor molecule attached to the receptor it is now activated and it can cleave pro io1 into mature ir1 so it's kind of this two-step process and the reason probably the reason why it's two-step you need the uh turning on of this inflammatory transcription factor nf-kappa b to get this and you need this activation of this receptor it's probably two steps it's like a fail-safe like if you think about
launching A nuclear missile you need to turn two keys in order to launch the nuclear missile that's probably what's going on here ir1 is so inflammatory an inflammation inflammation that's caused by il1 can be so damaging we need those two different processes to turn on in order to be sure that we really want to release it so it's a bit like that nuclear missile with two keys getting turned on now this is a complicated slide i'm very Sorry oh my gosh you shouldn't have this in the presentation um but this is how ir1 release can
be caused by amyloid so this is amyloid at the top here now amyloid can be produced as a monomer but then it sticks together into ligaments and then it sticks together into fibrils and fibrils form those amyloid plaques that i just showed you that we see in alzheimer's disease so it turns out these monomers and ligaments can actually turn on receptors On the cell surface that activate that transcription factor nfk b so we can get amyloid oligomers and monomers turning on some receptors here they're called tlrs and they activate nfk b which causes the production
of that pro ir1 and the nlrp3 protein as well gets turned on from this transcription factor so now we're ready to release i1 we just need that second signal and what's really unique is amyloid is also that second signal so The purples and ligaments can activate receptors or they can cause a thing called frustrated phagocytosis so if you remember back to my immunohis chemistry we showed that there was amyloid fibrils inside the microglia they had eaten the fibrils that's this process here it's eating the fibrils in here now what can happen is if you can't
digest those proteins you can end up with what's called frustrated phagocytosis it's essentially a breakdown of the phagosome Due to the contents of the phagosome so amyloid seems to break down the phagosome and that is one of those perturbations that can be detected by nlrp3 so if the microglia eats something that they cannot digest they get a bellyache there's one way to put it right they get frustrated phagocytosis and that activates the nlrp3 receptor so now we've got the expression and the activation which Causes the release of material il1 which is interesting that it can
all happen from the single protein in different forms so why do we do this why do we have an inflammatory response to amyloid which is an interesting question it is a self protein right we produce it why are we having an inflammatory response to it well one answer is we may be confusing these amyloid species these oligomers and fibrils with a pathogen-associated Molecular pattern so here we have some bacteria streaked on a plate now some bacteria express proteins that look almost exactly like amyloid and amyloid fibrils and evidence for this is one of the stains
for bacteria is a stain called congo red and so we can see this bacteria here is stained in congo red in fact this stain conga red was originally designed for bacteria and it binds to amyloid-like proteins Now the stain can also be used to stain the brains of alzheimer's disease and here we see amyloid plaques here stained and red so these red dots here are amyloid plaques stained with congo red so this stain binds to the amyloid and bacteria and binds to the amyloid in your brain indicating the molecular similarity between these two protein structures
so it is possible especially when we know what receptors uh nlrp3 is what Receptors amyloid interacts with it's possible that our immune system is essentially confusing it with a pathogen and so we end up with a chronic anti-pathogen response in the brain including the production of bleach which is not ideal if it's happening for 20 to 30 years in your brain chronic inflammation now the best evidence for the role of nlrp3 induced inflammation contributing to alzheimer's disease it's this Fantastic paper by michael henniger and doug golembock in 2013 published in nature so here's what they
did this is a mouse and this mouse has been placed in a water maze a water tank a circular water tank and in one location in that tank there is a platform just below the water and so the mouth can't see that platform what it has to do is sort of learn using visual cues the location of that Platform mice don't like to be in water so we place the mouse in the water it wants to find that platform we let it swim for a minute if it doesn't find it in a minute we place
