well greetings everyone and welcome to the ekg case for the week of april 1st 2013. got a great case for you and this week's case was sent to us all the way from chile by dr nicholas pineda uh and by the way as long as we're talking about chile i want to let you know about a fantastic conference that's coming up august 28th through 30th in santiago chile and some of the speakers are the likes of dr mel herbert stewart squadron billy mallon and a handful of other really excellent speakers it's going to be a
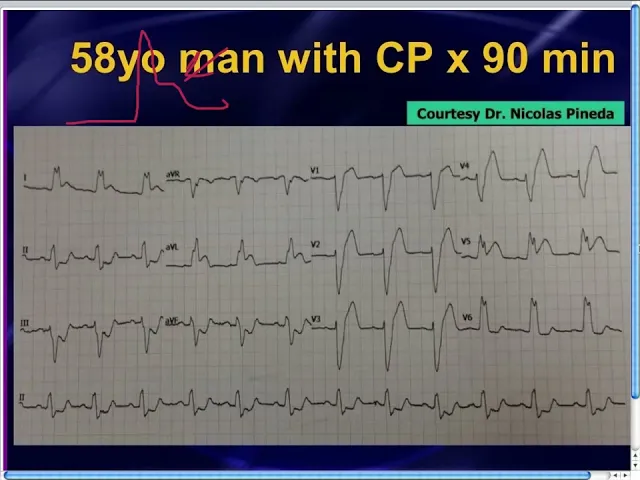
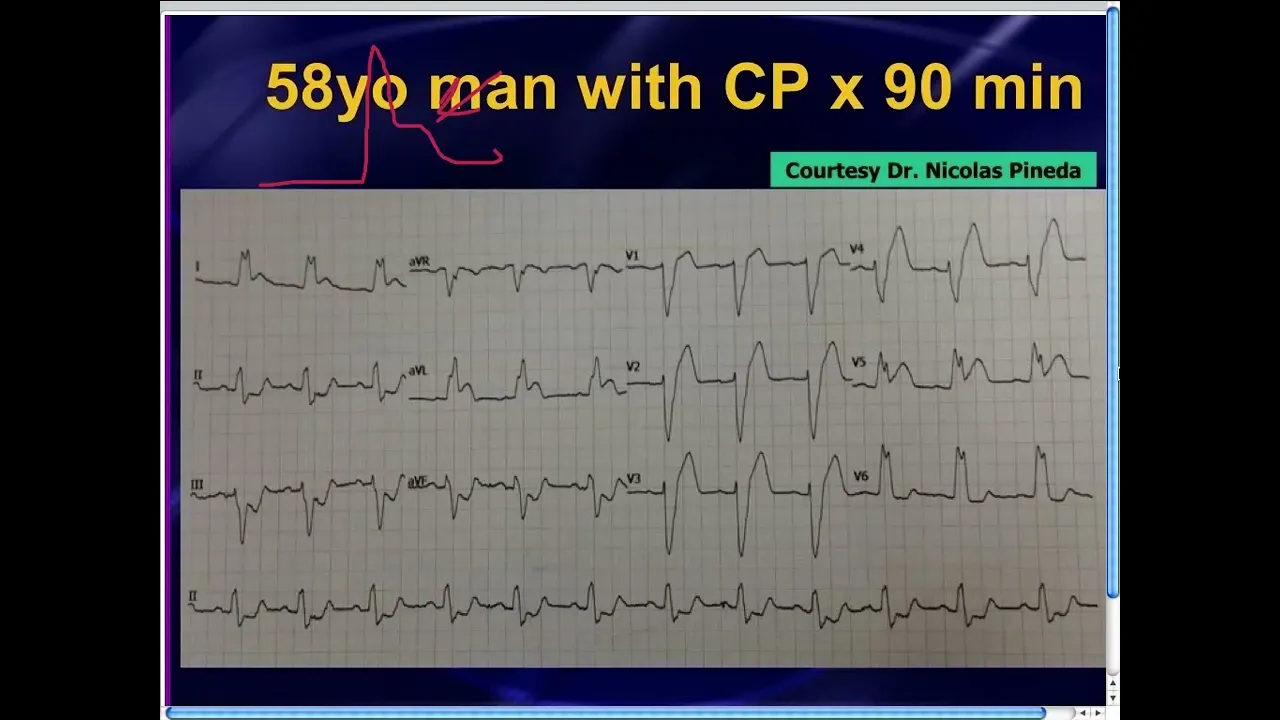
fantastic conference and i don't know what the website is but if i can find that out for you i'll be happy to share it with anyone just email me and i'm looking forward to attending that conference as well but anyway back to the ekg case that dr pineda has sent us he had a 58 year old man who had presented to the emergency department complaining of chest pain for about an hour and a half and one of the things that you'll notice right up front is that there is a left bundle branch block pattern and
what does that mean well when somebody's got chest pain in the left bundle we've all learned that you can't read any ischemia in the presence of a left bundle well if you've been keeping up with the literature unlike perhaps some of your consultants no names to be mentioned well you know that you can actually in many cases read ischemia in the presence of a left bundle not always but in some cases you can so that's what we're going to spend time talking about before we get into that we first of all have to define a
left bundle so a left bundle branch block pattern what are the criteria for a left bundle first of all you have to have a wide qrs it's got to be at least 120 milliseconds all right lead v6 typically has these rabbit ear pattern you see an rsr prime type of pattern maybe often present in v5 as well and typically in lead v1 you've got a little r deep wide s wave sometimes you just have this q s type of pattern in v1 and that usually persists out in v2 and v3 another important finding that you
should use to define a left bundle is you know left bundle is such a powerful leftward force you really should not have any q waves in those lateral leads you should just have big r waves maybe an rs wave but certainly a big giant r wave without any q waves in the lateral leads if you ever see a small q wave even a tiny q wave in those lateral leads a lot of authors will tell you that that obviates the diagnosis of a left bundle and you have to call it just a non-specific conduction delay
one of the other important findings of a left bundle that relates to ischemia is this thing that we refer to as the rule of appropriate discordance what that means is that every time the qrs complex primarily goes up the j point in st segment should be below the baseline all right actually i didn't draw that too well let me try that again qs goes up and the j point should be below the baseline well that almost looks like ditch toxicity but anyway you get the point so qrs for example in lead one take a look
at lead v1 or rather lead one the qrs goes up and so the j point and st segment are a little bit below the baseline that's normal isoelectric's okay also but it should be in the opposite direction discordant every time the qrs complex goes down for example in lead avr the j point or st segment should be a little bit elevated isoelectric is okay but it should be in the opposite direction once again and that applies for all 12 leads all right if you lose that discordant relationship you have to worry that the person may
be having some ischemia in other words if the cures goes up and the st segments also elevated or concordant same direction or if the cures goes down and the st segment is depressed in the same direction or concordant in the same direction well these findings were all first described back in 1996 by a cardiologist by the name of elena scarbosa and we now refer to this as the scarbosa criteria what she described was a very very nice predictive model for predicting when a person with the left bundle is having an acute mi essentially a stemi
equivalent what she said and i'll refer to these as scarbosa a b and c scarbosa criteria a essentially said if the qrs goes up and there's st segment in the same direction or concordant in the same direction person's having an mi scarbosa criteria b really just applied to v1 v2 or v3 what she said is the qrs complex goes down and the st segment is depressed in the same direction concordant depression then that predicts an acute mi and then scarbosa criteria c essentially said that if the cures goes down and there's elevation normally elevation is