it on the platform and leave it there for a bit we then repeat that process over five days regularly training them about five times a day for five days and over that period of time they learn where the platform is and they start to swim straight to the platform they can remember based on Visual cues where their platform is and they swim straight to it this is called the morris water maze and then we do something a little bit mean is we remove the platform for the final run and we place the mouse in the
maze for 30 seconds and we look where they swim and we build a track map so this is a track map tracking the mouse for that 30 seconds when we remove the platform here's the white dot where the platform Is and this is the water maze here now what we can see is this mouse here this is a normal regular mouse it remembers the location of the platform because it is like i am sure the platform is around here somewhere and it's just swimming back and forth over the top of where the platform was so
that tells us over the previous five days of training it has learned and remembered where the platform is now this is an alzheimer's Mouse model basically we've inserted two human genes that we know cause alzheimer's disease the basically modified amyloid precursor protein and a modified enzyme that chops up that precursor protein now so this is a mouse model of alzheimer's disease and this is the track map of that what we can see is this mouse has no idea where that platform is it's just swimming around in circles so it has not remembered where The platform
is over five days of training this is a thor a sure sign of a loss of memory and a loss of memory is one of the major symptoms of alzheimer's disease so we can see the alzheimer's symptoms here in this mouth now this is where it gets very clever they took a mouse with alzheimer's disease so it had those two alzheimer's genes inserted in it and they removed the gene for the nlrp3 receptor so now these mice Have the alzheimer's genes but do not have that molecular switch that is turned on by amyloid to induce
the pathological inflammation right so they will not have the pathological inflammation going on the bleach production the neutrophils the phagocytosis they won't be having that process because that molecular switch that is turned on by amyloid which is nlrp3 has been genetically deleted from these mice and what we can See is these mice have a great memory they can remember where their platform is so we have not seen the memory deficits that we normally see indicating that nlrp3 induced inflammation is critical to the amyloid-induced memory deficits in these mice right so it's still a preclinical model
but it's a strong indicator that inflammation is a major contributor to alzheimer's disease particularly the inflammation caused by the nlrp3 receptor Now this leads to the central hypothesis of a lot of my research which is factors which influence nlrp3 activity and subsequent r1 release will affect alzheimer's disease progression now i've done two or three big projects looking at can we inhibit pharmacologically using drugs can we inhibit nlrp3 as a therapy as a therapy for alzheimer's disease and another one of my projects is can we synthesize Nlrp3 through environmental factors maybe some of those environmental factors
that increase our risk of alzheimer's disease are sensitizing nlrp3 which accelerates alzheimer's disease or gives us an increased risk now today in this video i'm just going to cover this process here where i go through those preclinical models into human data exploring can we inhibit nlrp3 as a therapeutic target for alzheimer's disease so let's jump into It now what i wanted to research one of the big things i researched is can we find an existing drug that inhibits nlrp3 so these are existing off-patent drugs so therefore very cheap and proven to be safe in humans
because they're an existing drug can we find an existing drug that inhibits nlrp3 so this is what we did and so we explored several classes of drugs loads of different kinds of drugs You know antidepressants all sorts of different drugs but one class of drugs we looked at was insates non-steroidal anti-inflammatories so the aspirin the ibuprofen the declovin act the voltarin that kind of thing uh do any of these inhibit nlrp3 so we know insides inhibit prostaglandins but is there any insights that can inhibit the cytokine il1 that's essentially the first step in this research
So we did a big drug screen and we did lots of different drug screens this is just one of the many drug screens we did so essentially you take a macrophage now we could take microglia but it's just easier to take in cheaper and a little bit more ethical it uses fewer animals to take macrophages so we took macrophages now we treated them with two bacterial toxins one is lps and the other one is nigerian these are two bacterial toxins One causes the expression of il1 and one causes the activation of nlrp3 so these are
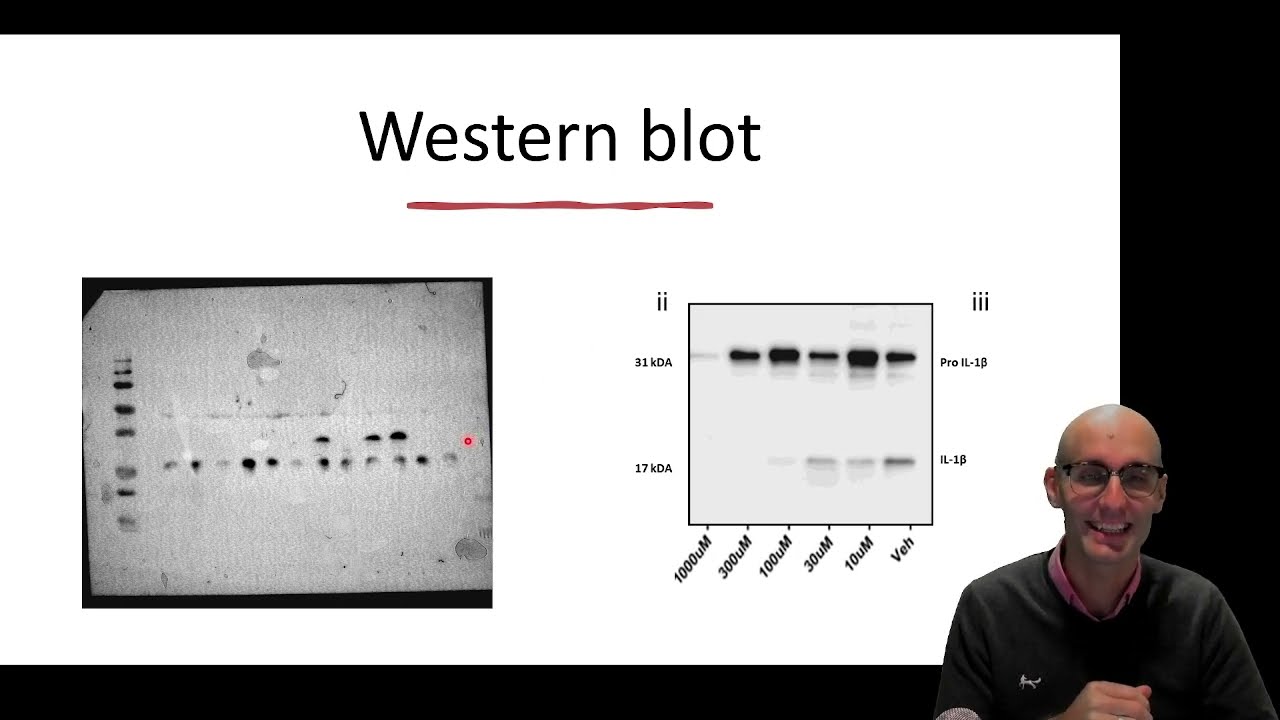
our two keys to launch the nuclear bomb now these have nothing to do with alzheimer's disease but this is just a drug screen to activate nlrp3 it didn't matter how we did it so the critical thing here was we just wanted uh the cheapest easiest fastest way to activate the inflammasome and this is it right here we then measured how much r1 was Released after giving all the different drugs can many of these drugs inhabit it and this is what we found so on the x-axis we have the log of the drug concentration and on
the y-axis we have percentage il-1 release so how much il-1 beta was released here and what we could see is some drugs some insides do not inhibit il1 release so uh ibuprofen sulicoxa paracetamol naproxen aspirin none of those inhibited il1 but two did to Clavinec and methanomic acid now this immediately tells us something the enzymes that are inhibited by nsaids cox enzymes to inhibit prostaglandin production have nothing to do with il1 so these drugs here from naproxen down to ibuprofen all inhibit prostaglandin production but they don't inhibit ir1 these two drugs here do inhibit ir1
as well so something else is going on molecularly speaking that the carbonate And methanoic acid are inhibiting il1 release what's very interesting about this is these are very molecularly similar they're different to the other ones but they're very similar to each other so memphinemic acid to cover it have a very similar molecular structure here so somehow they are gunking up the nlrp3 activation pathway and it's something very specific to the molecular structure which we love that's a great sign when you're doing a drug screen So the next thing is we had to check does that
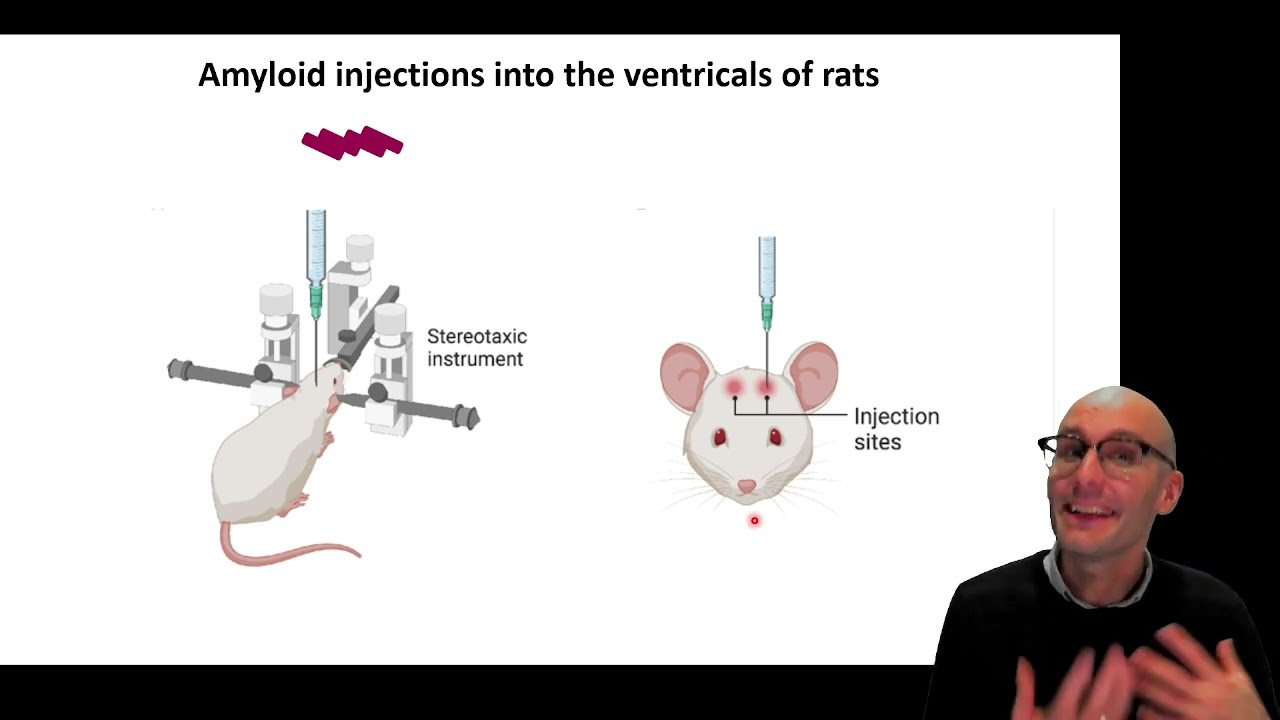
work in an animal so often things that work in cell culture don't work in animals so we needed to do a very simple test to see if we could inhibit the nlrp3 receptor in an animal so to do this we took mice just regular mice and we injected them with atp remember that damage associated molecular pattern atp so atp is normally inside of cells so when it's outside of cells it can Activate receptors one of the receptors that activates um uh is the enol rp3 it's a little bit indirect but it does activate the nlrp3
receptor to call ir1 so we injected atp into the peritoneum then we flush that peritoneum look for il1 and we also look for il1 in the plasma so here we can see here's our control here's our atp treated mice loads of vital ones this is a ridiculously large amount of r1 um And then with the methanamic acid we completely block their production so our nsaids are inhibiting nlrp3 in vivo now we used an established pharmacological inhibitor this sort of had just been invented um of io1 inhibition and it too blocked it and we also used
nlrp3 knockout mice so these mines lack the gene so we shouldn't see the response and indeed we don't so these are just positive controls here and we see basically the Same data in the plasma over here so this is in the blood a complete blocking of ir1 so great our drugs work in cells and they work in animals now we wanted to do this experiment because it's faster than doing an alzheimer's experiment you know it takes a long time and a lot of money and a lot of investment to do an alzheimer's trial so we
want to be sure that the drugs work in vivo and mice before we then go on to A mouse model of alzheimer's disease so this is our mouse model now we don't want to be injecting the mice with our drugs regularly so we use what's called an osmotic mini pump basically they use the fluid of the mouth to power a little pump and this pump will pump out a little bit of drug each day so um it's basically continually leaking a little bit of drug so um we didn't want to use the morris water main
so the morris water maze i Mean that swimming task it kind of relies on stress the mice don't want to be in the water and so if you have a drug that sort of interacts with fear and stress and anxiety you might see an aberrant result we wanted to look at a pure memory one perhaps it was a little bit more ethical so this is called the novel object task it's amazing so mice love novel things they like to explore novel things so if you show a mice a mouse two objects one it's seen Before