okay but if there's excessive elevation of more than five millimeters all right so in other words this elevation right there is more than five millimeters if you see more than five millimeters of st elevation there then that was predictive of an mi unfortunately that had lower specificity so we oftentimes don't use that but scarbosa criteria a concordant st elevation scarbosa criteria b concordant st depression in v1 v2 or v3 these have more than 90 predictive value for telling you this person is having an mi and if you have consultants that don't believe you just show
them this article oftentimes a cardiologist may not be up with this even though you would think so a lot of them don't know about this or don't believe in it show them their literature make them read their own stuff this is the journal of the american college of cardiology this is the most recent really nice review on this topic i think you should have this in your back pocket and stuff a copy of this into the lab coat of anybody out there who doesn't believe that this garbosa criteria are useful it's a really great review
article by the cardiologist for the cardiologist in their main journal all right so just show it to them you've got to know scarborough criteria it's on the em boards it's on the cardiology boards you've got to know about this and when you see scarbosa a or b you've got to act on it let's go back to dr pineda's case 58 year old man with chest pain scarbosa criteria a is present in a handful of leads remember scarborough criteria a said if the cures goes up and the j point and st are in the same direction
and you see this in lead one and in lead avl and in lead v5 in three leads by the way they do not need to be contiguous this works even if you see it in one isolated lead in this case you see it in three leads qrs complexes are going north and the j point and st segment are in the same direction in lead one in lead avl and there in lead v5 this person's having an mi there is no scarbosco criteria b you recall scarbosco criteria b would have said that in leads v1 v2
or v3 if the crest complex is going down and there is st concordant st segment depression you'd have to worry about that and you do not see that in v1 v2 or v3 by the way you notice that there is concordant st segment depression in leads 3 and avf some people will probably be looking at that and saying well there's concordant st depression qs is going down and the j point and st segment are below the baseline in the same direction doesn't that constitute an acute mi also well what i would say is that it
constitutes a significant concern but recall recall that scarbosa only talked about concordant st depression in v1 v2 or v3 you can't really talk about it in those other leads and so those don't technically constitute an acute mi but i would certainly worry quite a bit about it and no surprise to anybody who actually keeps up with the literature and knows about this this patient went to the cath lab and had a 100 percent lady occlusion if somebody had simply looked at this 12 lead and said up it's a left bundle we can't tell anything this
person could very well have died but fortunately dr pineda looked at the 12 lead he knew scarborough's criteria he saved a life good job all right so just to finish things up please remember again people still talk about this myth a qmi in the presence of a left bundle can sometimes be diagnosed not always but sometimes you can diagnose it based on the scarbosa a or b and remember what scarborough criteria a is concordant st segment depression or i'm sorry concordia st segment elevation scarbosa criteria b is that concordant st segment depression all right so
when you see concordant st segments in qs complexes you've got to worry about that patient even though they have a left bundle branch block pattern and for those people out there that have not typically believe that you can diagnose ischemia or stem equivalent in the presence of a left bundle what you do is tell them to go read a little bit all right so again hopefully that was helpful my thanks to dr pineda for sending a fantastic case and for those people that want a little bit more practice with this concept of scarborough criteria we've
done this in the ekg video series a couple of times now last time we did it was july 23 2012 so just go to the ekg website and again it's www.ekg.umem and scroll back to july 23rd you get some more practice and i hope that's helpful remember reading ekgs can save lives so get good at it and i look forward to talking to all of you next week dr pineda thanks for sending a great case