one hasn't seen before it will play with the one that it hasn't seen before more often so here we can see a mouse exploring this object it hasn't seen that object before so it's going to play with this object more than that object which it has seen before however an alzheimer's mice can't remember which object it's seen before to them to amount to alzheimer's mouse both objects are novel so it'll play with both objects equally so this is a Way to distinguish the the memory of a mouse can we evaluate the memory of a mouse
using its natural behavior and it's fun for the math the mice love novel things and so it gets to explore a new object so it's great it's got lots of good attributes about it so here's the data here the higher up the bar the more it played with the novel object and the lower the blah the more equal it was it didn't recognize the novel object so here are Our normal mice wildty mice that don't have the alzheimer's genes and they can both recognize the novel object here we have an alzheimer's mouse not recognizing the
novel object at all very poor memory here here we have an alzheimer's mouse treated with mephanamic acid using these mini pumps here and what we can see they're performing basically the same as normal and there's a very significant two-way interaction Effect here so clearly the drug is significantly improving the memory of the mice which is fantastic and so exciting now we also did some histology on here here are our microglia now as microglia become active they pull in their processes so we can sort of score them on how activated they are so this microglia is
very resting this is a little bit activated this is very activated and this is a cluster of very Activated microglia so we can sort of score them on their level of activation so this is a typical alzheimer's mouse now in red we have il1 in green we have microglia we can see that the morphology of the microglia is very activated and we can see that many of these mice are actually microglia are actually full circular microglia just pumping out il1 so they've formed these very tight circular microglia and they're positive for il1 Here's the mephenamic
acid treatment it is amazingly similar to the wild type mice we could not believe it so in research to avoid bias we do everything blinded and i've lined right from the beginning so i didn't know what drug was going in then i blind all the cage cards so i don't even know what cage i'm working with and then so all my behavior is blinded then and i don't even get to unblind that until i've done my histology so Then i do the histology and i was working with a very talented undergraduate student called sophie and
we were on the microscope scoring them taking photos scoring them taking photos it took weeks and then we finally got to unblind the data and it was nine o'clock at night and we i've never had this happen in my career before up until this point all the large numbers of high activation went into one column the alzheimer's Column and all the small no activation went into the other column of alzheimer's mice plus drug and we couldn't believe our eyes we were hooting and hollering in the lab at nine o'clock at night it was one of
the most exciting times of my life it was really really funny it was great oh i and things are smart page just thinking about it unblinding is normally terrifying because it's normally negative normally you don't get a Treatment that works right so it's normally negative data unblinding is normally a sad state of affairs and this was the first time it was ever just absolutely amazing and so here's a graphically this is percentage of activated microglia so here's our alzheimer's mice alzheimer's drug treated mice and this is il1 expressing microglia so that those read positive microglia
and you can see alzheimer's mice alzheimer's drug treatment so our Drug was very effective at blocking inflammation in the mice and preventing cognitive decline in the mice which was amazing but that's mice right whenever you're reading a paper if it's mice you know there's a huge butt there and that's because of this thing called translational failure a lot of drugs that work in mouse models don't work in the human condition for a huge number of reasons it's not because mice aren't Humans i don't think that's the major player there i think there's a whole bunch
of other things we we're in ideal situations humans are not in ideal situations our mice are healthy humans often have co-morbidities they're obese or high blood pressure or they smoke you know there's lots of confounding factors when you go from an animal model to a human model so you always need to check it doesn't work in humans right you need a Clinical trial clinical trials are very expensive very difficult to do especially with drugs that are off-patent there's no money to be made so pharmaceutical companies don't want to run those clinical trials this is why
we need state-funded clinical trials for off-patent drugs anyway so what we're we're to from here well these drugs exist in the real world and people take these drugs for lots of reasons methanoic acid and declover neck Are two nlrp3 inhibiting drugs so i we now applied for and i got access to this data set which followed a cohort of alzheimer's patients for up to 10 years and it's 1600 people and it's cochlear in normal patients people with mild cognitive impairments something in between cognitively normal and alzheimer's disease and people with alzheimer's disease now they follow
these 1600 people for 10 years regularly taking cognitive scores and really Importantly for me they recorded what drugs they were prescribed and taking which was amazing so this allowed us to do to look in this real world human setting do people who take the nlrp3 inhibiting drugs have slower cognitive decline than people who take similar drugs that aren't nlrp3 inhibiting [Music] so we did a clinical data analysis and we wanted to compare these drugs here That worked the the cognitive the ones that inhibit nlrp3 against the same similar drugs right these are all insanes all
prescribed for very some similar reasons um naproxen aspirin silicox with ibuprofen um so we want to compare these drugs that inhibit nlrp3 versus these drugs that don't paracetamol there it's not really an insane it's not a cox inhibitor at biological concentrations but it's Prescribed for very similar reasons so if you have chronic pain like arthritis you might be prescribed paracetamol so it allows us to look at the prostaglandin effects of insides deal with that confounding factor of why are you taking the drug in the first place and then also compare it with these nlrp3 inhibiting
drugs here now in our data set no one was taking methanoic acid this because it's typically prescribed for period pain and So at the age of these uh this cohort we wouldn't see anyone taking methanamic acid but there were a large number of people taking declover neck which is also an nlrp3 inhibiting drug so the first thing i had to do was clean the data now i had this slide it's not really important for you guys but it took me forever so i had to put it in the presentation doctors can't spell not filling out
These data sets so if you can imagine any way to spell a drug it will be in this data set so i had to go through and find every possible way doctors spelled a drug to clean the data so i could score it effectively so there was aspirin aspirin aspirin eps bran you know any possible way to misspell it was in the data set so i had to do a lot of cleaning that's the important part of that okay so the first thing you can Look at is look at time zero right so don't look
at the progression look at time zero what was the prevalence of the disease not the progression of the disease what was the prevalence of the disease so in blue here we've got cognitively normal in green we've got early cognitive impairment yellow we've got late stage mild cognitive impairment and in red we've got full blown alzheimer's disease and these are the proportions in the Non-pain relieving group so in the group that didn't take any pain relieving drugs these are the proportions there now what we can immediately see anyone taking any drug seem to have a lower
risk of alzheimer's disease all these reds are much lower here now this could be due to lots of factors and actually in in my published research in this i go into this that this might be what's called the healthy user bias that healthier patients are more likely To seek drug treatment and so then they're less likely to have alzheimer's disease just by being healthier you know reduced cardiovascular risk factors reduced obesity rates and all that kind of stuff but interestingly early good signs is that diclovanec had the lowest alzheimer's disease prevalence and definitely the much
higher prevalence of cognitively normal so in the group that took the clavinecs the large the Proportions were much more favorable which already is a great indication now this kind of had already been known this is a meter analysis of uh that snapshot data looking at prevalence in nsaids and what we can see is that overall it seems that people who take non-steroidal anti-inflammatories have about a 30 decreased risk in alzheimer's disease and my data roughly sat where that data did it so here's my data here As a prevalence uh drug trial but prevalence isn't what
i'm interested in right clinical trials is when you typically take people who might have the disease or do have the disease you give the drug and you hope for improved outcomes so the thing i wanted to see was progression i didn't want to see reduced prevalence i wanted to look at reduced progression that way we might have a drug where if you've got mild cognitive impairment early signs of Alzheimer's disease perhaps we could give the drug to slow the progression so to do that i had to take the data that followed the neurological scores that
followed the patients over 10 years right so each patient underwent a neurological test and this is what it looks like the money mental state examination actually used two scores the mini mental state examination and the as death score here to evaluate the neurological Function of these patients and it's quite it's quite easy for cognitively normal people what is the year season day day month each of those is worth a point and you the mmsc is out of 30 points and so i wanted to track the mmsc scores of patients who were taking uh declover neck
versus who were taking other nsaids other non-steroidal anti-inflammatories what's the slope look like now the first thing to do that is i need To know what statistical model to overlay the data that's how stats works right so traditionally we know that most data is normally distributed so we assume a normal distribution we plot that model over and we look at how that distribution changes with our explanatory variables like drug treatment for example now a score out of 30 is not a traditional thing to model in statistics And so this you know as a field we've
struggled with what model to apply over it and a lot of people can't find a model and so they binarize the data so they say zero or one that's a very easy statistical model it's called a logistic regression so we say do you have severe alzheimer's disease or not zero or one but that loses a lot of information in the data it's a score out of thirty So importantly what i spend a lot of time hunting out a model that might work for this data set so um in red we have the model and in
white we have the data set so here you can see the data set departs from the model it's not the same so poisson this is a poisson model in red and here's the data and we can see it's not working this is a gamma model here and we can see it's not working but eventually i found quite a rare model that's not used a lot called the Negative binomial model and it's essentially a modified count model which means essentially we're counting the mistakes in the exam right in the mini mental state examination now that's very
technical details but it was a very exciting thing and for my knowledge it's the first time a negative binomial model has ever been applied to this data so this was a cool little breakthrough that i discovered you know exploring this data set so now that we had our Model what we needed to do was to explain away the nuisance variables right maybe there's healthy user bias going on there so maybe in the decarbonate uses there's more people who run a lot and eat healthy so we need to adjust for things like that and so this
is basically the process you build a base model so this is a model and in this model we've got only the explanatory variable of time so over time you expect the scores to go Down so i've included that in my model and then we sort of evaluate how informative the model was then what we do is we include another explanatory variable in our model to attempt to explain the variation in the data and in this case i've got diagnosis here and then we sort of battle these two models and say did it increase how informative
the model was and the answer is obviously Going to be yes because alzheimer's disease people will have a different relationship with time than um people who are cognitively normal okay so um it's increased the informativeness of the model by including diagnosis then we we'll do is include another potentially nuisance variable in here and in this case i've included a risk gene this is the known risk gene for alzheimer's disease called Apoe4 specifically so we include that and we see does it improve how informative the model is again so we battle these two models now this
is a very important step we then remove one of the variables so you can see here i've removed diagnosis and just included apoe and then we checked to see whether the informativeness of the model declined the reason why we do this is perhaps diagnosis and genetic risk factor Explain the same variation in the data so we kind of need to include both things in the model in order to we need to remove it to check whether they're explaining the same variation because the informativeness of the model went down we can see the diagnosis and the
risk gene apple e4 explain different parts of the variation in the data so it's worth including them both in the model so essentially we do this over and Over again include exclude include exclude include exclude until we end up with a perfect model that explains all the nuisance variables right it gets rid of all the noise in the data so now we can look at what our drugs are doing in the model so now we essentially repeat the process we've got our full model here this has explained all the nuisance variables and now we include
the drug in the model and see did it significantly improve the Informativeness of the model and we can see in this case it has now this is a very important step we then look at indication so indication a drug indication is why you would take the drug so we include the drug in the model and then we include why you would take it so is it arthritis it's a back pain it's a headache we include that variable in the model because it is highly possible that the reason you take the drug and The drug are
explaining the same variation in the data so perhaps you know in a in a kooky world perhaps osteoarthritis protects you from alzheimer's disease we needed to check that statistically so we include the indication in the model and then we remove drug to see were they explaining the same variation and what we can see is that the informative of the model dropped substantially when we removed drug but kept why you were Taking the drug headache or osteoarthritis for example so here we can see that that effect of improving the informative of the model was specifically due
to drug right and so now we can say that the drug was significantly associated with this interaction with cognitive decline so that's basically the process and these are the final graphs that we end up with so here we have the score mmsc score so as That goes down that's cognitive decline and we've got month along the x-axis so that's 10 years right there in the non-users we can see this is the average decline and in this one we're modeling someone with mild cognitive impairment so this is somewhat sort of pre-alzheimer's what would happen if they
started taking these drugs the theory here we can see non-users declined at This rate approximately declined 10 points in 10 years whereas the clovernet uses decline at this rate approximately declining about three and a half points in ten years so we had this very significant effect and the clovernecked users were associated with a slower decline a slower cognitive decline a slower progression of alzheimer's disease now critically the other non-steroidal anti-inflammatories like ibuprofen which are prescribed for the Same reasons right so arthritis and headache predominantly they did not see a significant reduction decline so even though
they had lower prevalence which i mentioned in the beginning the progression of the disease did not change with ibuprofen naproxen aspirin cerlicoxan any of these drugs that don't inhibit nlrp3 so ibuprofen is performing almost exactly the same as a non-user there so here we can see we've got all these Drugs here inhibit cox only diclovanec and this dataset inhibited nlrp3 and then insanely only that drug was associated with a slower cognitive decline what i love about this is the a priori hypothesis the hypothesis that we've established from the animal models before we went into the
clinical data analysis the cohort data analysis i should say was so specific we were saying if it is xeno rp3 only declovinate should be Associated with a slower cognitive decline and the other one should not if it is xenolrp3 that is inducing the damaging inflammation in alzheimer's disease and that very specific hypothesis sort of you know it fleshed out in the day once we did the analysis that's exactly what we saw which was another crazily exciting moment in my career to see what what i've done in the cells what I've done in the animals happen
again in in the human data which was amazing so essentially we followed it through we followed it from cells into animals we actually did a rat model of alzheimer's disease but i didn't want to go over time too much and then we followed that into the human data so we did the drug screen in the cells we then took that to a mouse model as well as a rate model and then we looked at it in the human data and i think this is such A powerful workflow and i think we've got a really strong
case now to do a clinical trial on these drugs so thank you very much if you have any questions pop a comment below like and subscribe to the channel and or you can flip me an email or check out my website which is www.jackorty.com it's right there there's my website and you can follow me on twitter if you want as well it won't be as informative Follow me on twitter is checking out my website there thank you very much and thank you for listening